
Abstract
Background:
Despite the increased popularity of reverse total shoulder arthroplasty, total shoulder arthroplasty is the standard treatment for advanced shoulder arthritis in young adult patients. Conventional metal-backed glenoid (MBG) designs result in more loosening and revision surgery compared with cemented polyethylene glenoid components. However, modern MBG designs have been recently devised to overcome such drawbacks.
Purpose:
To compare the radiolucency, loosening, and failure rates of modern MBG designs with those of conventional designs.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search for relevant articles was carried out using the PubMed, Cochrane Library, and Embase databases using MeSH (Medical Subject Headings) terms and natural keywords. A total of 362 articles were screened. We descriptively analyzed numerical data between the groups and statistically analyzed categorical data, such as the presence of loosening, failure, and revision surgery. The main outcome was the rate of revision surgery or failure. Subgroup analysis according to follow-up duration was performed to reduce heterogeneity.
Results:
A total of 25 articles (2036 shoulders) were included; 15 articles (1579 shoulders) involved a conventional MBG design, and 10 (457 shoulders) involved a modern design. The mean age of the patients was 64.2 and 66.5 years in the conventional and modern design groups, respectively, with a mean follow-up duration of 102.0 and 56.1 months, a mean gain of forward elevation of 35.1° and 61.7°, and a mean gain of external rotation of 24.2° and 39.2°. The rate of radiolucency was 48.0% and 16.7%, the rate of loosening was 11.2% and 4.9%, and the rate of revision was 15.9% and 2.4%, for the conventional and modern design groups, respectively. Subgroup analysis according to follow-up duration showed that the rates of loosening and revision were significantly lower in the modern design group (P < .001).
Conclusion:
Our findings suggest that modern MBG designs showed significantly lower loosening and failure rates than conventional designs. The overall results of the comparison, including loosening, failure, change in range of motion, and clinical scores, indicate that modern MBG designs are promising. More long-term follow-up studies on modern MBGs should be conducted.
First-generation shoulder arthroplasty was developed by Frederik Krueger 15 in 1951. This was followed by modular-type, second-generation shoulder arthroplasty with various humeral head diameters; however, the clinical results were not significantly improved. In the third generation, shoulder prostheses could be adapted to the individual patient so that the patient’s anatomic structure could be reconstructed. 22,30,31 Despite the increased popularity of reverse total shoulder arthroplasty (rTSA), TSA is the standard treatment for advanced shoulder arthritis in young adult patients with an intact rotator cuff. TSA consists of a glenoid component, humeral head, and humeral component, and each of these parts can vary in material, modularity, length, and design. Numerous studies have attempted to optimize the design for each component, but no clear conclusions have yet been drawn, and the matter is still being actively researched. 26
Neer et al 23,24 first introduced glenoid implants in shoulder arthroplasty to treat glenohumeral arthritis. The glenoid component can have a keel- or rod-type shape, and it can be composed of all-polyethylene (PE) materials or have a metal-backed design. Metal-backed glenoid (MBG) components usually have metal base plates, metal screws or rods, and PE liners. In the initial design, the PE liner was thin, resulting in high rates of wear and failure. 1 According to a systematic review conducted in 2014, MBGs have a higher failure rate than all-PE components. 29 Advanced designs were devised to overcome these shortcomings. 4,10,18
This systematic review aimed to summarize the results of TSA using MBGs and to compare the radiolucency, loosening, and failure rates of modern MBG designs with those of conventional MBG designs. The main outcomes were radiolucency, loosening, other complications, and failure or revision. Additionally, we compared range of motion (ROM) improvements and clinical scores for some of the studies that presented these data. We hypothesized that modern MBG designs would show lower rates of radiolucency, loosening, and failure than conventional MBG designs.
Methods
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 19 Additionally, it was registered on the PROSPERO website (CRD42019131822).
Inclusion and Exclusion Criteria
The inclusion criteria for this systematic review were as follows: (1) human adult participants, (2) presentation of the outcomes of TSA using an MBG component to treat any type of arthritis, (3) mean follow-up duration of more than 2 years, and (4) publication in English. The exclusion criteria were as follows: (1) case report or inclusion of fewer than 5 cases, (2) conference abstract or biomechanical study, (3) use of an implant that was not truly metal backed (eg, a glenoid component with only the rod made of metal), and (4) inclusion of glenoid revision or bone grafts.
Search Strategy and Study Selection
PubMed, Embase, and Cochrane Library were searched to find articles related to the topic. The search terms were determined through a group discussion and included a natural language search as follows: total AND shoulder AND (replacement OR arthroplasty) AND (metal OR backed OR (cementless glenoid)). After excluding duplicate documents, 2 independent reviewers (F.A., M.A.) screened the articles by title and abstract. They then made the final selection through a full-text review. This study also conducted citation tracking to find additional articles and checked newly published articles by performing a search update just before completing the review. All disagreements were solved by a group discussion involving ≥3 investigators.
Methodological Assessment and Data Extraction
Levels of evidence were assessed according to the Oxford Centre for Evidence-Based Medicine. 13 A methodological assessment was performed using the MINORS (Methodological Index for Non-Randomized Studies) tool, which has been validated. 34 Noncomparative studies are evaluated by 8 items and comparative studies by 12 items, and each item is scored as 0, 1, or 2 points. Thus, noncomparative studies can have a total score of 0-16 and comparative studies of 0-24. A study that scored ≥60% of the total score was considered a high-quality article.
The terms “modern design” and “conventional design,” which were the main themes of this study, were defined through a group discussion, during which the latest review articles on glenoid components were evaluated. The 3 advanced designs presented in the 2019 review by Castagna and Garofalo 3 were defined as modern designs: (1) the second-generation Systema Multiplana Randelli (SMR) MBG (LimaCorporate); (2) the first-generation trabecular metal (TM) glenoid, which consists of a soft MBG (Sulmesh; Zimmer Biomet); and (3) the second-generation TM glenoid (Zimmer Biomet). The second-generation SMR MBG had the following characteristics: curved back and less conforming shape, stiff and thick metal back (5 mm) to minimize wear, hydroxyapatite coating on a peg, and stable fixation through 2 screws and 1 central peg. The first- and second-generation TM glenoids were selected as modern designs because they were monoblock systems; they used porous tantalum or titanium to stabilize the initial fixation and reduce backside wear. The Sulmesh, one of the first-generation TM glenoids, consists of several layers of titanium mesh and has 4 pegs made of Protasul-Ti (Zimmer), which allows stable initial fixation without screws. 10 The second-generation TM glenoid exhibits a further improved design: a porous tantalum keel. The remaining designs were regarded as conventional designs.
Two independent reviewers (F.A., M.A.) extracted the following data from selected articles: publication year, number of patients and shoulders, months of follow-up, age, sex, surgery, history of disease or surgery, rehabilitation program, diagnosis, name of implant and manufacturer, clinical score, ROM, radiolucency, loosening, other complications, and revision surgery (failure). Radiolucency was defined as a radiolucent line of ≥1 mm, grade ≥2 on the Lazarus radiolucency scoring system, or at least 7 points of a total 18 points. 20 “Loosening” included both clinical and radiological loosening, and failure was defined as revision surgery because of an implant-related problem.
Statistical Analysis
We could not perform a meta-analysis on numerical data such as ROM and clinical scores because important data, such as the standard deviation, were often absent. Also, there was no specific patient-reported outcome that all articles used in common. Therefore, a descriptive analysis of the numerical data was conducted to compare the modern and conventional designs. Regarding categorical variables, such as the presence of radiolucency, loosening, and failure or revision surgery, statistical analysis was performed on the difference between modern and conventional designs. If preoperative factors, such as age or follow-up duration, differed between the 2 groups, we planned to minimize bias using a subgroup analysis of these factors. All statistical analyses were conducted using SPSS for Windows (Version 24.0.0.0; IBM), and P values <.05 were considered statistically significant.
Results
Search Results
A total of 177 articles in PubMed, 324 in Embase, and 29 in the Cochrane Library were found. After removal of duplicates, 362 titles and abstracts were screened, and 33 articles underwent full-text review. There were 24 articles that were included in the systematic review after the full-text review, and 1 article was added through citation tracking of the included articles. No additional articles were found in the search update. Figure 1 shows the entire process using a PRISMA flow diagram. Overall, 15 studies used conventional MBG components, ¶ and 10 studies used modern MBG components. #

PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flow diagram showing the selection of appropriate articles.
Assessment of Methodological Quality and Heterogeneity
Levels of evidence were determined by an agreement between 2 researchers (D.M.K., K.H.K.), and no disagreements occurred. There was 1 randomized controlled trial (level 1), 1 study with level 3 evidence, and 23 studies with level 4 evidence. The mean MINORS score was 9.43 ± 1.35 for noncomparative studies and 19 ± 0 for comparative studies. Also, 9 of 15 articles (60.0%) that used conventional designs and 6 of 10 articles (60.0%) that used modern designs were high quality. The distribution of age and follow-up duration in each study is shown using a summary plot (Figures 2 and 3) to determine the heterogeneity between the 2 groups. In the summary plot, age showed a similar pattern between the 2 groups, but the conventional design group had a longer follow-up period than the modern design group.

Summary plots for age.

Summary plots for follow-up duration.
Summary of Outcomes of Each Article
The demographic data and outcome measurements of each study are summarized in Table 1. The TSA outcomes were presented using various items and measurement methods; the following were the most common: ROM (10 and 6 articles for conventional and modern designs, respectively), the visual analog scale for pain (3 and 7 articles, respectively), the Constant score (6 and 3 articles, respectively), the American Shoulder and Elbow Surgeons score (1 and 6 articles, respectively), complications (all articles), and revision surgery or failure (all articles). The results of each article with regard to these commonly used items are shown in Table 2.
Demographic Data and Outcome Measurements of Individual Studies a

a ABD, abduction; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FE, forward elevation; IR, internal rotation; LOE, level of evidence; NR, not recorded; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; SF-36, 36-Item Short Form Health Survey; SMR, Systema Multiplana Randelli; SST, Simple Shoulder Test; TM, trabecular metal; VAS, visual analog scale.
b Data are shown as mean, mean ± SD, mean ± SD (range), mean (range), or range.
c Neer II metal-backed polyethylene component (Kirschner Medical).
d Aequalis metal-backed glenoid (Tornier).
e Copeland CSRA (Cementless Surface Replacement Arthroplasty; Zimmer Biomet).
f Kirschner II-C uncemented glenoid component (Kirschner Medical).
g BioModular TSR prosthesis (Zimmer Biomet), initial Nottingham TSR prosthesis, and Nottingham TSR prosthesis (Zimmer Biomet).
h Neer I metal-backed polyethylene component (Kirschner Medical).
i Neer II metal-backed polyethylene component and Cofield 1 and 2 metal-backed polyethylene components (Smith & Nephew).
j BioModular TSR prosthesis.
k Univers metal-backed, uncemented glenoid implant (Arthrex).
l ARROW universal shoulder prosthesis (FH Orthopedics).
m Second-generation SMR system (Systema Multiplana Randelli; LimaCorporate).
n Sulmesh titanium metal-backed glenoid component (Zimmer Biomet).
o Second-generation, porous, tantalum trabecular metal glenoid (Zimmer Biomet).
Clinical Outcomes of Studies Using Conventional and Modern Designs of MBG Components a

a ER, external rotation; FE, forward elevation; MBG, metal-backed glenoid; NR, not recorded; RC, rotator cuff.
b Data are shown as n (%).
Comparison Between Conventional and Modern MBG Designs
Table 3 shows the results of our comparison of modern versus conventional MBG designs based on the studies reviewed. The mean gain in forward elevation was 35.1° and 61.7° and the mean gain in external rotation was 24.2° and 39.2° for conventional and modern designs, respectively. The respective rates of radiolucency, loosening, and revision surgery (failure) were 48.0%, 11.2%, and 15.9% in the conventional design group and 16.7%, 4.9%, and 2.4% in the modern design group. A scatter plot was used to graph the rates of loosening and failure of each study according to the follow-up duration (Figure 4). The graphs showed that the modern design group tended to have lower loosening and failure rates than the conventional design group. In addition, a subgroup analysis according to follow-up duration was performed (Table 4). The rates of radiolucency, loosening, and revision surgery were significantly lower in the modern design group (P < .001 in all cases), with the exception of radiolucency in cases with a follow-up duration of ≤6 years. The findings of the subgroup analysis concurred with the overall comparison between the 2 groups.
Comparison Between Conventional and Modern Designs of MBG Components a

a ER, external rotation; FE, forward elevation; MBG, metal-backed glenoid.

(A) Rate of loosening or wear according to design and follow-up duration. (B) Rate of revision surgery or failure according to design and follow-up duration. MBG, metal-backed glenoid.
Subgroup Analysis of Radiolucency, Loosening, and Revision Surgery (Failure) According to Follow-up Duration a

a Data are shown as n (%).
The causes of revision surgery are summarized in Figure 5. The most common cause of failure in cases that used conventional designs was loosening (118 cases; 47.0%), while in cases that used modern designs, the most common cause was fracture of the glenoid component (6 cases; 54.5%). Other complications, excluding implant problems, occurred in 91 cases (5.8%) that used a conventional design and in 14 cases (3.1%) that used a modern design (Figure 6). Such complications in the conventional design group included instability (33 cases; 36.3%), wound problems (22 cases; 24.2%), and rotator cuff tears (20 cases; 22.0%). The most commonly seen complications in the modern design group were stiffness (5 cases; 35.7%), rotator cuff tears (3 cases; 21.4%), and instability (2 cases; 14.3%).
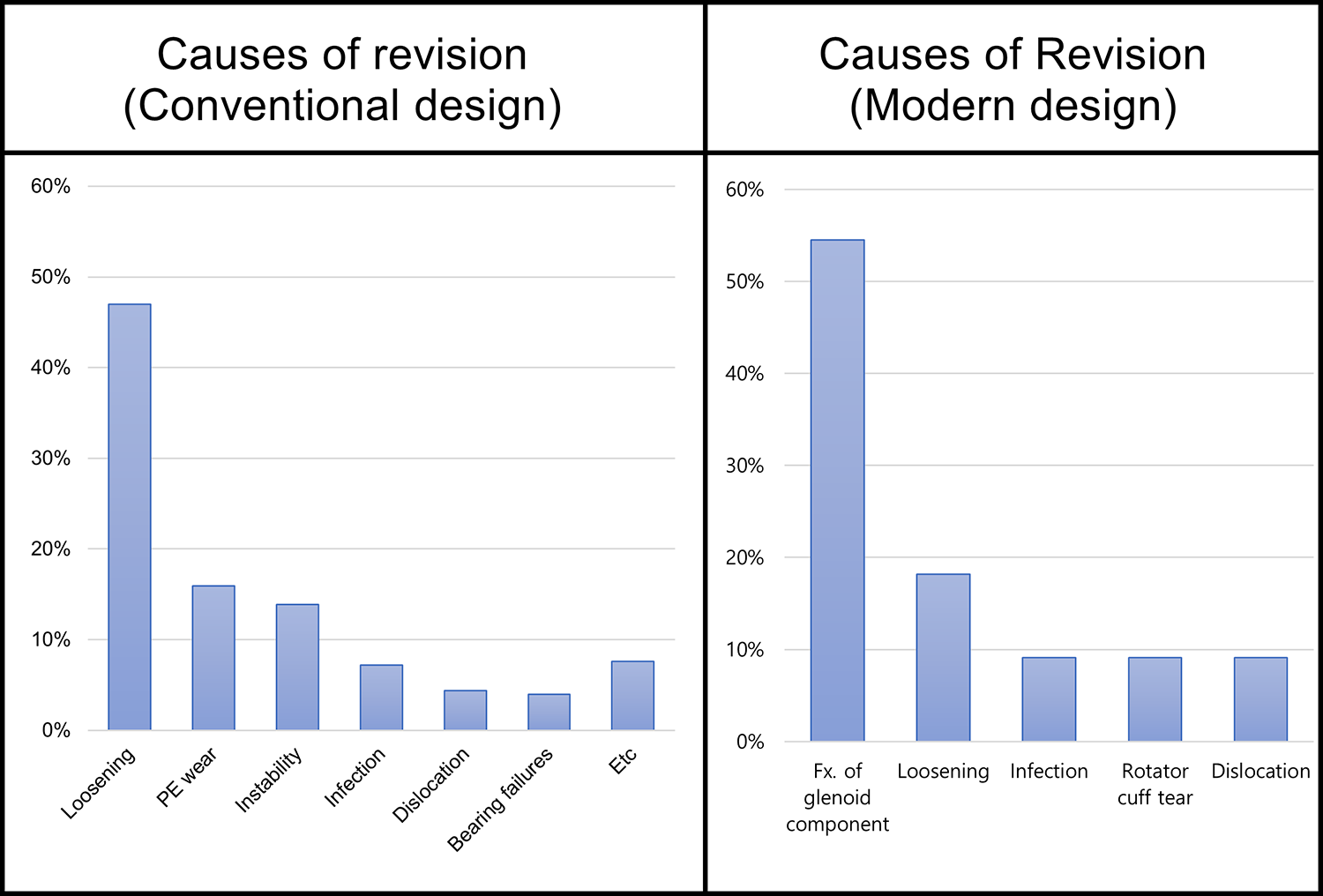
Graph showing the causes of revision surgery. Fx, fracture; PE, polyethylene.

Other complications in the conventional and modern design groups.
Discussion
A systematic review carried out in 2014 compared complications and revision surgery rates between MBG and all-PE glenoid components and found that MBGs showed significantly higher rates of complications and reoperations. That review included all MBG implants in the same group. 29 After MBGs were abandoned by many surgeons, attempts were made to improve the design, altering the shape of the implant, the design of the peg and keel, and the angle of the screws or peg. The second-generation SMR MBG is representative of the modern design. Castagna et al 4 reported good results using this device, citing the following reasons: (1) the shape of the glenoid—the implants have a curved back and are less conforming; (2) a stiff and thick metal back (5 mm), which reduces stress on the PE component and reduces wear; (3) hydroxyapatite on the peg as well as the base plate; and (4) the presence of 2 screws and 1 central peg, which ensures stable fixation.
Another representative modern design is Zimmer Biomet’s tantalum or titanium TM. The first-generation TM glenoid—the Sulmesh soft MBG—consists of several titanium meshes, and 4 pegs protect the metal back. The second-generation TM glenoid shows an improved design with a porous tantalum keel. Recent clinical studies on these modern MBG designs have reported good results. ** Future improvements in these modern designs may further minimize negative outcomes and improve overall results. 3
In the current review, after comparing variables such as ROM change, loosening, and revision surgery (failure), the modern designs of MBG components seem promising compared with the conventional designs. Our hypothesis was supported by the results. Statistical analysis of numerical data such as ROM was not possible because many studies did not provide the standard deviation. However, most studies presented information regarding radiolucent lines on plain radiography, loosening, and revision (failure). Furthermore, because these data were presented in a categorical fashion, such as present versus absent, they were analyzed able to be using crosstab analysis. The scatter plot and subgroup analysis showed that loosening and failure were less common in the modern design group than in the conventional design group (P < .001 for each item).
MBGs were designed to allow strong fixation by inducing bone ingrowth using a porous-coated component at the glenoid interface. The joint surface was designed to induce smooth ROM using a PE component. Various types of MBGs have been developed, most of which are cementless and are fixed to the glenoid using screws or rods. General advantages of MBGs over cemented PE glenoids are as follows: (1) bone ingrowth that provides greater stability, (2) easy conversion to reverse TSA, (3) concomitant bone graft procedure in case of severe glenoid bone loss, and (4) no complications related to cement. Conventional MBGs were expected to be an ideal design, but the results of clinical studies were disappointing. †† The following reasons were given for this: (1) PE wear, which occurs because the metal back necessitates a thin PE liner 9 ; (2) overstuffing of joints, which was often done to ensure sufficient PE thickness, resulting in loosening and rotator cuff tears and eventually leading to joint instability; and (3) failure of rods and screws, which are not used in cemented, all-PE glenoid components.
A 2018 study by Page et al 27 analyzed glenoid revision rates using the Australian Orthopaedic Association National Joint Replacement Registry, which was begun in 2004. Cementless MBGs were classified into a modular and fixed type in the study, and SMR L1, L2, and TM glenoids were included in the analysis. Cementless glenoids showed a significantly higher revision rate compared with cemented glenoids. Contrary to the results of the study by Castagna et al, 4 which used SMR L1 glenoid, the SMR L2 design showed a higher revision rate than other designs according to Page et al. Based on the result, SMR L2 was withdrawn from the market. Only L1 glenoid has been used since 2012. TM glenoids, on the other hand, showed the same low revision rate in the current review and in the study by Page et al. Results of this review and the study by Page et al suggest that surgeons be cautious in their selection of MBG because different designs can produce different results. TM glenoids are promising and comparable with cemented glenoids. However, TM glenoids cannot be easily converted to reverse TSA because of the monoblock design. SMR glenoids can be easily converted to reverse TSA and can be used even in case of glenoid bone loss. More reports regarding the results of the SMR are needed.
This study has several limitations. First, although we carried out a systematic search using predefined criteria and search terms, we may have missed some articles. Second, there is no clear consensus about the distinction between modern and conventional designs. We based our definitions on the study by Castagna and Garofalo, 3 which was the most up-to-date review article presenting the rationale for glenoid components. Third, a meta-analysis or Kaplan-Meier analysis could not be carried out because the current study failed to acquire all the appropriate data. It is for this reason that the numerical data, such as clinical scores and ROM, were not significant, even though the difference was quite large. Fourth, the follow-up duration in the modern design group was relatively short; this was the main heterogeneity against the conventional design group. However, we minimized this heterogeneity through the scatter plot and subgroup analysis according to the follow-up duration. Also, most of the modern designs were TM glenoids. This made it difficult to generalize on the advantages of modern MBG designs.
Conclusion
Our findings suggest that modern MBG designs, especially the TM glenoid, showed significantly lower loosening and failure rates than conventional designs. The overall results of the comparison, including loosening, failure, change in ROM, and clinical scores, indicate that the modern MBG designs are promising. More long-term follow-up studies on modern MBGs should be conducted.
Footnotes
Acknowledgment
Final revision submitted March 7, 2020; accepted April 10, 2020.
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Basic Science Research Program through the National Research Foundation of Korea, funded by the Ministry of Education (NRF-2018R1D1A1A02086025). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.