
Abstract
Background:
Recurrent shoulder instability results from overuse injuries that are often associated with athletic activity. Timely diagnosis and treatment are necessary to prevent further dislocations and secondary joint damage. In pediatric and adolescent patients, insurance status is a potential barrier to accessing timely care that has not yet been explored.
Purpose:
To examine the effect of insurance status on access to clinical consultation, surgical intervention, and surgical outcome of pediatric and adolescent patients with recurrent shoulder instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We conducted a retrospective review of pediatric and adolescent patients who were treated at a single tertiary children’s hospital for recurrent shoulder instability between 2011 and 2017. Patients were sorted into private and public insurance cohorts. Dates of injury, consultation, and surgery were recorded. Number of previous dislocations, magnetic resonance imaging (MRI) results, surgical findings, and postoperative complications were also noted. Delays in care were compared between the cohorts. The presence of isolated anterior versus complex labral pathology as well as bony involvement at the time of surgery was recorded. The incidences of labral pathology and secondary bony injury were then compared between the 2 cohorts. Postoperative notes were reviewed to compare rates of repeat dislocation and repeat surgery.
Results:
A total of 37 patients had public insurance, while 18 patients had private insurance. Privately insured patients were evaluated nearly 5 times faster than were publicly insured patients (P < .001), and they obtained MRI scans over 4 times faster than did publicly insured patients (P < .001). Publicly insured patients were twice as likely to have secondary bony injuries (P = .016). Postoperatively, a significantly greater number (24.3%) of publicly insured patients experienced redislocation versus the complete absence of redislocation in the privately insured patients (P = .022).
Conclusion:
Public insurance status affected access to care and was correlated with the development of secondary bony injury and a higher rate of postoperative dislocations. Clinicians should practice with increased awareness of how public insurance status can significantly affect patient outcomes by delaying access to care—particularly if delays lead to increased patient morbidity and health care costs.
Shoulder instability has become increasingly common in the pediatric and adolescent population, as these patients have become more involved in athletic competition. 10 Shoulder instability results from acute traumatic events as well as overuse injuries from repetitive microtraumas due to athletic activity. 11 After the initial injury, patients are at high risk of redislocation, with reported rates of up to 100% in skeletally immature patients. 12 Given that recurrent shoulder instability can lead to degenerative arthropathy, timely diagnosis and treatment are necessary to prevent secondary joint damage and further dislocation, preserve function, and restore athletic activity, especially in high-risk, active pediatric and adolescent patients. 17
Recurrent shoulder instability is strongly associated with secondary injuries, such as bony Bankart and/or engaging Hill-Sachs lesions. These osseous lesions often develop as a result of traumatic anterior shoulder dislocations, especially in the setting of high-impact injuries sustained in contact sports. Furthermore, these lesions can worsen with recurrent dislocations from repetitive microtraumas, such as those sustained in athletic activity. 3 Development of secondary joint damage also predisposes patients to more dislocations. For example, Olds et al 14 reported that 100% of observed pediatric patients with radiographic evidence of Hill-Sachs lesions had episodes of recurrent instability. Moreover, osseous glenohumeral lesions can lead to surgical complications, as the amount of bone loss directly affects surgical outcomes. 7 Given the strong association of the development of these osseous lesions with recurrent dislocations, timely treatment is necessary to prevent secondary morbidity, avoid surgical complications, and prevent the need for secondary procedures or larger, index open operations.
Insurance status is often a barrier to receiving timely care. Existing literature has shown significant differences in access to care for privately versus publicly insured adult patients with orthopaedic-related pathology, indicated by delayed diagnosis and treatment. 2,5,15 For pediatric and adolescent patients with shoulder instability, however, insurance status has not yet been studied as a risk factor for delayed care. The purpose of this retrospective cohort study was to analyze whether the insurance status of pediatric and adolescent patients with recurrent shoulder instability affects the time from injury to diagnosis and surgical intervention as well as the incidence of secondary bony injuries. It was hypothesized that pediatric and adolescent patients with public insurance would face delays in care and in surgical intervention, leading to a greater incidence of secondary bony injury when compared with that of privately insured patients. In addition, it was hypothesized that there would be a higher rate of surgical failure in the public insurance cohort, manifesting clinically as a higher rate of postoperative redislocation.
Methods
Data Collection
This study was a retrospective review of pediatric and adolescent patients who were treated at a single tertiary children’s hospital for recurrent shoulder instability between 2011 and 2017 by a single, fellowship-trained pediatric orthopaedic surgeon (N.K.P.) specializing in sports medicine. Approval from the institutional review board was obtained. Patients were included in the study if they presented with recurrent shoulder instability and underwent surgical intervention for their injury. Patients were excluded from the study if they presented for revision surgery after having their primary surgery performed by another surgeon.
A review of the electronic medical records was performed to obtain patient demographic information including date of injury, date of presentation to clinic, date of magnetic resonance imaging (MRI), and date of surgery, which were recorded as continuous variables. MRI was performed at our institution. The number of previous dislocations was recorded categorically as none, single, or multiple (defined as having >1 dislocation). In this study, we included patients with multiple frank dislocations as well as those who reported recurrent subluxation rather than frank dislocations that were documented in the chart. Thus, patients who were recorded as having zero or 1 previous dislocation fell under the category of having recurrent subluxations. All patients who reported recurrent subluxations had unidirectional rather than multidirectional instability on physical examination.
Insurance status (public — including uninsured status — or private) was recorded as a categorical variable. Upon beginning care at this safety-net hospital (no preference for care based on insurance), uninsured patients were automatically enrolled in public insurance programs, so they were included in the public insurance cohort. The presence of anterior only versus complex labral pathology as well as bony involvement (bony Bankart, engaging Hill-Sachs, glenolabral articular disruptions) at the time of surgery were recorded as binary variables based on operative report findings. Complex labral pathology was defined as any labral pathology that did not only involve the anterior labrum (eg, posterior labral tears). Complex labral pathology also included the presence of additional soft tissue injury, such as rotator cuff tears, biceps pathology, and loose bodies. Finally, follow-up notes were reviewed to determine the rates of repeat dislocation and repeat surgery. The mean follow-up was 28.2 ± 16.2 months. All patients presented for at least 1 in-person postoperative follow-up visit. To ensure accurate reporting of the redislocation rates, all patients were asked as part of the postoperative protocol to contact our office if they had a repeat instability event. We also had access to an integrated feature within our electronic medical records that allowed us to look back to see if they presented to another hospital system.
Surgical Technique
All patients underwent arthroscopic surgical stabilization in the lateral decubitus position. Given that no patients had glenoid bone loss >25%, no primary open procedures were indicated. Glenoid bone loss was determined via MRI scans and was confirmed intraoperatively. Patients underwent standard Bankart repair using a combination of knotless and knotted anchors to both repair and shift the capsulolabral complex. If patients demonstrated an off-track Hill-Sachs lesion, a remplissage procedure was performed as well using a double-loaded bioabsorbable suture anchor (Smith & Nephew). Patients were not allowed to return to contact sports until at least 6 months after their procedure.
Statistical Analysis
The Welch 2-sample t test, which assumes unequal variance between the comparison groups, was used to determine if there was a statistically significant difference in time from injury to clinic presentation, injury to diagnostic MRI, injury to surgery, clinic presentation to diagnostic MRI, and MRI to surgery between publicly and privately insured patients. The Pearson chi-square test was used for categorical and dichotomous variables to determine if there was a statistically significant difference in the number of previous dislocations and the presence of anterior versus complex labral pathology and bony involvement, as well as repeat dislocation and repeat surgery rates between the public and private insurance cohorts. Calculated P values <.05 were considered statistically significant. With regard to the study’s sample size, with an alpha of .05 and power (1-beta) of 80%, there was sufficient power to find a 10-day difference between the 2 groups assuming an enrollment of at least 16 patients in each group.
Results
Demographics
A total of 55 patients were identified as having recurrent shoulder instability, for which they underwent subsequent surgical intervention between 2011 and 2017. There were 37 patients in the public insurance cohort and 18 patients in the private insurance cohort. Both cohorts were active, engaging in athletic activities including wrestling, baseball, volleyball, football, mountain biking, snowboarding, soccer, basketball, lacrosse, rugby, softball, crew, and skateboarding. Mechanisms of injury included collision, trauma, and fall on an outstretched hand. The mean age at the time of injury was 14.81 ± 1.68 years (range, 10.22-18.35 years). The mean age at the time of surgery was 16.40 ± 1.67 years (range, 11.99-19.96 years).
Access to Care
There were statistically significant differences in the time from injury to clinic presentation, injury to diagnostic MRI, and injury to surgery between the private and public insurance cohorts (Figure 1). Privately insured patients were evaluated by clinicians nearly 5 times faster than were publicly insured patients (mean, 85.61 days vs 402.38 days; P = .000009). Additionally, privately insured patients received MRIs >4 times faster than did publicly insured patients (mean, 99.11 days vs 431.97 days; P = .0001). Thirteen patients presented with MRI scans: 8 of 37 patients (21.6%) in the public cohort and 5 of 18 patients (27.8%) in the private cohort. The time from injury to surgery was also significantly faster for privately insured patients versus publicly insured patients (mean, 226.44 days vs 561.38 days; P = .0066). There was no statistically significant difference between the 2 insurance cohorts for the time from clinic presentation to diagnostic MRI and time from MRI to surgery (Figure 2). The difference in the number of previous dislocations before the initial consultation between the 2 insurance cohorts was also statistically significant (P = .043), with a higher incidence of multiple previous dislocations among publicly insured versus privately insured patients.
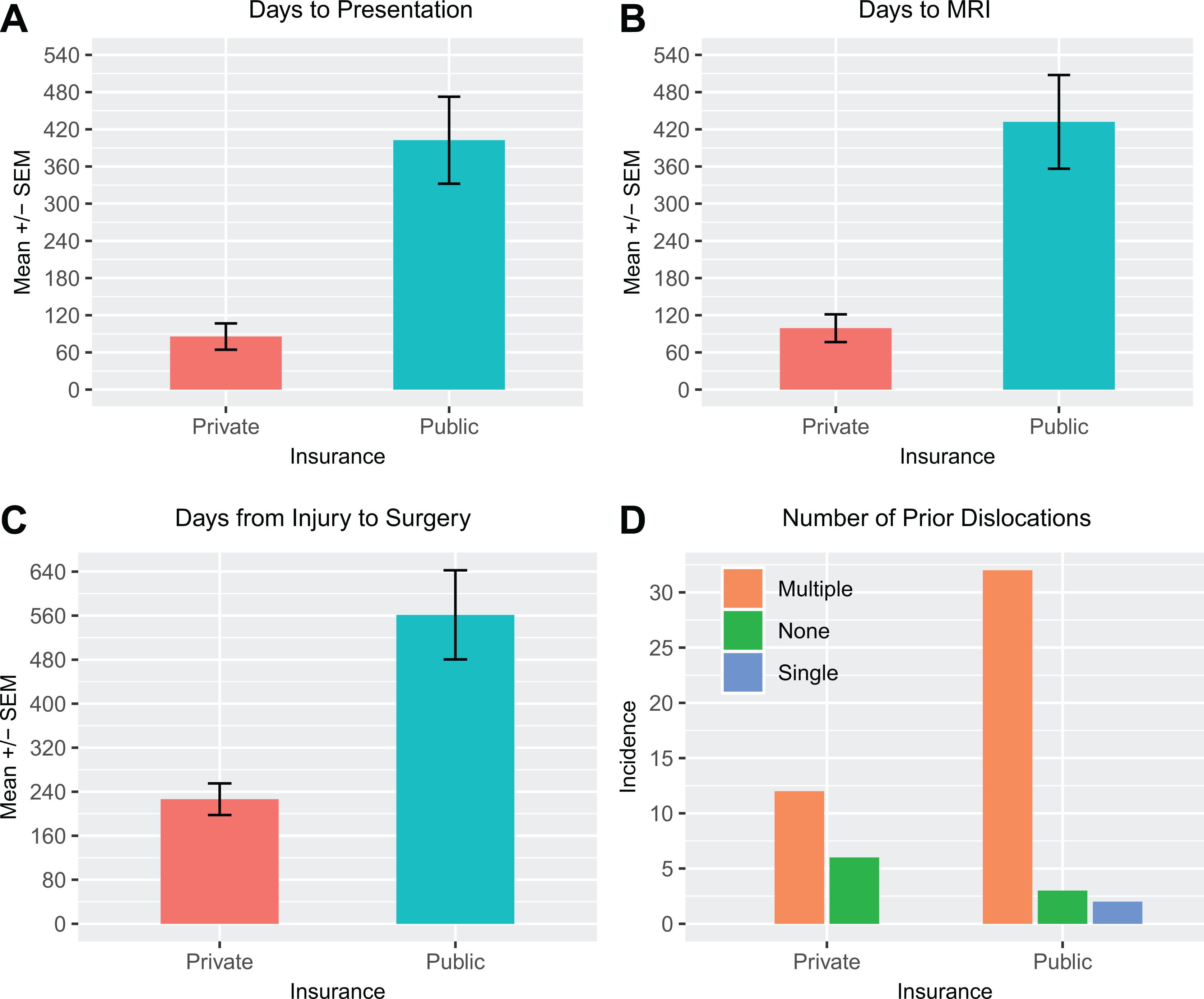
Comparison of access to care between public and private insurance cohorts, including mean days from (A) injury to clinic presentation, from (B) injury to diagnostic magnetic resonance imaging (MRI), and from (C) injury to surgery. (D) Comparison of the number of previous dislocations before presenting to the clinic is also shown. These differences were statistically significant for all parameters shown (P < .05).
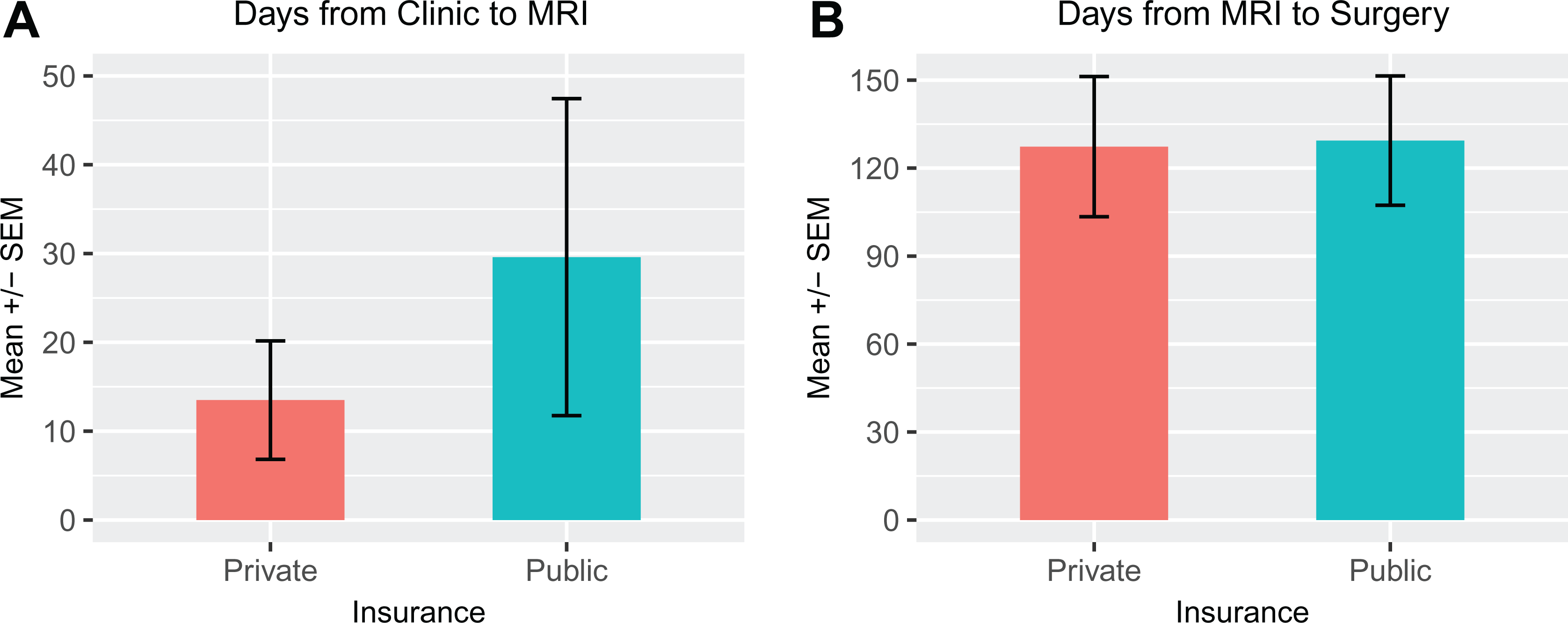
Comparison of mean days from (A) clinic presentation to diagnostic magnetic resonance imaging (MRI) and from (B) MRI to surgery between public and private insurance cohorts. There was no statistically significant difference between the 2 cohorts for these parameters (P > .05).
Secondary Injuries
There was a statistically significant difference between the insurance cohorts for the incidence of bone involvement; publicly insured patients were twice as likely to have secondary bony injuries (including bony Bankart deformities, engaging Hill-Sachs deformities, glenolabral articular disruptions) when compared with privately insured patients (P = .016). There were no statistically significant differences between the insurance cohorts for the incidence of anterior only versus complex labral pathology (P = .588) as seen at the time of surgery (Figure 3).

Comparison of (A) secondary bony injury and (B) labral pathology between public and private insurance cohorts. Secondary bony injuries included bony Bankart lesions, engaging Hill-Sachs lesions, and glenolabral articular disruptions. Complex labral pathology included any labral pathology that did not involve the anterior labrum (eg, posterior labral tears) and soft tissue injury, such as rotator cuff tears, glenohumeral ligament tears, loose bodies, and so forth. These differences were statistically significant for both parameters shown.
Repeat Dislocation and Repeat Surgery
Postoperatively, the incidence of repeat dislocation for publicly insured patients was statistically significant (24.3% compared with 0.00% for privately insured patients; P = .022). There was no statistically significant difference in the rates of repeat operation for publicly versus privately insured patients (8% and 0%, respectively; P = .214) (Figure 4). Many publicly insured patients elected not to undergo revision surgery even when they had a repeat instability event.

Comparison of postoperative complications between public and private insurance cohorts. These differences were statistically significant for the (A) incidence of repeat dislocation (P = .022) but were not statistically significant for the (B) incidence of repeat operation (P = .214).
Discussion
Our results demonstrated that publicly insured pediatric and adolescent patients with recurrent shoulder instability face significant delays in obtaining care when compared with privately insured patients. Publicly insured patients waited nearly 5 times longer from the time of injury to the initial clinic consultation than did privately insured patients; however, the difference in the wait time between the 2 cohorts from the clinic consultation to MRI and from MRI to surgery was not statistically significant.
Delays in access to care for pediatric and adolescent patients with recurrent shoulder instability can lead to the development of secondary injuries including bony Bankart and engaging Hill-Sachs lesions. The development of these bony lesions is associated with an increased risk of treatment failure and recurrent instability by taking an injury that may be soft tissue in nature after initial dislocation and transforming it to a complex soft tissue and bony injury with a risk of repetitive instability. Our study demonstrated a statistically significant correlation between insurance status and secondary injury development; publicly insured patients were twice as likely to develop secondary bony injuries compared with privately insured patients. The secondary joint damage associated with subsequent shoulder dislocations follows another observed outcome in orthopaedic pathology where delays in stabilization of anterior cruciate ligament (ACL) injuries can lead to cartilage and meniscal damage. 1,4,6,8,13
Given the significant secondary injury that can result from delayed care, it is critical to investigate barriers to accessing care, such as insurance status. Previous studies have assessed the effect of insurance status on wait time for adults with orthopaedic injuries. Baraga et al 2 reported that in 80 patients with ACL injuries, the time from injury to diagnosis was 14 days for privately insured patients, 56 days for publicly insured patients, and 121 days for uninsured patients, while Khanna et al 9 identified a statistically significant delay from injury to MRI diagnosis for publicly versus privately insured pediatric and adolescent patients with ACL injuries. Another study demonstrated nationwide disparities in access to care for publicly/uninsured pediatric patients with orthopaedic injuries by reporting a significantly lower percentage of orthopaedic surgeons who accept Medicaid for payment. 16
Yet, there has been limited examination of how insurance status affects outcomes for pediatric and adolescent patients with recurrent shoulder instability. An investigation of this patient population is particularly warranted, as pediatric and adolescent patients have the highest activity demand on the shoulder joint given their high participation in athletic competition. Our findings of differences in wait times from injury to consultation, MRI, and surgery for publicly versus privately insured patients suggest that in this particular system, delayed access of entry to the care system had the most significant effect on the patient’s time course of treatment. Once patients were seen and evaluated, the wait time from consultation to subsequent segments of their treatment (MRI and surgery) was not significantly different between the 2 cohorts. Thus, delays due to authorization are not necessarily the root cause of care access, but rather ability to access orthopaedic surgeons within the community after injury occurrence is where further intervention can be made.
We did not examine the cohort of patients who directly presented to our safety-net hospital after injury in a formal statistical fashion because the information with regard to their previous presentation to other institutions was not consistently recorded in the chart. However, from our subjective experience, even given immediate presentation to our clinic, there were still delays in care that could not be accounted for simply by initial presentation to another institution. We hypothesize that additional factors affecting access to care include the ability to attend appointments (ie, time off work, transportation issues, child care), availability of postoperative physical therapy, and distance from the clinic. In order to effectively address these additional barriers, providers should be aware that these factors affect patient populations disproportionately. By taking the time to ask patients and their parents about anticipated scheduling challenges to minimize difficulties in follow-up in a nonjudgmental, nonstigmatizing manner at each visit, providers can help minimize disruptions in accessing care, for example, by employing alternative modes of follow-up, such as telephone or video follow-ups, when feasible. Additionally, differences in postoperative failure rates, marked clinically by repeat dislocation after surgery, suggest that ultimately patients will be better off postoperatively if they can be evaluated earlier.
These results illuminate an existing issue within our health care system where pediatric and adolescent patients, with public and private insurance alike, experience multiple shoulder dislocations before seeking or initiating care. However, patients with private insurance are better able to advocate for themselves in initiating care, as their insurance plan structures often enable them to directly consult an orthopaedic surgeon. In comparison, patients with public insurance must rely on referral sources for the initial consultation, causing them to wait significantly longer for the initial consultation. The reasons for this are multifactorial: limited access to primary care providers due to a shortage of physicians; primary care provided in emergency department settings; and limited musculoskeletal education in medical school, which may limit primary care/emergency department knowledge of the detrimental effects of multiple dislocations on outcomes. As a result, publicly insured patients sustain multiple repetitive injuries before evaluation at a higher rate than do privately insured patients, which is associated with higher rates of secondary bony injury development. Finally, our data also suggest that the increased delay in time from injury to consultation for publicly insured patients contributes to poorer surgical outcomes with higher rates of postoperative redislocation and reoperation.
Given the poorer surgical outcomes associated with delays in accessing care for publicly insured pediatric and adolescent patients with recurrent shoulder instability, what are practical next steps that can be taken to mitigate the inequalities produced by insurance status? First, awareness on behalf of providers in both inpatient and outpatient settings will help set the stage for future action. For example, when pediatric and adolescent patients present to the emergency department with repeat shoulder dislocation, the next step of care should be providing a referral to an orthopaedic surgeon for further evaluation. This also applies to the outpatient setting when these patients present to primary care physicians in a clinic. Immediate referral after initial presentation to the emergency department or to a primary care physician will increase the likelihood of a positive outcome for the patient, as we have demonstrated the significant clinical consequences of delays in evaluation for these patients. Additionally, from a health system cost standpoint, earlier referrals to the orthopaedic service will reduce overall spending because improved surgical outcomes will require fewer revision surgeries and physical therapy sessions. Furthermore, savings will also trickle down to the patient-caregiver level, as required time absent from work for caregiving for pediatric and adolescent patients will decrease.
One limitation of our study is that it was a retrospective review of a limited sample size of patients. Furthermore, data were collected from a single center. Thus, findings may not be generalizable to different clinical settings and practices. Second, a longer follow-up period could have illuminated further differences in postoperative outcomes and complications (redislocation and reoperation rates). The strengths of our study include that it was a single-surgeon study that took place at a tertiary care center with a large referral base. This consistency controlled for variation seen in multisurgeon settings including surgical indication preferences, scheduling preferences, and operative report documentation style. In addition, the fact that our institution was a safety-net hospital made it possible to delineate the effect of insurance status on care access without the effect of preferential care access at the initiation of orthopaedic care.
Conclusion
In today’s health care landscape, great emphasis has been placed on researching health care inequities, especially on identifying barriers to accessing care. Thus far, there has been limited examination of how insurance status affects access to care for pediatric and adolescent patients with recurrent shoulder instability. Our findings demonstrate that public insurance status indeed affects access to care, leading to significant delays from injury to consultation, contributing to a potentially higher incidence of secondary bony injury associated with multiple repetitive injuries. Finally, these delays establish an association with greater clinical failure rates as indicated by higher rates of postoperative repeat dislocation. Although it remains to be seen whether our results are generalizable, our study findings warrant further investigation with multicenter studies. In the meantime, clinicians in both inpatient and outpatient settings should practice with increased awareness of how public insurance status can significantly affect patient outcomes by delaying access to care.
Footnotes
Final revision submitted April 12, 2020; accepted May 8, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.K.P. has received educational support from Evolution Surgical and consulting fees from OrthoPediatrics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from UCSF Benioff Children’s Hospital Oakland (ID No. 150430E).