
Abstract
Anatomic reconstruction of the lateral ligamentous ankle complex with an autograft is indicated as a surgical approach in chronic ankle instability management. This approach benefits ankles deficient in ligamentous support and those with greater occupational or sporting demands. Autograft choice varies in clinical practice and is driven by surgeon’s choice and patient-specific ankle demands. Current literature does not favor any particular autograft with respect to functional outcomes or postoperative complications. This review systematically compares common autografts through patient-reported outcome measurements (PROMs) and radiographic assessments. A literature search was performed using Ovid MEDLINE and PubMed databases. Studies were screened against inclusion and exclusion criteria and selected studies were critically appraised using Mixed Methods Appraisal Tool 2018. Preoperative and postoperative values of PROMs and radiographic outcomes were extracted, and the percentage change indicated intervention effectiveness. One-way analysis of variance was used to ascertain any statistical significance between the autografts. A total of 20 studies were included comprising 734 patients and 738 ankles. Six different autografts (gracilis, extensor digitorum longus, bone-patellar tendon, semitendinosus, anterior half of peroneus longus, and anterior half of peroneus brevis), 3 PROMs (the American Orthopaedic Foot and Ankle Score, visual analog scale, and Karlsson-Peterson scale), and 2 radiographic assessments (anterior talar translation and talar tilt) were analyzed. Peroneal tendons showed superior PROMs and radiographic assessments, though not statistically significant, with also the lowest complication rates. Autografts with a distal harvest sites, such as gracilis or bone-patellar tendon-bone, carry higher risks of harvest-related and nerve injuries compared with other autografts.
Keywords
“A closer analysis of postoperative complications and autograft properties reveals potential factors that might favor a surgeon’s choice of a particular autograft over the other.”
Introduction
Lateral ankle sprains are the most common acute musculoskeletal injury, with its prevalence being especially high in physically active people. 1 The initial sprain carries a risk of reinjury among which 20% to 40% result in a chronic ankle instability (CAI). Chronic ankle instability encompasses continuous joint instability, recurrent sprains, limited range of motion, reduced neuromuscular control, and muscle weakness, overall leading to a cumulative decline in the ankle function 2 and underlying degenerative changes in the cartilage. 3
The primary management of CAI includes nonoperative interventions ranging from strength and balance training programs to more comprehensive multicomponent rehabilitation plans. 4 A surgical intervention is indicated after a failure in symptomatic improvement following 3 to 6 months of aforementioned nonoperative management. Surgical procedures for CAI can be divided into 3 distinct groups: anatomic repair, nonanatomic reconstruction, and anatomic reconstruction. 5
Anatomic repair uses existing ligamentous tissue to regain the ankle stability. Broström procedure, with oftentimes Gould modification, has been considered a gold standard surgical repair approach.1,6 However, ankles characterized by attenuated or deficient ligamentous tissue and concomitant local tissue scarring were shown to profit from an anatomic reconstruction using a free tendon graft to adequately restore the anatomy and thus ankle functionality. 7
Anatomic reconstruction was also proven to benefit high demand ankles in either occupational or sporting activities. 3 Reconstruction can be performed using an either autograft or allograft, with no clinical evidence of superiority of one over the other. 8 The vast research on anterior cruciate ligament (ACL) reconstruction highlighted the relevant advantages and disadvantages of graft choices which are applicable to ankle ligament reconstruction. 9 Expected-value decision analysis of patients undergoing ACL reconstruction revealed aversion to allografts. 6 Regardless of an absence of secondary incision at the harvesting site and thus prolonged theater time seen in case of autografts, allografts are associated with potential disease transmission, risk of immunogenicity, higher cost and varied availability.9,10 Therefore, recent years had demonstrated an established use of autografts in lateral ankle ligamentous complex reconstruction. 10
The choice of autograft varies greatly among surgeons whereby semitendinosus tendon, gracilis tendon, plantaris tendon, toe extensor tendon, and bone-patellar tendon are some of the most commonly employed. 11 Differing biomechanical properties of distinctive autografts as well as patient-specific ankle demands enable an opportunity for individualistic approach. However, the heterogeneity of autografts, variety of surgical techniques employed, and assortment of different outcome measurements make it challenging to ascertain the evidence on the graft choice. To date, no autograft has shown superiority to others with respect to functional outcomes or postoperative complications.
This review aims to systematically compare the use of common autografts through patient-reported outcome measurements (PROMs) and radiographic assessments including anterior talar translation (ATT) and talar tilt (TT). Patient-reported outcome measurements considered in this study included Karlsson-Peterson scale, visual analog scale (VAS), and American Orthopaedic Foot and Ankle Society (AOFAS). Harvesting an autologous tendon comes at the expense of potentially changing the biomechanics of the affected site. 10 In that regard, this review also aims to highlight any complications associated with a particular autograft choice and evaluate which autograft carries the least “cost” of harvesting.
Methodology
Electronic Literature Search
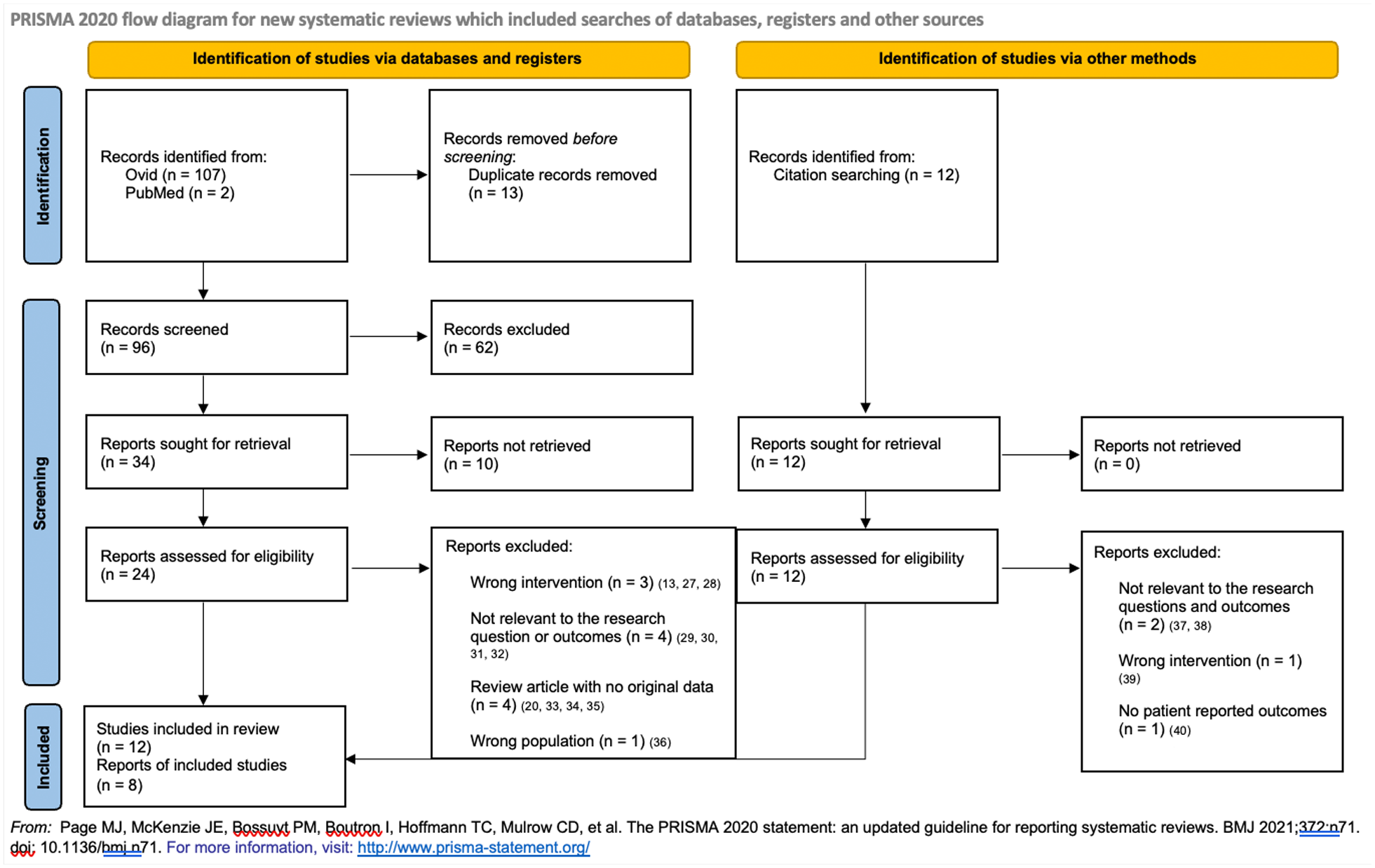
This study was conducted in accordance with the guidelines pertaining the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Figure 1). Electronic databases Ovid and PubMed were searched on the July 4, 2024. The search was conducted using the following key words: “chronic ankle instability,” “reconstruction,” and “tendon graft.” Studies were limited to full-text articles and English language only. Supplementary search methods were employed including cross-reference search of relevant systematic reviews and meta-analyses.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Study Selection
All retrieved articles were independently assessed by 2 reviewers (LB and CFMG). After removing duplicates, titles and abstracts of the articles were reviewed for an appropriate study design and clinically relevant comparable outcomes. Inclusion and exclusion criteria listed below were applied to the remaining articles.
Inclusion criteria
Prospective or retrospective therapeutic studies concerning anatomic reconstruction of lateral ligamentous ankle complex with the autologous tendon graft, either open or arthroscopic.
Studies including participants with CAI diagnosis who underwent at least 3 to 6 months of failed conservative, nonsurgical treatment, and/or failed Broström-Gould procedures, of any age, gender, BMI score, or level of physical activity.
Studies using at least one of the PROMs and/or radiographical reported outcomes with a follow-up of at least 6 months.
Exclusion criteria
Therapeutic studies concerning anatomic repair, nonanatomic reconstruction or anatomic reconstruction with allografts.
Studies involving participants with concurrent rheumatoid arthritis, grade II or above ankle degenerative arthritis, deformities of foot and ankle, systemic diseases, and neuromuscular disorders.
Systematic reviews, cadaveric studies, animal studies, and ex vivo studies.
Critical Appraisal and Quality Assessment
All selected studies were critically appraised using Mixed Methods Appraisal Tool (MMAT) 2018. 12 Each study was independently appraised by the 2 authors (LB, CFMG). In the case of a disagreement, a third author provided input to reach a consensus.
Data Extraction, Synthesis, and Analysis
Preoperative and postoperative values of PROMs and/or radiographic outcomes were extracted and analyzed in the Microsoft Excel. Similarly, any postoperative complications reported in the studies were noted and collated in the Microsoft Excel. Postoperative values of PROMs and/or radiographic outcomes were taken at the final patient follow-up. Percentage change in preoperative and postoperative values was taken as the indicator of intervention effectiveness and served as a basis for further statistical analysis in IBM SPSS software v.29.0.2.0. 13 One-way analysis of variance (ANOVA) test was used to ascertain any statistical significance between the autografts and reveal any superiority in therapeutic effect of a particular autograft.
Results
Study Selection
Figure 1 exhibits the flow diagram of the detailed study selection process. The initial database search yielded 109 articles. After removing duplicates, screening for relevant outcomes and application of inclusion and exclusion criteria, 12 studies were included in the review. In addition, studies identified through citation searching were subjected to the same scrutiny. Of those, 8 studies were included, achieving a total of 20 studies eligible for review. Reasons for exclusion of the remaining articles are listed in Figure 1.
Critical Appraisal and Quality Assessment
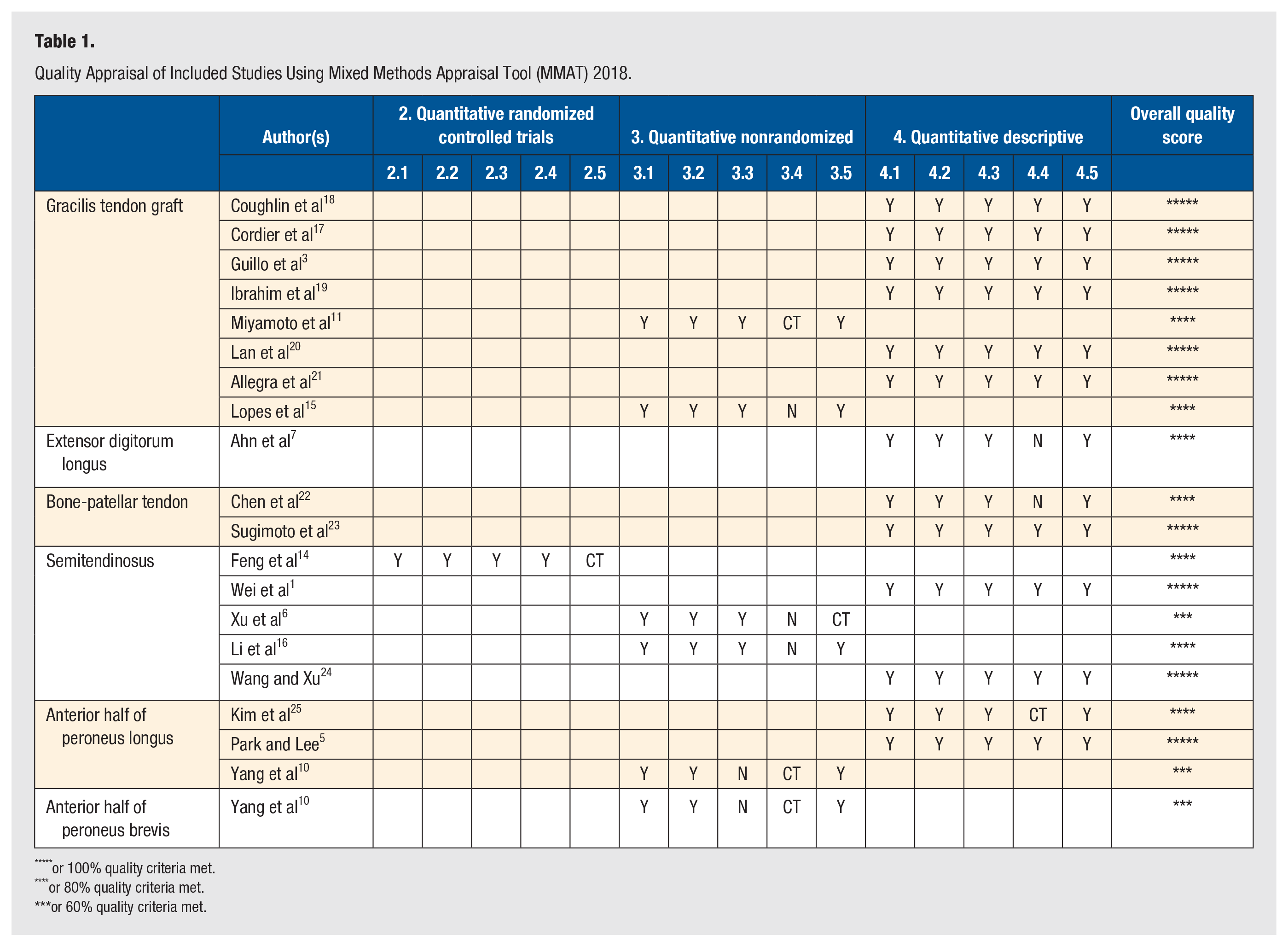
One study 14 was a level II randomized control trial (RCT) without blinding, 5 studies6,10,11,15,16 were level III quantitative nonrandomized studies, and 13 studies1,3,5,7,17-25 were level IV quantitative descriptive case reports or series. Seventeen studies were valued as higher quality papers, whereby 10 of these were fully satisfactory and 4 had some concerns in 1 of the 5 evaluation criteria. Three studies were deemed of lower quality, meeting 60% of the evaluation criteria (Table 1). No studies included met any lower than 60% of evaluation criteria.
Quality Appraisal of Included Studies Using Mixed Methods Appraisal Tool (MMAT) 2018.
or 100% quality criteria met.
or 80% quality criteria met.
or 60% quality criteria met.
Data Extraction, Synthesis, and Analysis
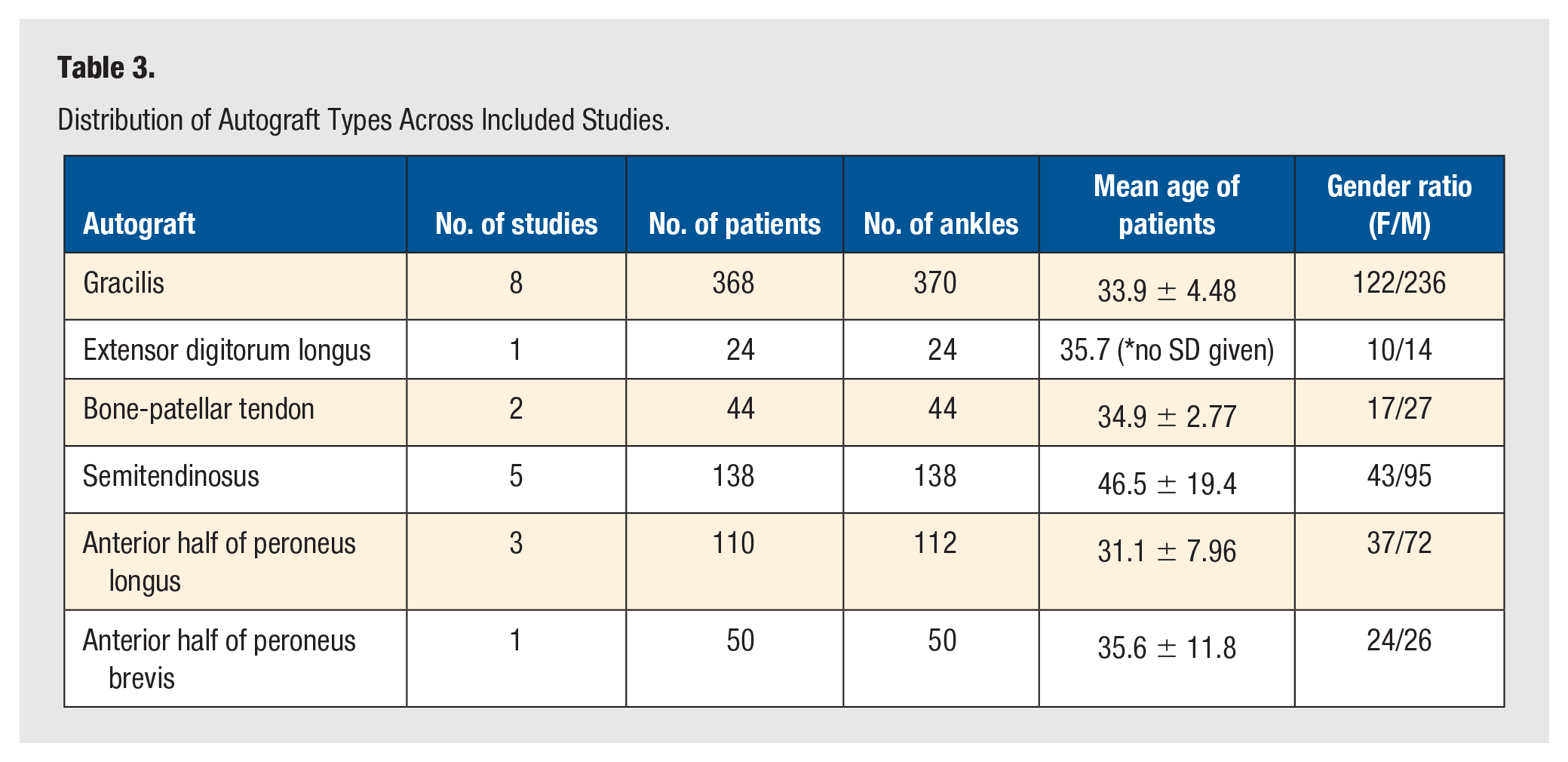
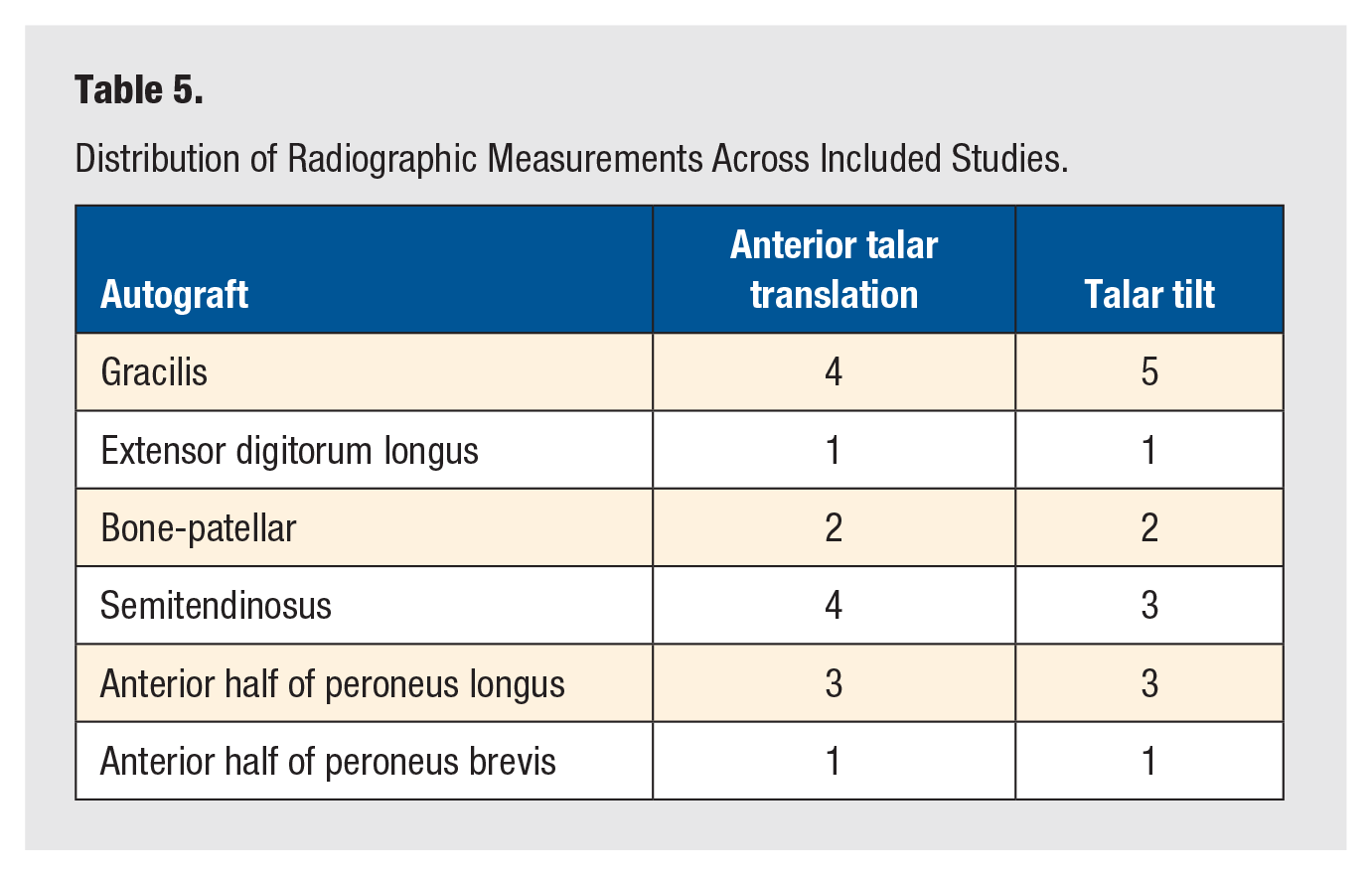
Detailed information about selected studies was extracted and synthesized in Table 2. Overall, a total of 734 patients and 738 ankles were included in the review. Synthesis of included articles revealed 6 different autografts employed across the studies with gracilis being the most frequently used autograft. The distribution of different autografts among patients is shown in Table 3. Studies employed a variety of different PROMs, with most studies using several of them solely or accompanied with radiographic outcomes. To surmount the heterogeneity of the outcomes and enable comparison between the autografts, this review focused on the most frequently used PROMs across studies, AOFAS, VAS, and Karlsson-Peterson scale. The radiographic outcome measurements used in this review included ATT and TT. The distribution of PROMs and radiographic outcomes is demonstrated in Tables 4 and 5, respectively.
Characteristics of Included Studies.
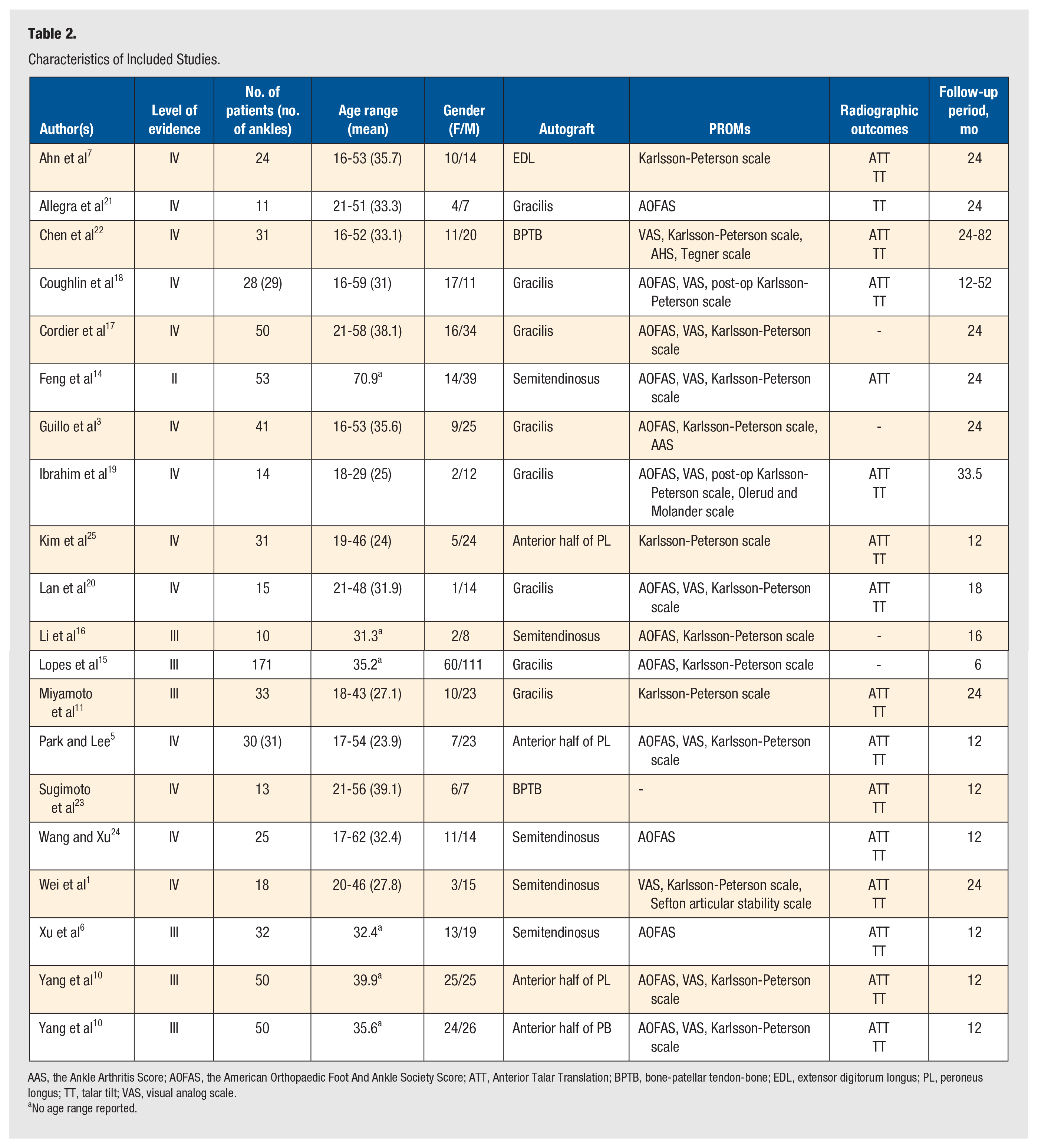
AAS, the Ankle Arthritis Score; AOFAS, the American Orthopaedic Foot And Ankle Society Score; ATT, Anterior Talar Translation; BPTB, bone-patellar tendon-bone; EDL, extensor digitorum longus; PL, peroneus longus; TT, talar tilt; VAS, visual analog scale.
No age range reported.
Distribution of Autograft Types Across Included Studies.
Distribution of Outcome Measurements Across Included Studies.
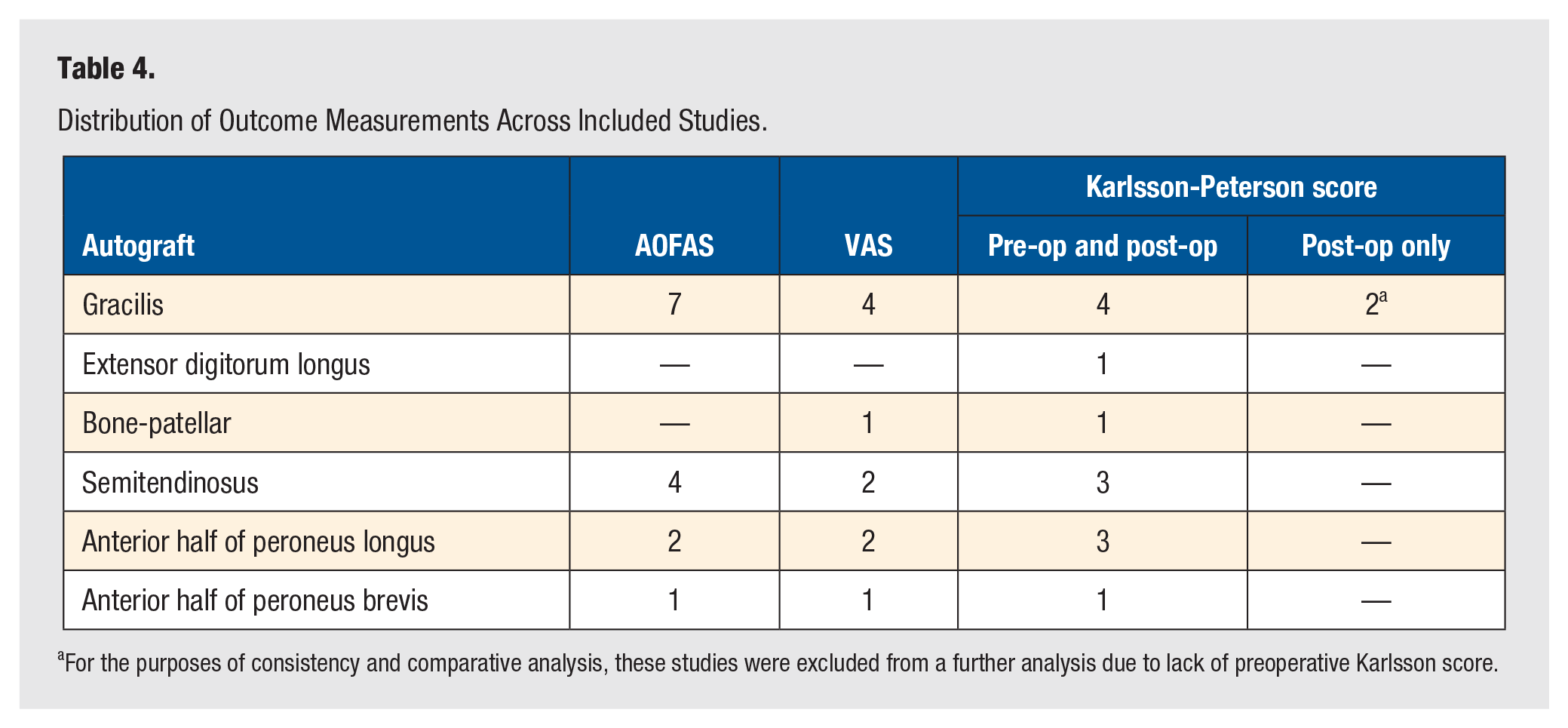
For the purposes of consistency and comparative analysis, these studies were excluded from a further analysis due to lack of preoperative Karlsson score.
Distribution of Radiographic Measurements Across Included Studies.
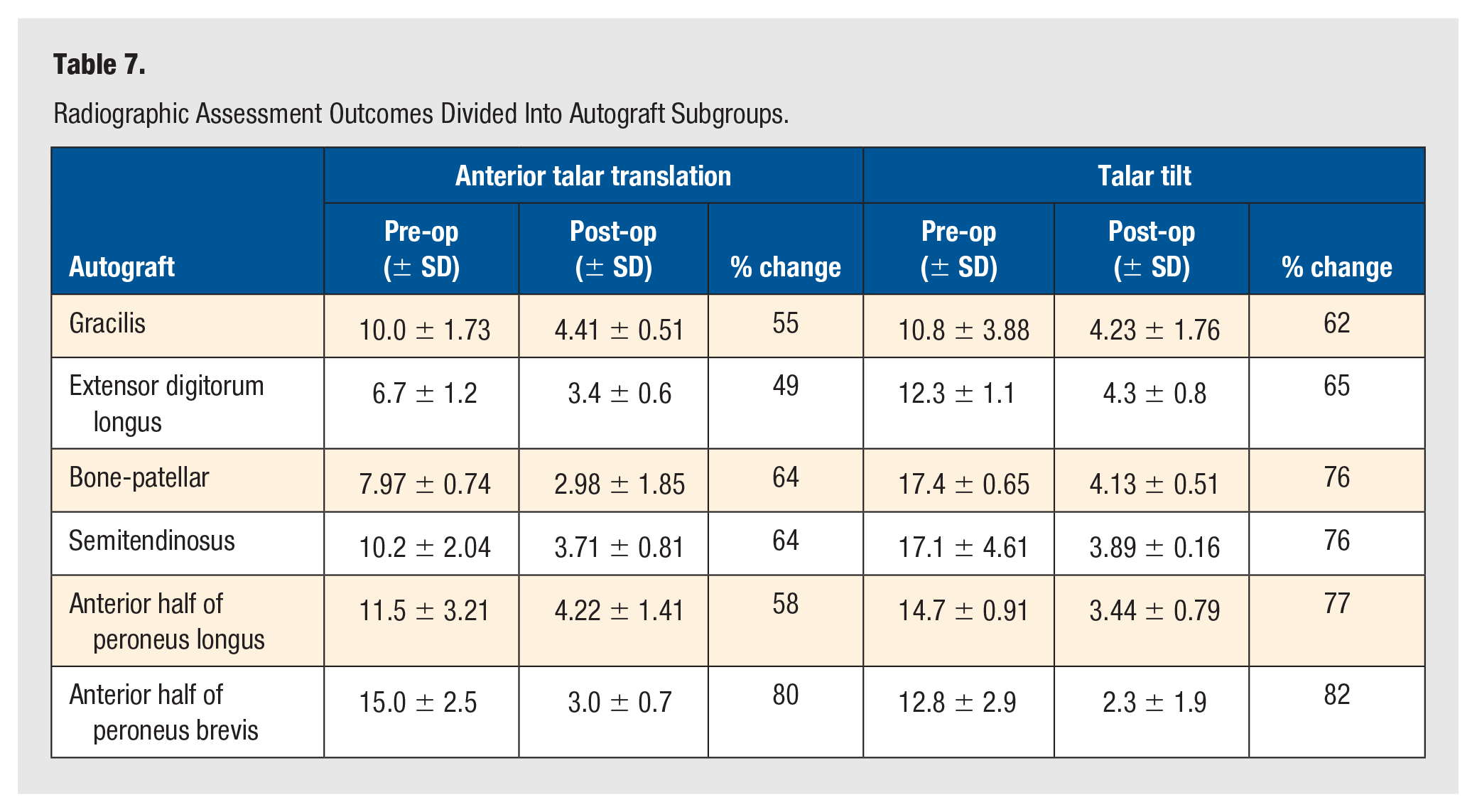
Percentage change in the aforementioned outcomes between the autografts allowed for the quantification of the effectiveness of the intervention with a given autograft and enabled a more robust statistical analysis (Table 6). One-way ANOVA test was performed for each individual PROM as well as radiographic assessment tool. Due to the restriction of the 1-way ANOVA test, autograft subgroups containing less than 2 cumulative mean values in any of the outcome measurements, were excluded from the analysis. In that respect, 1-way ANOVA for AOFAS excluded extensor digitorum longus (EDL), analysis of VAS excluded anterior half of peroneus brevis (PB) and bone-patellar tendon-bone (BPTB), and analysis of Karlsson-Peterson score excluded EDL, anterior half of PB and BPTB. In the instance of radiographic assessments, 1-way ANOVA tests excluded EDL and anterior half of PB. Nevertheless, the data presented below account for all values from the included studies (Table 6). According to PROMs, AOFAS revealed anterior half of peroneus longus (PL) to have the most positive outcomes with reported change of 59%. Studies utilizing VAS reporting found that semitendinosus and anterior half of PB stood out as most effective interventions with an 83% change. Last, interventions reported by Karlsson-Peterson scale showed EDL to be most effective autograft with a 92% change. However, 1-way ANOVA analysis of PROMs revealed no significant difference between autograft groups (P > .05), and thus, no autograft exhibits clinical superiority with respect to patient outcomes. Radiographic outcome measurements revealed anterior half of PB to be the most effective intervention, with 80% and 82% change measured in ATT and TT, respectively. Nevertheless, 1-way ANOVA test performed for radiographic assessments also revealed no significant difference among the autografts of interest (P > .05).
Patient-Reported Outcome Measurements Divided Into Autograft Subgroups.
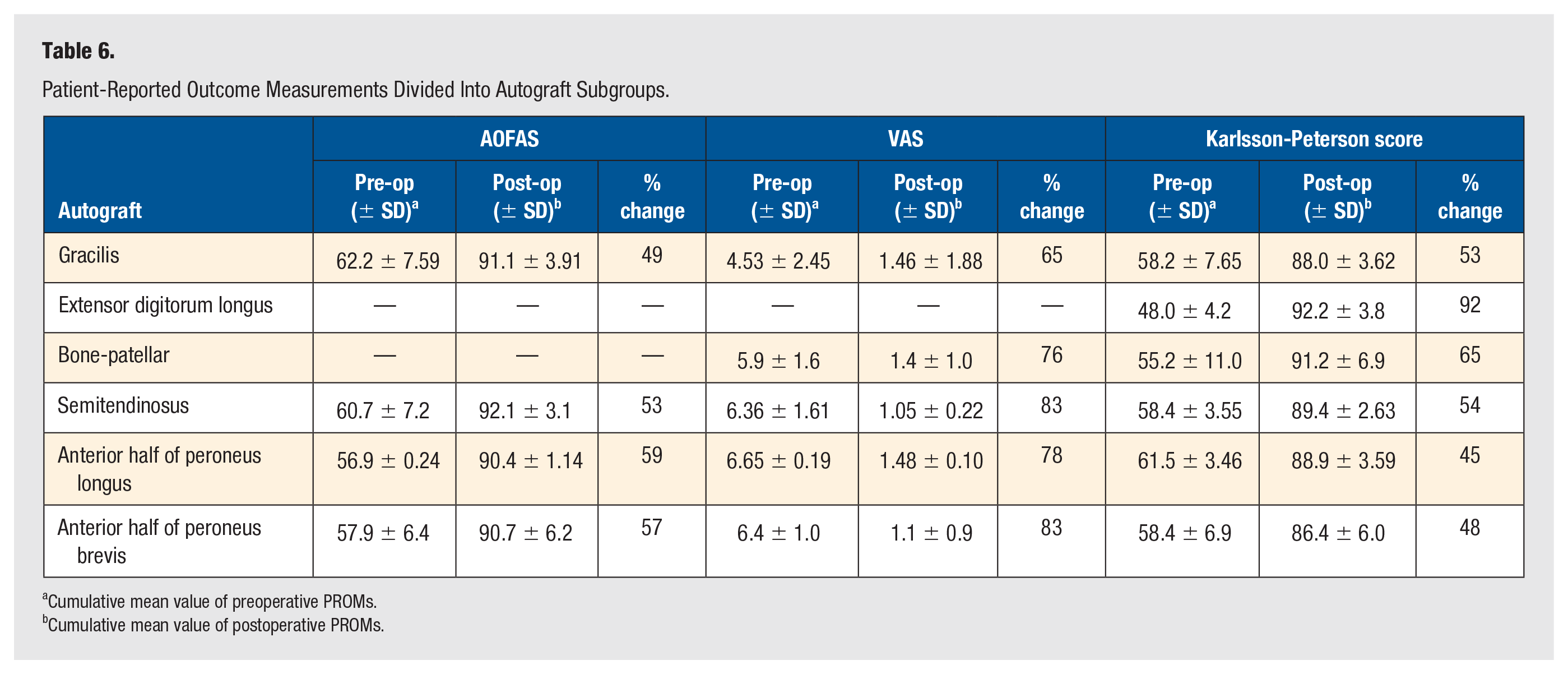
Cumulative mean value of preoperative PROMs.
Cumulative mean value of postoperative PROMs.
Complications Associated With Autografts
In the studies utilizing gracilis autograft, 84 out of 368 patients reported postoperative complications. In 4 cases, surgical revision was performed either due to autograft rupture or other unrevealed reasons. There were 17 cases of suspected injury to the superficial peroneal nerve due to patient-reported neuralgia and 5 cases of injury to the sural nerve. Postoperatively, 4 patients complained about peri-incisional numbness, pain or itchiness at the harvest site, 13 patients reported mild swelling, and 7 patients reported morning stiffness. In addition, there were 8 incidences of hardware-related issues, 14 cases of postoperative lateral ankle sprain, and 9 reports of regional chronic pain. In the cohort of 24 which underwent anatomic reconstruction using EDL autograft, 2 patients reported weakness in the dorsiflexion of the fourth toe and 1 case of mild cock-up deformity in the fifth toe. Among the 44 patients who received BPTB, 4 reported harvest-related problems. Two complained about sensory disturbance at the harvest site and the remaining 2 sustained an infrapatellar nerve injury during the harvest. There were also 2 separate incidences of a local infection. In the studies concerning semitendinosus autograft, of the 138 patients, there are reports of 1 postoperative residual instability and 1 recurrent ankle sprain. Of 110 ankles who received an intervention with anterior half of PL autograft, there were 6 cases of irritability over screw insertion site and 7 cases of ankle sprains following the procedure. There were no reported complications in the study concerning anterior half of PB.
Discussion
This review aimed to compare the effectiveness of different tendon autografts in an anatomic reconstruction of lateral ankle ligamentous complex and thus ascertain superiority of any autograft option. An ideal autograft should have adequate tensile strength to support ankle’s structure and function, easily accessible as well as safe to harvest without compromising the functionality of the donor site.5,26
Considering both PROMs and radiographic measurements, peroneal tendons have shown to be the most effective autografts. However, both outcome measurements suggested that there is no statistical difference between any autograft options. A closer analysis of postoperative complications and autograft properties reveals potential factors that might favor a surgeon’s choice of a particular autograft over the other. A successful anatomic reconstruction would come at the minimal compromise of the ankle’s pre-existing functionality and autograft donor site complications. Autograft harvest carries a risk of mechanical and functional damage to the anatomical site that given tendon supports. Peroneus brevis tendon has associated concerns with regards to tendon weakening and decreased power of eversion. 7 Nonetheless, there were no reported complications concerning PB tendon in this review. It is accepted that PB is a more effective evertor than PL, thus deeming the latter as a more suitable autograft choice. 25 However, of 110 ankles who received an intervention with anterior half of PL autograft, there were 7 cases of ankle sprains following the procedure. Autografts with a more distal harvest site can achieve ankle stability without affecting the peroneal tendons and subtalar movement. 18 Regarding its biomechanical properties, PL was shown to be comparable with semitendinosus and superior to other autografts in its strength to withstand load to failure in cadaveric studies. 5
Another aspect of the harvesting process to consider is the autograft accessibility. Harvesting gracilis tendon requires repositioning of the patient to a supine position. This not only prolongs the theater time but also necessitates broader knowledge of the local knee anatomy from a foot and ankle surgeon or potentially involvement of a second specialist. 25 In the case of gracilis, there is a secondary surgical site that introduces the risk of further complications. Within population included in this review, gracilis autograft exhibited seemingly higher rate of harvest-related and nerve injury-related complications when compared with other autograft options. These included suspected injury to the superficial peroneal nerve, injury to the sural nerve, peri-incisional numbness, and pain or itchiness at the harvest site. However, biomechanical properties and great tensile strength still consider gracilis as an adequate autograft choice. 11
A secondary surgical site and associated complications are also encountered with BPTB autograft. Bone-patellar tendon-bone autograft also casts doubt on its compatibility as an intervention, as its fibers resist the force perpendicular to the floor whereby autograft reconstructing the lateral ankle ligamentous complex requires a force axis oblique to the floor. 22
In addition to adequate biomechanical properties, 26 optimal autograft also potentially necessitates modification of the surgical technique to surmount the hindrances of a harvested tendon and make it suitable for a reconstruction. Extensor digitorum longus was found to be advantageous due to its great cross-sectional area and stiffness, but proved to be inadequate in dimensions, requiring the doubling or tripling the graft to provide sufficient material for ankle stabilization. 7 Also, the ease of access and harvest relies on the surrounding tissue. Extensor digitorum longus autograft harvest can frequently pose difficulty due to its adherence to the local surrounding tissue, also possibly accounting for postoperative complications. 7 In this study, 2 patients reported weakness in the dorsiflexion of the fourth toe and 1 case of mild cock-up deformity in the fifth toe.
Semitendinosus reportedly provides sufficient material in diameter and length for entire lateral ligamentous complex reconstruction. 6 Also, it is associated with the low incidence of complications. In this review, of the 138 patients, there are reports of 1 postoperative residual instability and 1 recurrent ankle sprain.
One of the limitations of this review was the identification of 8 additional studies that were initially missed during the database search and were later included by cross-reference of other reviews. This occurred despite conducting a comprehensive search across 2 databases. The omission of these studies may be attributed to the inherent variability in indexing terms in databases, potential limitations in keyword selection, and differences in how relevant studies were categorized in the literature. While the studies included in this review were all deemed of satisfactory quality for an inclusion eligibility, it is important to note that most studies were level IV evidence with nonrandomized treatment assignment, nonblinding of the examiners, and oftentimes paucity of homogeneity and consistency in the relatively small study population. In addition, overarching short follow-up period does not enable discussion on long-term efficacy and later occurring complications associated with different autograft interventions. Further studies tackling the mutual issue of patient adherence to a long-term follow-up would consolidate the indication of this procedure. Due to limited number of included studies reporting on return to daily or sporting activities, the comparison of this variable was left out of this review. Nevertheless, promoting inclusion of such factors into the future studies would further inform the decision behind the optimal graft, especially when coupled with clearly defined physical activity level of the population studied. Across studies, there is intravariability in population characteristics with regards to the mechanism of injury that led to the diagnosis of CAI. While this reduces the risk of population bias, further studies of these interventions in more focused cohorts such as athletes could provide more meaningful insights into the utility of specific autografts (Table 7).
Radiographic Assessment Outcomes Divided Into Autograft Subgroups.
The heterogeneity of PROMs used across studies made the initially proposed comparative analysis of autografts such as EDL and anterior half of PB unfeasible. Further studies concerning these autografts would inevitably provide a greater insight into the optimal choice of autograft. The subjectivity of PROMs potentially affects the reliability of the presented results which was attempted to be mitigated by contrasting those outcomes with more objective, radiographic assessment tools including ATT and TT.
Statistical analysis relied on the percentage change from preoperative to postoperative value as measured by distinct outcome measurements. Postoperative values were taken at the final follow-up which varied across studies and could be a confounding factor in determining the effectiveness of the intervention with a particular autograft. Furthermore, postoperative care undoubtedly has a significant impact on the resulting outcome of the intervention. Studies included in this review revealed different postoperative care either through formal rehabilitation program or patient care instructions. While patient’s characteristics and needs are predominant guides in individual postoperative journey, to what extent could those impact the outcome measurements at the follow-up is difficult to ascertain. Even though randomization and blinding in a surgical setting raise another set of ethical concerns, this review highlights the need for RCTs involving different autografts to mitigate the extent of confounding factors and provide a greater reliability in drawing conclusions about the autograft choice for an anatomic reconstruction of lateral ligamentous complex of the ankle.
Conclusion
This is to our knowledge the first review that focuses solely on autograft types in lateral ankle ligament reconstruction. Peroneal tendons have stood out as clinically superior autografts according to PROMs and radiographic measurements, though not statistically significant. These have also had the lowest incidence of complications among autografts. Caution should be exercised when using autografts with a more distal harvest site, such as gracilis or BTPB due to a higher rate of harvest-related and nerve injury–related complications. The choice of autograft should come at the minimal compromise of the ankle’s pre-existing functionality and autograft donor site complications, with consideration also given to autograft’s biomechanical properties, accessibility, and patient’s choice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought or required for this study, as it constitutes a systematic review of previously published data and did not involve the collection or analysis of new, identifiable patient information.
Informed Consent
Informed consent was not applicable to this study, as no new data were collected from human participants. The research involved secondary analysis of previously published studies, all of which are assumed to have obtained appropriate ethical approval and informed consent at the time of their original conduct.
Trial Registration
N/A.