
Abstract
Development and advances in our understanding of basic sciences such as anatomy, biochemistry, histology, and biomechanics have led to a better knowledge of tendon injuries. Likewise, technological advances in available therapies have conditioned the rise of new therapeutic techniques, turning both diagnosis and therapeutic indications into the foundation of treatment for patellar tendon disorders. Furthermore, we often find no correlation between patellar tendon function and structure, as studied and diagnosed from images taken and referred symptoms. This statement proposes an analytic procedure that ensures a specific therapeutic goal instead of applying a specific drug or therapeutic technique, with the aim of establishing parameters that define the kind of tendinopathy clinicians see, taking into account all conditioning factors that may affect a patellar tendinopathy. These include etiological factors, systemic illnesses affecting tendons, local mechanical causes and clinical presentation, range of clinical presentations, symptom persistence, and pain location, as well as those factors described by echography, with or without the presence of neoangiogenesis and location of the pathology, and magnetic resonance imaging. Diagnosing patellar tendinopathies requires deployment of a complex and thorough assessment process for each individual case and should include all variables that basic sciences have provided. Once a diagnosis has been made, a therapeutic strategy that includes all existing variables should be established. The more precise a diagnosis is, the more selective the treatment options become.
Development and advances in our understanding of basic sciences such as anatomy, biochemistry, histology, and biomechanics have led to a better understanding of tendon injuries. 10,23,26,29,30 Improvements in diagnostic processes such as echography and magnetic resonance imaging applied to tendons and, more specifically, the patellar tendon enable specialists to differentiate more precisely any disorder or anomaly in the tendon structure. 7,12,17 Likewise, technological advances in available therapies have led to the rise of new therapeutic techniques, turning both diagnosis and therapeutic indications into the pillars of any adequate treatment of patellar tendon disorders.
Many treatment options are available for patellar tendon pathologies, yet therapeutic indications are often based on personal and professional experience rather than scientific criteria (Table 1). ∥∥ In most cases, whether an applied therapy fails is not a matter of application but rather a matter of indication. It is essential to make a correct diagnosis to apply the appropriate therapy.
List of Treatment Procedures Currently Applied to Tendon Pathologies

We often find no correlation between patellar tendon function and its structure, as studied and diagnosed from images and referred symptoms. 34 We may come across a patellar tendon that is seriously damaged structurally yet the patient is asymptomatic; likewise, an apparently healthy tendon structure might be associated with a painful clinical presentation with severely reduced mobility and functionality. 34 Thus, we cannot consider only one of these parameters as the criterion to establish a therapeutic indication. On this topic, we should point out that patients who have undergone surgery of the patellar tendon in which a bone-tendon-bone ligamentoplasty technique has been applied in anterior cruciate ligament reconstruction have not been more likely to experience tendon tears than other patients with full, original unoperated patellar tendons.
This statement proposes an analytic procedure that enables clinicians to establish a specific therapeutic goal rather than choose a specific drug or therapeutic technique; the aim is to establish parameters that define the type of tendinopathy clinicians encounter, taking into account all factors that may affect a patellar tendinopathy (etiological, mechanical, and clinical) as well as those described by echography and magnetic resonance imaging.
Cause of Patellar Tendinopathy
The patellar tendon may be harmed in 3 ways: a general systemic cause (eg, illness, metabolic disease, rheumatoid condition, drugs); a specific mechanical cause, such as an alteration in the biomechanical axis of the tendon; or a local cause in the tendon itself, such as a partial tear, inadequate repair, or direct trauma.
Systemic Illnesses Affecting Tendons
Systemic illnesses such as diabetes, hypercholesterolemia, collagen-related metabolic disorders, and storage diseases such as high levels of uric acid may condition tendinopathies. Administration of certain drugs such as quinolones, used to boost metalloproteinase activity in tendons, also contributes to the deterioration of tendons. Anabolic drug intake will provoke a sudden and exponential increase in muscular strength without allowing tendons to adapt to such a change. Finally, certain gene expression alterations have been observed that overexpress the presence of metalloproteinases, a process with detrimental effects on type I collagen formation, which causes an imbalance between type I collagen fiber degeneration and renovation, eventually leading to pathology. 8,21,28,36
Mechanical Causes
Alterations in lower limb axis alignment may create highly focused overloads in specific areas of the patellar tendon. For example, hip arthrosis showing limited internal rotation will increase external rotation at the hip during flexion, leading to lateral pain on the patellofemoral joint by impingement at the internal area of the proximal insertion of the patellar tendon due to excessive traction forces. 25 Patellar tendinopathies have also been observed in relation to varus/valgus, recurvatum, alterations of the Q angle, and other lower limb axis malalignment conditions, all of which increase weightbearing forces on specific areas of the patellar tendon.
Local Causes
Patellar tendons may show different morphologic characteristics in terms of length, thickness, or general size, which may lead to a loss of mechanical balance of the force levers acting on the knee. The patellar tendon has a special geometrical shape with respect to the patella and the tibia that creates high levels of traction forces during hyperextension in eccentric contractions. This event leads, in many cases, to a localized tendinopathy on the ventral side of the proximal insertion of the patellar tendon. Thus, the presence of exostosis or distal bone spurs at the patella may be considered a consequence and not a cause of tendon pathology (Figure 1). 6,9,24,38 A patella infera may occur secondary to overstimulation of peritendinous structures, which leads to a retraction of intratendinous collagen fibers and an increase of peritendinous fibrosis.

Sagittal magnetic resonance image including a schematic drawing representing the geometrical shape of the patellar tendon (yellow outline).
Clinical Presentation
Pain may appear suddenly. Patients may feel a stabbing, intense pain, possibly associated with the tendon snapping, and an immediate and relative functional incapacity, all of which may indicate a partial tendon rupture. Other times, pain may gradually settle in, as described by Blazina et al 5 in 1973. Pain first appears after physical activity, followed by a period in which pain is present both at the beginning and at the end of practice sessions, until it is present throughout most of the exercise bout and only subsides well into the rest period after exercise. Finally, patients exercise with continuous pain, and it becomes gradually harder to eliminate pain altogether, even at rest. In these cases, we should consider the possibility of a degenerative process with no infrastructural tear.
Symptom Persistence
According to biological studies on tendon repair, normal physiological healing processes for tendons are possible within the first 8 weeks of injury onset. Beyond those 8 weeks, the biological cell and chemical activity tend to decrease to such an extent that natural healing processes are no longer viable. 34 The Spanish Group for Tendon Consensus document on management of tendinopathies 34 defined tendinopathy as acute when it is present for <8 weeks after symptom onset and chronic when it persists for >8 weeks.
Pain Location
Assessing the type of pain may also indicate the site of pathology. Superficial pain that resolves after subcutaneous injection of a local anesthetic may indicate an affected superficial peritendinous structure. If the patient also describes a burning sensation with dysesthesia, the pain may be of neuropathic origin due to an affected infrapatellar nerve. If pain appears at a deeper level and improves after injection of retrotendinous anesthetic, the tendon itself may be affected on the ventral face of the patellar tendon. 20,27,32,41
Imaging Diagnostic Methods
In acute tendinopathy (<8 weeks), the presence of neoangiogenesis observed on echography may be due to an increase in vascularization considered a normal part of the repair process of a partial rupture. In chronic tendinopathy, neoangiogeneses may be considered pathological and secondary to a faulty tendon repair. Each of these situations requires specific and different therapeutic objectives. 13,33,35,37
Echography or magnetic resonance imaging scans may reveal tendinous and peritendinous anomalies, with images leading us to think that a chronic and systemic pathology is present. Nevertheless, images by themselves are not able to clarify whether the lesion is secondary to a partial tear with abnormal evolution or due to a degenerative stage in a chronic tendinopathy. A careful and thorough medical history will guide us toward the right answer.
Finally, the location of the pathology may affect the treatment goal. Tendon and peritendon structures differ not only in histological and cellular parameters but also in terms of proximal or distal enthesis. The peritendon is the histological tendon structure that is most reactive to mechanical, biochemical, metabolic, and external changes affecting tendons. The peritendon is followed in this sense by the intratendinous fiber area and, last, by entheses. Additionally, the location of the repair process—on the dorsal or ventral surface of the tendon—will affect its evolution because traction forces differ in magnitude on both sides: flexion causes forces to be more intense on the dorsal surface, whereas extension has the same effect on the ventral side. 11,19
For all of the above reasons, we propose that clinicians use an assessment that includes the items listed in Table 2, drawing on the answers to establish an appropriate therapeutic aim. Each response contributes to the most appropriate therapeutic objective based on all parameters considered for each item and not just the information gathered exclusively from diagnostic images.
Items Included in an Assessment to Determine the Most Precise Therapeutic Aim
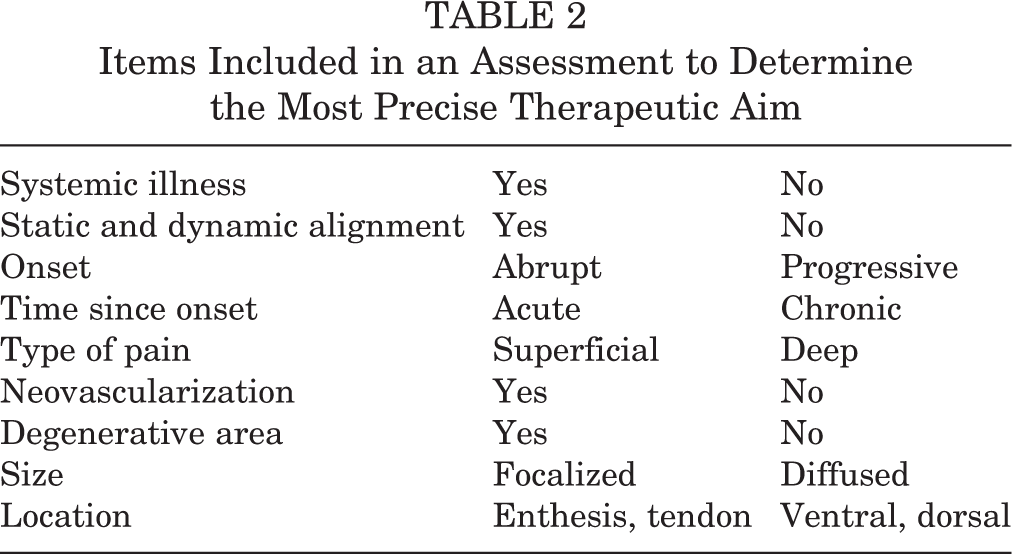
In Figure 2, for instance, we can see how the ventral surface of a patellar tendon is affected. After using the questionnaire, we might find that a patient has no systemic illness or alteration in the joint or bone axis; a deep, acute pain, which appeared suddenly; signs of neovascularization; and no degenerative area on the ventral surface of proximal enthesis, all of which indicate a partial tear in the recovery phase. Treatment aims include supporting the natural healing processes by applying noninvasive physiotherapy and metabolic measures. However, if the results of the assessment indicate that a patient has no systemic illness or alteration in the joint or bone axis, has experienced a progressive onset of pain that has now become chronic and intense, shows signs of neovascularization, and has a degenerative area on the ventral surface of proximal enthesis, these answers would indicate a degenerative area with neovascularization. Treatment would, in this case, aim to revitalize the degenerative area and neutralize neovascularization through application of various techniques such as focused shockwave therapy, percutaneous techniques under echographic guidance, or ventral tenolysis with a rotor.

Sagittal magnetic resonance image showing injury on the ventral side of patellar tendon’s proximal insertion.
Conclusion
Diagnosing patellar tendinopathies requires application of a complex and thorough assessment process for each individual case and should include all variables that basic sciences have provided. Once the diagnosis has been determined, a therapeutic strategy including all existing variables should be established. The more precise a diagnosis is, the more selective the treatment options become. Conducting the assessment thus provides physicians with a well-defined overview of each patient’s situation in a very specific way, leading to an appropriate diagnosis and a tailor-made therapeutic treatment.
Footnotes
Acknowledgment
We thank Mario Wensell for his translating, editing, and proofreading work on this paper.
Final revision submitted May 21, 2020; accepted May 21, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. The publishing of this project was funded by CEMTRO Clinic and the Spanish Group for Research on Muscle and Tendon (GESMUTE). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.