
Abstract
Background:
Athletes who return to sport (RTS) after anterior cruciate ligament reconstruction (ACLR) often have reduced physical performance and a high reinjury rate. Additionally, it is currently unclear how physical performance measures can change during the RTS transition and with the use of a functional knee brace.
Purpose/Hypothesis:
The purpose of this study was to examine the effects of time since surgery (at RTS and 3 months after RTS) and of wearing a brace on physical performance in patients who have undergone ACLR. We hypothesized that physical performance measures would improve with time and would not be affected by brace condition.
Study Design:
Controlled laboratory study.
Methods:
A total of 28 patients who underwent ACLR (9 males, 19 females) completed physical performance testing both after being released for RTS and 3 months later. Physical performance tests included the modified agility t test (MAT) and vertical jump height, which were completed with and without a knee brace. A repeated-measures analysis of variance determined the effect of time and bracing on performance measures.
Results:
The impact of the knee brace was different at the 2 time points for the MAT side shuffle (P = .047). Wearing a functional knee brace did not affect any other physical performance measure. MAT times improved for total time (P < .001) and backpedal (P < .001), and vertical jump height increased (P = .002) in the 3 months after RTS.
Conclusion:
The present study showed that physical performance measures of agility and vertical jump height improved in the first 3 months after RTS. This study also showed that wearing a knee brace did not hinder physical performance.
Clinical Relevance:
Wearing a functional knee brace does not affect physical performance, and therefore a brace could be worn during the RTS transition without concern. Additionally, physical performance measures may still improve 3 months past traditional RTS, therefore justifying delayed RTS.
As many as 250,000 anterior cruciate ligament (ACL) injuries occur in the United States each year. 14 Most athletes will undergo ACL reconstruction (ACLR) surgery in hopes of restoring knee stability and allowing for return to sports (RTS). 19 However, even after surgical reconstruction and 6 to 12 months of rigorous physical therapy, many athletes with ACLR are unsuccessful when attempting RTS. 2,32 In a recent meta-analysis, Ardern et al 2 reported that although 82% of ACLR patients returned to some level of sport postoperatively, only 63% successfully returned to their preinjury level of sport and 44% returned to competitive sport. These low rates of successful RTS are also found among collegiate and professional athletes, who are expected to have excellent access to physical therapy and both the time and the motivation needed for successful recovery. 5,45 In athletes who do successfully return to their sport after ACLR, marked decreases in performance have been noted. 5,17,45 A more complete understanding of the factors that govern physical performance in athletes recovering from ACLR is necessary to optimize the RTS transition.
The early RTS period is a stressful time for athletes recovering from ACLR, as they transition back to sport after being in a physical therapy setting. Recovering athletes may want to perform well when returning to sport, but they must understand that they have not finished their recovery and that the RTS transition needs to be gradual to prevent further injury. 11 The later stages of physical therapy often focus on recovery of surgical limb strength and power, with the goal of returning to sports and preventing secondary injuries. 4,27,47 The ability to complete sport-specific tasks without deficits should also be a focus to ensure that patients will be able to achieve RTS at an appropriate level of performance. 27 However, little research has been conducted regarding how physical performance can change in the early RTS transition in athletes recovering from ACLR.
Many orthopaedic surgeons prescribe a knee brace for their ACLR patients to wear during activity, 10,24 but low brace compliance remains an issue. Despite moderate evidence suggesting that braces improve movement mechanics and reduce the risk of reinjury in athletes such as skiers, 42 many athletes choose not to wear their brace owing to concerns about its impact on their physical performance. 23,28,35,37 Although the impact of brace wear on sport performance has been a potential concern, previous studies have reported conflicting results when examining whether a functional knee brace improves, 8,33 hinders, 9,48 or has no effect 3,26,44 on physical performance. Most studies did not provide time for participants to get accustomed to the brace, 3,9,26,33,44,48 but the impact of brace wear on performance has been shown to decrease as participants become acclimated to the brace in healthy control populations. 36 Furthermore, healthy individuals 3 and patients with ACL deficiency 8,26,44 have been the subject of previous studies on the effects of bracing on physical performance, which cannot necessarily be generalized to patients who undergo ACLR. A more complete understanding of the effects of brace condition, in addition to time since surgery, on physical performance measures would help surgeons determine the best methods to help athletes achieve RTS.
Physical performance tests are widely used to both assess recovery and retrain athletic ability in patients recovering from ACLR. 4,13,15,27 Unilateral hop tests are the most widely used physical performance tests in athletes recovering from ACLR, but although hop testing has proven to be important for determining readiness for RTS from an injury prevention perspective, 20,34 other measures may better address the question of whether athletes are prepared to return from a performance standpoint. For example, the modified agility t test (MAT) is widely used by athletic trainers and coaches for quantifying agility. The MAT incorporates acceleration, deceleration, change of direction, side shuffling, and backpedaling, which are fundamental movements in many sports. 30,39 Because jumping is another fundamental movement in sports, the countermovement jump (CMJ) test is widely used to quantify an athlete’s explosive power. 30 Scores on the MAT are not correlated with CMJ height or 10-m straight sprint times, suggesting that these physical performance measures quantify multiple independent aspects of sports-related movement ability. 39 The MAT and CMJ tests have also been incorporated into clinical RTS test batteries to assess physical performance, suggesting that results on these tests may be important with regard to injury prevention. 11 Despite the importance of these tests, limited research has been conducted on these performance metrics, with the exception of 1 study which found that MAT time improved between 4 and 6 months after ACLR surgery while vertical jump height had a minimal improvement. 40 However, there is a clear need for further testing on the factors that affect performance measures and how they could be incorporated into future RTS evaluations.
The purpose of the present study was to determine whether physical performance would change in athletes recovering from ACLR during the first 3 months after returning to sport participation and while wearing a custom-fit, extension constraint, functional knee brace. We hypothesized that wearing the brace would have no impact on physical performance, as previous literature has found that brace condition does not affect hop distance, 3,26,44 but that physical performance measures would improve over the 3-month period.
Methods
Patients
A total of 30 participants (9 male, 21 female; age, 19.4 ± 4.2 years; height, 1.73 ± 0.07 m; mass, 72.4 ± 13.5 kg) recovering from primary unilateral ACLR completed institutional review board informed consent documents and were enrolled in the study between May 2016 and May 2017. All participants had been involved in competitive sports before injury, had no previous knee injury or surgery, and did not have any additional ligament injuries. All participants had undergone physical therapy, had been released to RTS by their surgeon, and had completed similar formal rehabilitation protocols designed to prepare them for RTS. Decisions on RTS release and bracing protocols were made by the surgeon and were not collected as part of this study design. In total, 17 participants had injured their dominant limb and 13 had injured their nondominant limb, which was defined as the limb used to kick a soccer ball. Most patients received an autograft (8 hamstring, 21 patellar tendon), except for 1 patient who received an allograft. All participants were given a custom-fit functional knee brace (DonJoy Orthopaedics) with extension resistance in the last 30° and were instructed by their surgeon to wear the brace while doing anything more strenuous than walking. The participants were tested according to the study protocol upon RTS as well as 3 months later (RTS+3).
Procedure
Before the surgical procedure, participants completed the ACL Return to Sport after Injury (ACL-RSI) scale, which quantifies the psychological aspects of recovering from an ACLR and returning to sport, 46 and the Marx activity score, which quantifies physical activity. 21 Participants also completed these scores at RTS and RTS+3. Before the performance testing session, all participants were asked to wear a neutral cushioned running shoe (Air Pegasus; Nike Inc) provided by the laboratory and were given time to become accustomed to the shoe before testing. Tests of the single hop, triple hop, and crossover hop on the surgical and nonsurgical limb were performed to document functional ability in the nonbraced condition at the time of RTS. 34 At each visit, the participant completed the MAT and a maximum vertical jump. These were done with and without a knee brace on the surgical leg, and the order (braced and unbraced) was randomized. The participant was given a 5-minute break between each task to prevent fatigue.
Agility Testing
The MAT was used to quantify agility; this test incorporates straight sprinting, directional changes, lateral movement to both the left and right, as well as backpedaling. Figure 1 shows the agility course setup for the MAT. Participants began with their feet behind a line at cone A. When they were ready, they first sprinted to cone B, shuffled left to cone C, shuffled right to cone D, shuffled left back to cone B, and then backpedaled through the same line they started from at cone A. 39 All participants were instructed to touch the base of each cone with their hand, to not cross their feet while shuffling, and to face forward throughout the entire test. If these conditions were not met, the trial was not scored and was repeated. A timing gate (Brower Timing Systems) was placed immediately in front of the start/finish line, which measured completion time to the nearest hundredth of a second. The t test and the MAT have been previously found to have high between-session reliability. 30,39 The MAT was completed 3 times in both the braced and the nonbraced conditions at each visit. The 3 trials in each condition (braced vs nonbraced) were averaged by condition at each visit.

Course schematic of the modified agility t test. Participants sprinted from cone A to B, side shuffled left to cone C, side shuffled right from cone C to D, side shuffled left back to cone B, and then backpedaled back to cone A.
Maximum Vertical Jump
The vertical jump test was used to quantify power. We began by measuring the participant’s standing maximal reach height with his or her dominant limb followed by measuring a maximal vertical jump with the same arm reaching upward, both measured to the nearest tenth of a centimeter (Brower Vertical Jump). 38 Maximum jump height was then taken as the difference between maximal height of the hand while the participant was standing and jumping. This test was completed 3 times in both the braced and the nonbraced conditions and was averaged for both conditions at each visit.
Statistical Analysis
All statistics were completed by use of SPSS (Version 24; SPSS Inc) with a significance level of .05. Repeated-measures analyses of variance were performed to determine the main effects of time (RTS and RTS+3) and brace (braced and unbraced) and the average values for each task (MAT times and vertical jump height). In addition to determining the total MAT time, we also evaluated the times to complete the sprinting, side shuffling, and backpedaling portions of the test. Paired t tests were completed to compare the ACL-RSI and Marx scores between the testing visits. Effect sizes were calculated with η2, which is the proportion of the dependent variable (speed or jump height) that can be attributed to the independent variable (time or brace). Therefore, a larger effect size indicates a stronger relationship between the 2 variables, or the fact that the independent variable (eg, brace) has a large effect on changes in the dependent variable (eg, speed). These effect sizes were considered small, medium, and large if they were above 0.04, 0.25, and 0.64, respectively. 12
Results
Of the 30 initial patients, 2 female participants did not complete the study and were therefore excluded from this analysis. Initial testing was completed at a mean ± SD of 6.95 ± 1.27 months after surgery when the patient was returned to sport (RTS), and follow-up assessments were completed approximately 3 months (3.46 ± 0.49 months) after the initial visit (RTS+3). The limb symmetry index for participants at the time of RTS, calculated as the distance ratio between the surgical and nonsurgical limb (100% indicates perfect symmety), was 80.7% ± 12.4% for the single hop, 77.0% ± 13.8% for the triple hop, and 79.5% ± 17.2% for the crossover hop. ACL-RSI scores significantly increased between the 2 visits (RTS, 87.2 ± 20.1; RTS+3, 93.9 ± 16.9; P = .028); however, no significant difference in Marx scores was found between the testing sessions (RTS, 14.3 ± 2.6; RTS+3, 13.8 ± 3.6; P = .867).
The MAT and vertical jump height (Table 1) were significantly different between the 2 time points. Agility course times improved for the total time (nonbraced RTS, 8.75 ± 1.19 seconds; nonbraced RTS+3, 7.86 ± 0.62 seconds; P < .001; η2 = 0.505), the side shuffle (nonbraced RTS, 5.60 ± 0.87 seconds; nonbraced RTS+3, 4.93 ± 0.50 seconds; P < .001; η2 = 0.492), and the backpedal (nonbraced RTS, 1.75 ± 0.24 seconds; nonbraced RTS+3, 1.58 ± 0.15 seconds; P < .001; η2 = 0.464). Vertical jump height also improved between RTS and RTS+3 independent of brace condition (nonbraced RTS, 15.45 ± 3.50 cm; nonbraced RTS+3, 16.70 ± 3.06 cm; P = .002; η2 = 0.313). Brace condition did not have any significant effects on physical performance. The only interaction between time since surgery and brace condition occurred in the side shuffle (P = .047; η2 = 0.139). This interaction revealed that the effect of brace condition on side shuffle performance changed with time, as the brace slightly improved performance at RTS but slightly decreased performance at RTS+3.
Effect of Time After Return to Sport and Brace Use on the Performance Measures of a Modified Agility t Test and Vertical Jump a
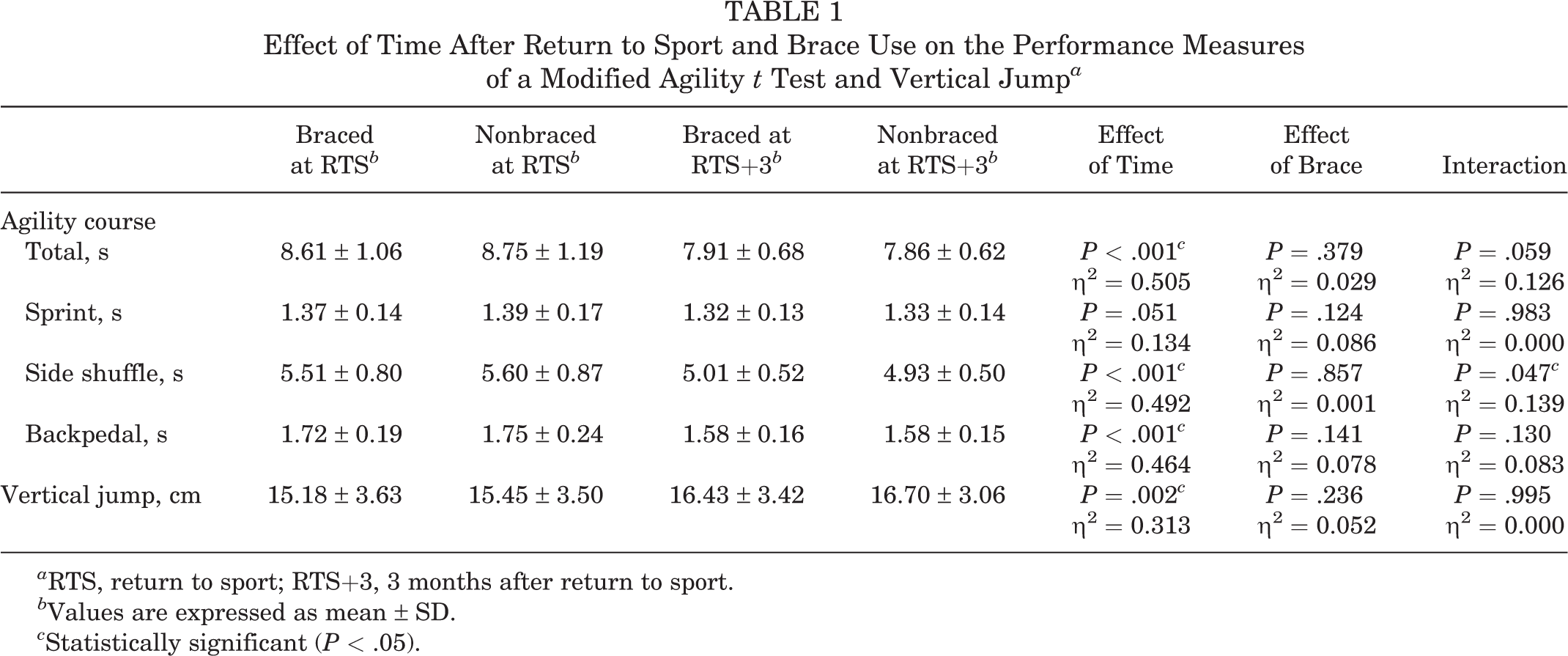
a RTS, return to sport; RTS+3, 3 months after return to sport.
b Values are expressed as mean ± SD.
c Statistically significant (P < .05).
Discussion
The purpose of the present study was to compare the effect of time since surgery (RTS and RTS+3) and of wearing a functional knee brace on physical performance measures in patients recovering from ACLR. We hypothesized that physical performance would improve in the 3 months after RTS independent of knee brace condition and that physical performance would be similar between the braced and nonbraced conditions. Agility and jump height significantly improved between the RTS time point and the RTS+3 assessment, which indicates that physical performance improved after patients were released from physical therapy and returned to sport participation. Although improvements in physical performance measures were seen across this time period, the results of this study did not indicate whether these athletes had any improvement in other aspects of sport performance. Additionally, the results indicate that functional knee braces do not hinder sports performance, based on the measures involved in the present study.
Many surgeons consider range of motion and knee stability when determining whether to allow a patient to RTS, 32 but other surgeons have suggested that RTS decisions should also consider physical performance measures. 13,15,27,29 The MAT and CMJ have been added to RTS test batteries to further quantify physical performance and provide additional measures for determining when athletes are ready for RTS. 27,40 The present study used the MAT and CMJ to quantify agility and power, respectively. This examination of physical performance found that patient agility improved in 24 of 28 participants and jump height improved in 20 of 28 participants with time since surgery. This suggests that ACLR patients were more physically prepared for the athletic demands of their sport 3 months after RTS. A previous study found that total MAT time moderately improved with time and rehabilitation, but unlike the results in the current study, those authors found that there was minimal improvement in jump height. 40 This difference could be because the previous study tested participants at 4 and 6 months after surgery, 40 whereas the current study tested participants at approximately 6 and 9 months after surgery, suggesting that the measure of jump height may improve in later stages of recovery. Although further research would allow for more thorough conclusions, the results of the present study suggest that delaying RTS, focusing on sports performance tasks during rehabilitation, and transitioning to full activities gradually may make the RTS transition more successful.
The RTS transition should be gradual, and athletes should work to improve performance-based tasks to optimize their chances of successful RTS. Physical therapy and rehabilitation protocols focus on muscle strength, 4,47 improving speed in athletic movements, movement symmetry, power production, and endurance, 27,40 but little is known about what happens to these measures after patients are released from physical therapy and return to sport participation. Unfortunately, due to a variety of factors, athletes are often cleared for RTS even though their performance levels are still being recovered and they may still have some functional deficits. 22
High expectations despite functional deficits can cause psychological stress for these athletes, which has been shown to be present throughout the rehabilitation process and the RTS transition. 1,18,25,46 The current study evaluated psychological changes through ACL-RSI scores and found that they improved between the first and second testing sessions. This agrees the findings from another study that ACL-RSI scores linearly increase after ACLR. 18 These results indicate that athletes may feel more confident about their knee and returning to sport at their second visit, which may also be related to their improved physical performance.
In addition, the present study focused on the effect of brace condition on physical performance measures throughout the RTS transition and found that physical performance was not affected by wearing a brace. Many orthopaedic surgeons prescribe a functional knee brace for ACLR patients to wear during activity. 10,24 The findings from the present study agree with other studies which have found that brace condition does not affect physical performance tests, quadriceps or hamstring strength, knee function, or static knee stability. 16,23,35 There is evidence that brace wear may improve movement mechanics during walking and running by increasing knee flexion 8,41 and during cutting by increasing knee flexion velocity at initial contact. 8,9 Additional research has shown that braces improve jumping mechanics such as bilateral landing symmetry 6 and vertical jump height. 33 One study found that hop distance symmetry improved with time and a braced condition, which suggests that both time and bracing may not only improve physical performance but also help prevent additional injury. 31 Finally, previous studies have shown that athletes may be more confident wearing a brace on their surgical limb during physical activity. 7,43 These findings combined with the results from the present study suggest that physical performance measures are either unaffected or improved when athletes wear a brace. Future work should also focus on the effects of braces outside of the laboratory setting during sport as well as determine whether there are responders and nonresponders to brace wear in order to target bracing interventions.
Some limitations were associated with the present study. One potential limitation is the fact that no information about RTS criteria, physical therapy activities, or specific rehabilitation protocols was collected from the participants. Additionally, the number of male and female participants was not evenly split, and we did not account for the potential influence of graft type. Controlling RTS, rehabilitation, sex, and graft type could allow for a more homogeneous participant population. Another potential limitation is that participants were asked to wear the brace during any activity more strenuous than walking, but this was not monitored or controlled. Furthermore, the study did not include a control group that was not provided a brace to wear between testing sessions. Such a control condition could have allowed for conclusions about whether improvements over time were strictly due to time since surgery. One final limitation is the fact that based on the enrollment date, there was an overlap in time since surgery for the testing sessions (some participants underwent their second session before other participants had their first session). However, this is unlikely to have affected the results of this study.
Conclusion
Agility and vertical jump height in patients who had undergone ACLR improved in the 3 months after RTS, independent of brace condition. The mechanism for this improvement and the risk of second ACL injury are not fully understood and should be investigated further. Additionally, even though the long-term effects of brace wear on movement mechanics are unclear, the results from this study indicate that braces can be worn without a major impact on physical performance.
Footnotes
Final revision submitted January 15, 2020; accepted February 24, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from DonJoy Orthopaedics. J.T.M. is a consultant for Stryker, Corin, and United Orthopaedics; is on the advisory board for United Orthopaedics; is on the speaker’s bureau for Stryker; receives royalties from DePuy and Corin; and has stock options with Think Surgical and Invuity. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Carilion Clinic Institutional Review Board (protocol No. 2107).