
Abstract
Background:
Deficits in neuromuscular control are common after anterior cruciate ligament (ACL) reconstruction and may be associated with further knee injury. The knee valgus angle during a single-leg squat (SLS) is one measure of neuromuscular performance.
Purpose:
To determine whether the knee valgus angle during SLS changes between 6 and 12 months after ACL reconstruction and to assess how the operative knee valgus angle compares with that of the contralateral side.
Study Design:
Case series; Level of evidence, 4.
Methods:
A cohort of 100 patients with uninjured contralateral knees were assessed at 6 and 12 months after primary hamstring autograft ACL reconstruction. Participants performed the SLS on each leg, and the knee valgus angle was measured via frame-by-frame video analysis at 30° of flexion and at each patient’s maximum knee flexion angle.
Results:
For the operative limb at 30° of flexion, a small but statistically significant reduction was noted in the valgus angle between 6 and 12 months (5.46° vs 4.44°; P = .002; effect size = 0.24). At 6 months, a slightly higher valgus angle was seen in the operative limb compared with the nonoperative limb (5.46° vs 4.29°; P = .008; effect size = 0.27). At maximum flexion, no difference was seen between limbs in the valgus angle at either 6 or 12 months, and no change was seen in the operative limb between 6 and 12 months. At 6 months and 30° of knee flexion, 13 patients had a valgus angle greater than 10°. This group also had a higher mean valgus angle in the contralateral limb compared with the contralateral limb in the other 87 patients (8.5° vs 3.65°; P < .001).
Conclusion:
During a controlled SLS, the knee valgus angle remained essentially constant, and minimal limb asymmetries were present over the 6- to 12-month postoperative period, a time when athletes typically increase their activity levels. Whether changes or asymmetries will be seen with more dynamically challenging tasks remains to be determined. When present, high valgus angles were commonly bilateral.
Keywords
Deficits in neuromuscular control are common after anterior cruciate ligament (ACL) reconstruction and have been associated with an increased risk of reinjury. 13,14,25,27,35,36 Assessment of neuromuscular performance is therefore regularly incorporated into the assessment of readiness for return to sports after ACL reconstruction. 4,8,18,29
The analysis of neuromuscular control and biomechanical function is complex. In the clinical environment, many practitioners use clinician-friendly performance tests to aid in their assessment. 10,12 The single-leg squat (SLS) test is one such assessment tool that has gained popularity to provide a snapshot of overall biomechanical function and to identify potential neuromuscular deficits in the lower limb kinetic chain. 2,3,7,9,19,20,33,34,37 The SLS combines movements of the trunk, hip, knee, and ankle. 19,33,34,37 There are many ways to assess SLS performance and various parameters of interest. Ipsilateral trunk lean, pelvic tilt, hip adduction and internal rotation, knee valgus, and loss of balance have been used and are generally accepted as important elements in the evaluation of SLS performance. 7,9,20
Previous investigations into SLS performance after ACL reconstruction have illustrated poor performance in almost 50% of patients at 6 months postoperatively. 9 Whereas some have observed poor performance bilaterally, 9 others have suggested asymmetry with better performance in the non–ACL reconstructed limb. 33 These studies support the potential utility of the SLS to identify deficits in neuromuscular control after ACL reconstruction. However, the available data assessing SLS performance after ACL reconstruction report single time points only, and it remains unclear how performance changes over time. This is a limitation of the existing literature because important changes in neuromuscular control (that are potentially reflected in SLS performance) may occur as patients complete rehabilitation, engage in more demanding physical activity, and progress toward return to sports.
The purpose of this study was to assess SLS performance in a large cohort of patients with ACL reconstruction at 6 and 12 months postoperatively by measuring the knee valgus angle. The knee valgus angle is a 2-dimensional measurement of a 3-dimensional motion combining knee abduction/adduction and rotation of the thigh and leg and is significantly affected by hip abduction/adduction and rotation and ankle motion. 6,7,9,19,37 Two-dimensional frontal plane analysis has previously been shown to be a valid 20,31 and reliable 21 measure of the knee valgus angle. Although the cause of knee valgus during SLS is complex, with contributions from all joints in the lower limb kinetic chain, it is a readily measurable parameter that is easily evaluated in the clinical environment and widely recognized as an important marker of performance. 2,5 –7,9,17,33,34,37 The aims of this investigation were to determine whether the knee valgus angle changes between 6 and 12 months after surgery and to compare performance in the operative and nonoperative limbs.
Methods
Approval from the hospital human research ethics committee and informed consent from each participant were obtained.
Patients and Setting
The first 100 eligible consecutive patients undergoing primary hamstring tendon autograft ACL reconstruction who were recruited as part of a larger prospective cohort study were included. The study was performed in a private knee clinic in Australia with 3 experienced knee surgeons contributing participants. The recruitment dates for the patients included in this study were between December 2013 and December 2015, and all patients were aged between 13 and 50 years. For the current study, patients who had undergone previous surgery to the contralateral knee were excluded. Descriptive data for the patient cohort are summarized in Table 1. The mean time of attendance for the scheduled 6- and 12-month postoperative reviews was 6.6 and 12.5 months, respectively.
Patient Characteristics

Data were available on the chondral and meniscal status of 98 patients at the time of surgery. Medial meniscal tears were present in 27 patients. Of these tears, 12 were repaired, 11 were partially resected, and 4 were not addressed surgically. We noted that 2 patients had previously undergone partial medial meniscectomy. Lateral meniscal tears were present in 34 patients. Of these, 2 were repaired, 19 were partially resected, and 13 were not addressed surgically. Chondral damage of International Cartilage Repair Society grades 3 and 4 was present in 6 patients. The majority of patients had no chondral damage in either the patellofemoral compartment (n = 83) or the tibiofemoral compartment (n = 85). Of note, there was no concern for any acute or unstable meniscal or chondral pathology at the time of testing for any patient.
Surgical and Rehabilitation Protocols
Anatomic single-bundle ipsilateral hamstring ACL reconstruction was performed by use of suspensory fixation on the femoral side (EndoButton CL Ultra; Smith & Nephew) and interference fixation with a cannulated screw on the tibial side. The femoral tunnel was drilled via the anteromedial portal.
All patients were provided with the same rehabilitation protocol and guidelines. In the first 3 postoperative weeks, patients were encouraged to reduce knee swelling using rest, ice, compression, and elevation. Full weightbearing was permitted from the first postoperative day, and knee range of motion exercises, including active terminal knee extension, active knee flexion, and prone leg hanging exercises, were commenced. Beginning at 3 weeks, stationary bike, wall squats, straight-leg raises, forward lunges, and hamstring curls were introduced. At 5 weeks, a gymnasium program commenced that included leg press (both double- and single-leg concentric and eccentric), half squats, stationary bike, rowing machine, cross-trainer and step-machine, hamstring curls, bridging (both double and single), calf raises, exercise ball drills for core stability, and leg extensions (after 8 weeks). At 10 weeks, hopping and landing drills were commenced if there was no effusion. At 16 weeks, patients were typically allowed to return to sports-specific drills and activities, including kicking, dribbling, and controlled change of direction. At 26 weeks, patients were encouraged to increase training intensity. No patients had returned to unrestricted sports participation at this time. Return-to-sports clearance was made by the treating surgeon based on the absence of swelling, an essentially full range of motion, a stable knee on clinical examination, good quadriceps strength on clinical examination, control of a single-leg step-down, and the patient’s confidence in his or her knee. A minimum of 4 weeks of unrestricted training was required before return to competitive sports. Although return to sports was criterion-driven, patients would typically return to sports between the 12- and 14-month marks.
SLS Testing
SLS testing was performed by means of a standard protocol. After the task was demonstrated, the patient placed the foot of the nonoperative limb onto a premarked position on a Nintendo Wii Balance Board, which was used as part of the larger study to allow simultaneous capture of center-of-pressure data. With hands on hips, the patient performed a series of 3 SLSs with the instruction to squat as deeply as possible without losing balance or placing the contralateral foot on the ground. The 3 squats were performed within 25 seconds with the aim of achieving a consistent speed. The procedure was then repeated for the operative limb. The second squat for each limb was used for analysis. Video recordings were made in the coronal and sagittal planes at a distance of 170 cm using high-definition, 30 frame-per-second cameras (LifeCam HD-3000; Microsoft Corporation) at the level of the knee. The coronal and sagittal plane recordings were synchronized, and a frame-by-frame analysis of the sagittal plane recording was used to identify 30° of flexion and maximal knee flexion. The corresponding coronal plane frames were then used to measure the knee valgus angle for both flexion angles. The test protocol and valgus angle measurements were performed by 1 of 3 research assistants who adhered to a standardized protocol. Interrater reliability was assessed using a sample of 30 observations at 6 and 12 months for both right and left knees and at 30° of flexion and maximum flexion. Intraclass correlation coefficients were very good to excellent, with a mean of 0.892 and range between 0.748 and 0.990.
Knee flexion was determined as the angle subtended by a line through the lateral malleolus to the knee center and a second line from the knee center to the greater trochanter. We chose 30° so as to have a standardized degree of knee flexion that would be achieved by the entire cohort, which also represented a common flexion angle of the knee at the time of ACL injury. 16
The knee valgus angle was defined as the acute angle subtended by a line from the middle of the ankle to the middle of the knee and a second line from the middle of the knee that bisected the thigh (Figure 1). Data were measured and captured using in-house software developed with the LabVIEW program (National Instruments). A reduced valgus angle (ie, more neutral or more toward varus) is considered to reflect better SLS performance.

The measurement technique for the single-leg squat valgus angle (A) in full extension, (B) at 30° of flexion, and (C) at maximum flexion. The index fingers are on the anterior superior iliac spines.
Data Management and Statistical Analysis
Knee valgus was recorded from the digitized images at both 30° of knee flexion and maximum knee flexion for both limbs. The value of maximum knee flexion was also recorded. These data were analyzed via a 2-factor analysis of variance model with limb (operative, nonoperative) and time (6-month, 12-month follow-up) as repeated factors. Statistical significance was set at P < .05. For each analysis of variance that resulted in a significant F value, post hoc analysis was performed using paired t tests. Cohen's d effect sizes were also calculated and interpreted using the following convention: d = 0.2 considered a small effect size, 0.5 a medium effect size, and 0.8 a large effect size. All analyses were conducted using IBM SPSS Statistics Version 25.0.0.0 and Microsoft Excel (Microsoft Corporation). In addition, the number of patients who had between-limb asymmetry (defined as ≥10°) was tabulated and compared between time points through use of contingency analysis.
Results
Knee Valgus Angle
For the knee valgus angle at 30° of flexion, analysis of variance showed a significant main effect of limb (P = .02) and time (P = .003). Post hoc analysis showed that the mean valgus angle was larger in the operative knee compared with the nonoperative knee at 6 months (5.46° vs 4.29°; P = .008; effect size = 0.27) but there was no difference between limbs at 12 months (Table 2). Post hoc analysis also showed that the mean valgus angle in the operative limb at 30° of flexion was larger at 6 months compared with 12 months (5.46° vs 4.44°; P = .002; effect size = 0.24); however, the difference was slight, with a small effect size. No change in the valgus angle was seen between 6 and 12 months in the nonoperative limb.
Knee Valgus Angles During a Single-Leg Squat a
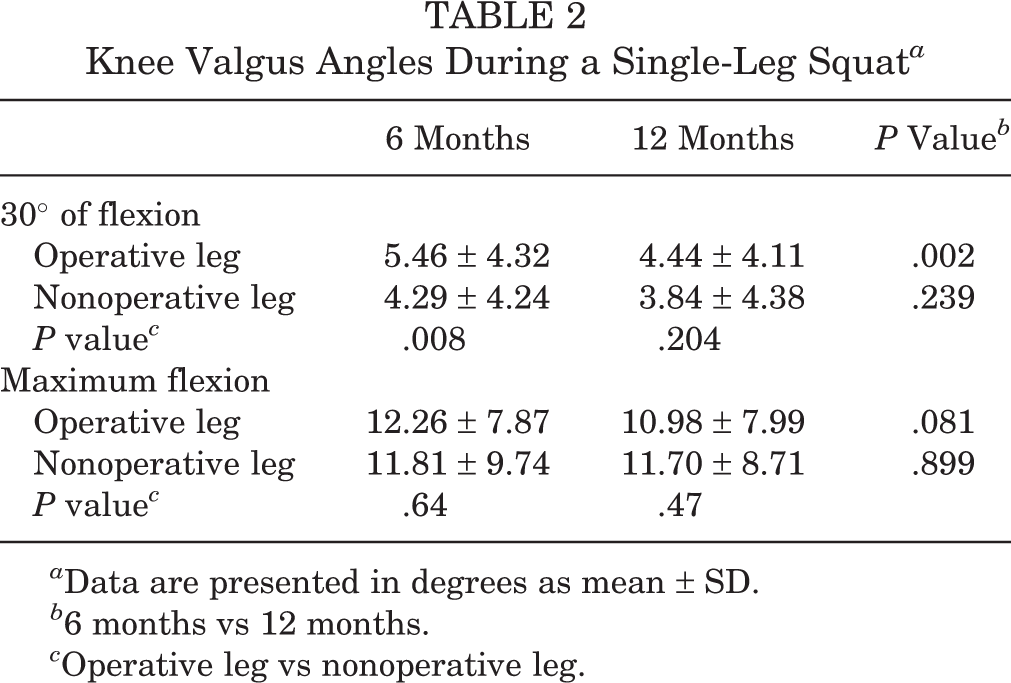
a Data are presented in degrees as mean ± SD.
b 6 months vs 12 months.
c Operative leg vs nonoperative leg.
Patients increased their maximum SLS depth between 6 and 12 months on the operative side by an average of 2° (mean ± SD, 66.1° ± 12.7° vs 68.1° ± 11.3°; P = .011; effect size = 0.26). At both time points, the mean SLS squat depth was slightly lower for the operative limb (66.1° ± 12.7° vs 69.9° ± 12.5° at 6 months and 68.1° ± 11.3° vs 70.1° ± 11.7° at 12 months). The analysis of variance for knee valgus at maximum flexion showed no significant limb, time, or interaction effects (Table 2).
Patients With Valgus Angles Greater Than 10°
At 30° of knee flexion, 13 patients (13%) had a valgus angle in the operative limb that was greater than 10° at 6 months. At the 12-month mark, 10 of these 13 (77%) no longer had a valgus angle greater than 10°. Conversely, 5 patients who had a valgus angle of greater than 10° at 12 months had previously had a valgus angle less than 10° at 6 months. For the group of 13 patients who had a valgus angle greater than 10° at 30° of knee flexion at 6 months, there was a significantly higher mean valgus angle in the nonoperative knee compared with that in the remaining cohort (8.5° vs 3.65°; P < .001). When stratified by sex, at 30° of knee flexion, 8 of the 46 female participants (17%) had a valgus angle greater than 10° at 6 months; this number was reduced to 5 female participants (10.9%) at 12 months. Further, 5 of the 54 male participants (9.3%) had a valgus angle greater than 10° at 6 months, which decreased to 3 male participants (5.6%) at 12 months. The proportion of male and female patients with a valgus angle greater than 10° was not significantly different at 6 months (χ2 = 1.45; P = .228) or 12 months (χ2 = 0.953; P = .329).
Individual Patient Valgus Asymmetry at 6 and 12 Months
At 30° of knee flexion, only 1 patient had asymmetry of knee valgus that was greater than 10° at either time point. At maximum SLS depth, 27% and 36% of patients had asymmetry (>10°) at 6 months and 12 months, respectively. The proportion of patients with asymmetry did not significantly change between time points.
Discussion
The results of this study demonstrate that at the group level, there was minimal difference in the valgus angle during SLS between the 6- and 12-month marks. Although we noted a statistically significant reduction in the valgus angle for the operative limb at 30° of flexion between 6 and 12 months, the change was small and is of doubtful clinical significance. Individual performance, however, was somewhat variable, and group data may not necessarily be applicable at the individual patient level.
In the context of assessing readiness for return to sports, many parameters that have been suggested as indicators of neuromuscular function and performance can be expected to improve with time. The SLS valgus angle is one of many elements in the assessment of neuromuscular function, but in terms of this one element, we found only minimal improvement in the operative limb between the 6- and 12-month marks. Whether this reflects the documented, persistent neuromuscular deficits beyond 12 months and up to 2 years after ACL reconstruction 11,22,24,25,26 is unclear. It is also possible that SLS performance may partly reflect nonmodifiable “deep-seated” neuromuscular capabilities, which could be one explanation for negligible change between 6 and 12 months despite ongoing rehabilitation, as well as the similarity between the operative and nonoperative limbs.
For the group of patients who had high valgus angles (>10°) in the operative limb at 30° of flexion, we noted significantly higher mean valgus angles in the nonoperative limb compared with those of the rest of the cohort. This corresponds with the study by Hall et al, 9 who examined 33 patients at 6 months after ACL reconstruction and demonstrated poor performance in SLS testing in 45% of patients. Poor performance in the contralateral limb was demonstrated by 47% of these patients with poor operative limb performance but by only 12% of patients with satisfactory operative limb performance. Without baseline preinjury SLS performance data, it is not possible to determine whether the 6- and 12-month data represent a deficit relative to baseline performance or whether these neuromuscular deficits are an ongoing preinjury phenomenon. The data from this study suggesting contralateral deficits in at least a subgroup of patients would be consistent with the latter. Longitudinal observation of this patient subgroup with a focus on graft rupture, contralateral ACL injury, and other knee injury rates will aid in understanding of the clinical implications of this observation.
Deficits in core and hip abductor strength may be another factor accounting for poor performance in both the operative and the nonoperative limbs. 2,7 Hip abductor and knee weakness have been shown to be associated with increasing valgus angles during SLS in the ACL-intact population. 6,7 Using 3-dimensional motion analysis and dynamometry, Claiborne et al 6 assessed 30 healthy adults and demonstrated that increasing peak torques in hip abduction, knee flexion, and knee extension were significant predictors of reduced valgus knee movement during SLS. Knee extensor mechanism strength is widely known to be reduced after ACL reconstruction and has been investigated extensively. 1,8,15,18,23,28 Many rehabilitation protocols emphasize the importance of extensor mechanism strengthening, but core and hip abductor strengthening is also likely to be important in patients with ACL reconstruction.
Patients who demonstrate good posture and balance with satisfactory performance or improvement over time would intuitively be expected to have a lower risk of ACL graft failure. Those with little change and ongoing deficits represent a concerning group. Future correlation of performance in SLS testing with return-to-sports rates, ACL failure rates, and patient-reported outcome measures is the ideal data set to assess the utility of SLS as a diagnostic tool, guide return to sports, and help counsel patients. The inclusion of a healthy comparison group would have allowed us to determine whether the consistency in knee valgus angle between 6 and 12 months after ACL reconstruction is typical of an uninjured population. However, the knee valgus angles of patients reported in this study are comparable with those of uninjured patients in previous investigations. 6,31,32
This study had some limitations. The SLS is a complex multiplanar movement, and we assessed only 1 element, the valgus angle. However, breaking this complex movement into its elements has facilitated a more in-depth assessment. This validated measure also lends itself to adoption within the clinical environment. The valgus angle changes with degree of knee flexion, making it challenging to standardize. To account for differing maximum knee flexion angles among patients, we took measurements at a standardized 30° of flexion. Differing patterns of knee valgus have been described, including medialization of the knee relative to the foot compared with lateral displacement of hip and pelvis relative to the knee. 30 These patterns have been correlated with strength deficits in specific muscle groups, but this was not addressed in this investigation. Rehabilitation was not standardized, and the emphasis placed on core and hip abductor strengthening may have varied among patients and affected the results. However, this study had a large number of participants, and we measured changes in the valgus angle during the rehabilitation phase. In addition, all patients were standardized in terms of graft type and the absence of pathology in the contralateral knee.
Conclusion
During a controlled SLS, the group mean knee valgus angle remained essentially constant; further, minimal limb asymmetries were present over the 6- to 12-month postoperative period, which is when athletes typically increase their activity levels. Whether asymmetries are present with more dynamically challenging tasks remains to be determined. At the individual level, more variation was present in performance between time points and between limbs, supporting an individualized approach in return-to-sports considerations. When present, high valgus angles were frequently bilateral, even in the absence of contralateral knee pathology.
Footnotes
Final revision submitted February 29, 2020; accepted March 31, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Epworth HealthCare Human Research Ethics Committee (study No. 57012).