
Abstract
Background:
Biceps tenodesis is a surgical treatment for both superior labral anterior-posterior (SLAP) tears and long head of the biceps tendon (LHBT) abnormalities. Biceps tenodesis can be performed either above or below the pectoralis major tendon with arthroscopic or open techniques.
Purpose:
To analyze the outcomes and complications comparing primary arthroscopic suprapectoral versus open subpectoral biceps tenodesis for either SLAP tears or LHBT disorders.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search strategy based on the PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) protocol was used to include 18 articles (471 patients) from a total of 974 articles identified. Overall exclusion criteria included the following: non–English language, non–full text, biceps tenodesis with concomitant rotator cuff repair, review articles, meta-analyses, and case reports. Data were extracted and analyzed according to procedure type and tenodesis location: arthroscopic suprapectoral biceps tenodesis (295 patients) versus open subpectoral bicepts tenodesis (176 patients).
Results:
For arthroscopic suprapectoral biceps tenodesis, the weighted mean American Shoulder and Elbow Surgeons (ASES) score was 90.0 (97 patients) and the weighted mean Constant score was 88.7 (108 patients); for open subpectoral biceps tenodesis, the mean ASES score was 91.1 (199 patients) and mean Constant score was 84.7 (65 patients). Among the 176 patients who underwent arthroscopic biceps tenodesis, there was an overall complication rate of 9.1%. Among the 295 patients who underwent open biceps tenodesis, there was an overall complication rate of 13.5%. Both residual pain (5.7% vs 4.7%, respectively) and Popeye deformity (1.7% vs 1.0%, respectively) rates were similar between the groups. Open subpectoral biceps tenodesis had higher reoperation (3.0% vs 0.0%, respectively), wound complication (1.0% vs 0.0%, respectively), and nerve injury (0.7% vs 0.0%, respectively) rates postoperatively. A meta-analysis of 3 studies demonstrated that both methods had similar ASES scores (P = .36) as well as all-cause complication rates (odds ratio, 0.76 [95% CI, 0.13-4.48]; P = .26).
Conclusion:
Patients undergoing arthroscopic suprapectoral biceps tenodesis for either SLAP tears or LHBT abnormalities had similar outcome scores and complication rates compared with those undergoing open subpectoral biceps tenodesis. Additionally, both residual pain and Popeye deformity rates were similar between the 2 groups.
The long head of the biceps tendon (LHBT) is often implicated in shoulder injuries such as superior labral anterior-posterior (SLAP) lesions, rotator cuff tears, and tendinitis or tenosynovitis. 17 Nonoperative treatment consists of rest, activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, and corticosteroid injections. When nonoperative treatment fails, surgical options such as SLAP repair, biceps tenotomy, or tenodesis are utilized. 22,31,32,44 Depending on the underlying injury and associated lesions, these procedures can either be performed in a concomitant or isolated fashion. For isolated lesions of the biceps tendon and SLAP tears in older and lower-demand patients, the choice of biceps tenotomy versus tenodesis, along with the location and technique utilized, is often debated. 64 The current literature suggests that clinical and functional outcomes are similar; however, tenotomy results in a greater risk of developing a cosmetic “Popeye” deformity along with biceps cramping or spasms. 10,18,25,33 Supporters of biceps tenodesis advocate several advantages over tenotomy, such as preservation of the shape and contour of the biceps, preservation of strength, and maintenance of the length-tension relationship. 3,4,33,63 The use of biceps tenodesis increased by 50% among the Midwest, Northeast, South, and West regions of the United States between 2008 and 2011 and reflects its growing popularity. 37,60 Tenodesis is also emerging as another option for the management of young athletic throwers and high-demand patient populations with isolated SLAP tears or LHBT disorders. 43
Biceps tenodesis can be performed arthroscopically or open, with many variations on the type (eg, interference screw fixation vs suture anchor fixation) and location (eg, suprapectoral with arthroscopic technique vs subpectoral with open technique) of fixation. 4,53 Although clinical and functional outcomes are generally satisfactory, the optimal biceps tenodesis technique is still widely debated in the literature. 1,13,28,35 Several clinical trials have directly compared the functional outcomes between different tenodesis techniques; however, a comparison of treatment outcomes and surgical complications was not possible because of low sample sizes. 21,61 A systematic review of aggregated cases can assess both the functional outcomes and the surgical complications as applied to a larger cohort of patients.
The purpose of this study was to conduct a systematic review and meta-analysis of the literature to compare outcomes (American Shoulder and Elbow Surgeons [ASES] and Constant scores) and complication rates between primary arthroscopic suprapectoral biceps tenodesis and open subpectoral biceps tenodesis without concomitant rotator cuff repair to treat either SLAP tears or LHBT disorders.
Methods
Search Strategy
A systematic and rigorous search strategy was developed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) protocols (Figure 1). 40,59 This strategy yielded appropriate peer-reviewed articles via a 4-phase systematic review. In phase 1 (“identification”), electronic databases were searched to find relevant biceps tenodesis articles. MEDLINE (PubMed), Embase (Elsevier), and Cochrane Library databases were accessed and searched on December 15, 2017, with the following Boolean search terms: ((((Suprapectoral Biceps tenodesis OR Subpectoral Biceps tenodesis OR Biceps tenodesis OR Arthroscopic biceps tenodesis OR Open biceps tenodesis OR tenodesis OR mini open biceps tenodesis) AND (Pain OR Range of Motion OR ROM OR Popeye OR Muscle Cramp OR satisfaction rate OR postoperative American Shoulder and Elbow Surgeon Scores OR satisfaction score OR ASES OR Complications OR Revisions OR SANE OR UCLA OR Constant OR Constant-Murley OR DASH OR RCQOL OR WORC OR WOSI OR Simple Shoulder Test OR outcomes))). To increase sensitivity, no filter was used during the database searches.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart exhibiting the search strategy to identify articles for inclusion.
Eligibility Criteria
All search returns were extracted and examined for relevance, and duplicated search returns were discarded. In phase 2 (“screening”), titles and abstracts were screened for relevance. Bibliographies of screened articles were also manually searched for other relevant articles that were potentially screened out of the database algorithms. Articles were filtered out based on the following overall exclusion criteria: (1) non-English text, (2) only the abstract was available, (3) treatment was arthroscopic rotator cuff repair with concomitant biceps tenodesis, (4) review article or meta-analysis, or (5) case report. The treatment methods reviewed were arthroscopic suprapectoral biceps tenodesis, open subpectoral biceps tenodesis, and mini-open subpectoral biceps tenodesis. For this review, the mini-open technique was grouped together with the open technique. While reviews and meta-analyses were excluded because of the aggregate nature of data from other primary studies, a bibliography review of these relevant reviews and meta-analyses added 2 primary studies previously not included in the original search criteria.
Article Review
In phase 3 (“eligibility”), all articles eligible after the screening phase were fully reviewed and evaluated for (1) inclusion criteria, (2) relevant data on clinical outcome scores, and (3) postoperative complications. All articles were reviewed, assessed, and data mined by 2 independent evaluators (Z.J.D., C.Y.). All results were then compared to ensure consistency and accuracy. Any conflicts or issues were resolved by a second review of the articles, and in the event of further disagreement, the final decision was made by the senior author (X.L.).
Data Extraction and Assessment
In phase 4 (“included”), articles that met inclusion criteria were analyzed for quality, and data were extracted to be used for the systematic review. The following items were extracted from the included articles: author, publication year, journal title, level of evidence, study design, surgical procedure, number of patients, mean age at the time of surgery, sex, mean follow-up period, concomitant procedures, outcome scores, and complications. In studies that included multiple surgical treatment methods, relevant data pertaining to the surgical procedures of this study were stratified and analyzed independently.
Aggregated mean outcome scores were calculated for the arthroscopic biceps tenodesis and open biceps tenodesis groups for comparison purposes. Scores were excluded if (1) the article failed to report a particular outcome score, (2) they were reported as a median value, or (3) they were found to be questionable and/or inconsistent with other outcome scores reported in the same article. With these criteria, the ASES scores reported by Faruqui et al 15 (ASES score was reported as a median value) and Shen et al 55 (ASES score of 33.6 conflicted with a Constant score of 89.1 reported within the same article) were excluded.
All complications reported by the included studies were consolidated into a list for comparison. An additional 2 articles were excluded in the final analysis. Mazzocca et al 36 did not differentiate postoperative complications after biceps tenodesis without concomitant rotator cuff repair, although they reported outcome scores in this manner. The study by Chalmers et al 9 was excluded, as the authors did not report on postoperative complications.
Statistical Analysis
Patient characteristics as well as subjective and objective outcomes were collected and analyzed. There were 3 studies 19,21,61 that compared outcomes between arthroscopic suprapectoral and open subpectoral biceps tenodesis and were therefore chosen to be included in a meta-analysis. The remaining studies were descriptively analyzed. Data were collected in Excel Version 1710 (Microsoft), and all statistical analyses were performed utilizing Review Manager 5.3 software (Cochrane). Random-effects models were chosen in an effort to account for differences among studies in regard to patient characteristics, surgical indications, and study methodology. 6 Heterogeneity analysis of the included studies was conducted using I 2 , which represents an estimated percentage of error attributed to interstudy variation. 23 An I 2 value of <25% was deemed to be of low heterogeneity, 25%-75% was moderately heterogeneous, and >75% was highly heterogeneous. 24 Results were expressed as mean differences for continuous variables and odds ratios (ORs) for dichotomous variables with 95% CIs. A P value of <.05 was deemed statistically significant.
Quality Assessment
To assess the quality of each study that was included in the analysis, the ROBINS-I (Risk of Bias in Non-Randomized Studies–of Interventions) was determined. 56 This risk-of-bias tool includes 7 criteria: (1) bias due to confounding, (2) bias in the selection of participants into the study, (3) bias in the classification of interventions, (4) bias due to deviations from intended interventions, (5) bias due to missing data, (6) bias in the measurement of outcomes, and (7) bias in the selection of reported results. Each criterion was rated as low, moderate, high, or critical risk of bias. The category was labeled as unclear when insufficient data were provided to permit a judgment (Table 1).
Risk of Bias

Results
After a careful review of the available literature, ten level 4 studies, ¶ seven level 3 studies, 5,8,11,14,19,21,61 and one level 1 study 54 were included in the final analysis. The 18 included studies spanned a period from May 2009 to February 2018 and included assessments of arthroscopic suprapectoral biceps tenodesis, open subpectoral biceps tenodesis, and mini-open subpectoral biceps tenodesis. Open subpectoral biceps tenodesis articles were aggregated together with the mini-open subpectoral biceps tenodesis articles to form a combined open subpectoral biceps tenodesis group. There were 8 studies that evaluated arthroscopic biceps tenodesis and 13 studies that evaluated open biceps tenodesis. Of these, 3 studies directly compared arthroscopic and open biceps tenodesis.
Various outcome measures were used, including the ASES score, Constant score, Disabilities of the Arm, Shoulder and Hand score, Oxford Shoulder Score, Rowe score, 12-Item Short Form Health Survey, Simple Shoulder Test, Single Assessment Numerical Evaluation, University of California Los Angeles shoulder score, visual analog scale, and patient satisfaction. The majority of studies used either the ASES or Constant score to evaluate patient outcomes.
Overall, 471 patients were available for follow-up, with 176 in the arthroscopic biceps tenodesis group and 295 in the open biceps tenodesis group. The weighted mean age at the time of surgery was 54.0 years (range, 22-69 years), with a range of follow-up of 12 to 68 months, for the arthroscopic biceps tenodesis group. For the open biceps tenodesis group, the weighted mean age at the time of surgery was 46.8 years (range, 16-73 years), with a range of follow-up of 6 to 109 months. The number of patients per study ranged from 15 to 49 in the arthroscopic group and 11 to 39 in the open group (Table 2). Given the limitation of data provided by the studies reviewed, a mean ± SD for age or follow-up across studies could not be accurately calculated.
Patient Demographics, Outcome Scores, and Complication and Reoperation Rates a

a ASES, American Shoulder and Elbow Surgeons.
Arthroscopic Suprapectoral Biceps Tenodesis
Overall, 8 studies evaluated clinical outcomes after arthroscopic biceps tenodesis (Table 3). 5,11,15,19,21,26,55,61 There were 4 studies 5,26,55,61 (108 patients) that used the Constant score, with a weighted mean value of 88.7. Based on the 5 studies 11,19,21,26,61 (97 patients) with eligible ASES scores reported, the aggregated weighted mean ASES score was 90.0. Of the 176 patients, there were no intraoperative complications. The overall complication rate was 9.1%. Complications reported postoperatively included 10 (5.7%) cases of persistent pain, 3 (1.7%) Popeye deformities, and 3 (1.7%) cases of postoperative stiffness. None of the studies reported infections, nerve injuries, or the need for reoperation (Table 5).
Various concomitant procedures were reported in 6 of the studies, 11,19,21,26,55,61 with the most common being subacromial decompression (98/176 or 55.7%), distal clavicle excision (16/176 or 9.1%), and labral debridement (8/176 or 4.55%). There were 2 studies 5,15 that reported no concomitant procedures.
Data for Included Arthroscopic Suprapectoral Biceps Tenodesis Studies a

a AC, acromioclavicular; ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; F, female; LHB, long head of the biceps tendon; LOE, level of evidence; M, male; N/A, not available; SAD, subacromial decompression; SANE, Single Assessment Numerical Evaluation; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale; VR-36, Veterans RAND 36-Item Health Survey.
b Data are shown as mean (range), mean ± SD, or mean ± SD (range).
c Data are shown as mean or mean ± SD.
d Data are shown as mean, mean ± SD, or mean ± SD (range) unless otherwise indicated.
e Median value reported (not used to calculate mean score).
f Inconsistent with other outcome scores reported by authors (not used to calculate mean score).
Open Subpectoral Biceps Tenodesis
A total of 13 studies were identified that evaluated clinical outcomes after open biceps tenodesis (Table 4). # Overall, 9 studies 8,14,19 –21,47,57,58,61 (199 patients) used the ASES score as a measure of clinical outcomes, with a weighted mean value of 91.1. Additionally, 2 studies 50,61 (65 patients) used the Constant score, with a weighted mean value of 84.7. The overall complication rate was 13.5%. There were 9 (3.0%) reoperations, 8 (2.7%) cases of postoperative stiffness, 14 (4.7%) cases of residual pain, 3 (1.0%) Popeye deformities, 3 (1.0%) cases of postoperative wound erythema indicative of an infection, 2 (0.7%) nerve injuries, and 1 (0.3%) traumatic rupture (Table 5). Of the 9 reoperations, 6 were reported by Schroder et al, 54 2 by Green et al, 21 and 1 by Chalmers et al. 8 Schroder et al reported that 3 patients underwent labral repair, 2 underwent capsular release, and 1 underwent acromioclavicular (AC) joint resection. Green et al reported that 2 patients underwent a reoperation for rotator cuff tears that occurred at 5 and 10 years after their biceps tenodesis. Chalmers et al 8 reported that 1 patient underwent a reoperation for lysis of adhesions and manipulation under anesthesia. Moreover, 11 studies ** reported information on whether concomitant procedures were performed, with subacromial decompression (115/226 or 50.9%) and distal clavicle resection (27/226 or 11.9%) being the 2 most common procedures reported.
Data for Included Open and Mini-Open Subpectoral Biceps Tenodesis Studies a
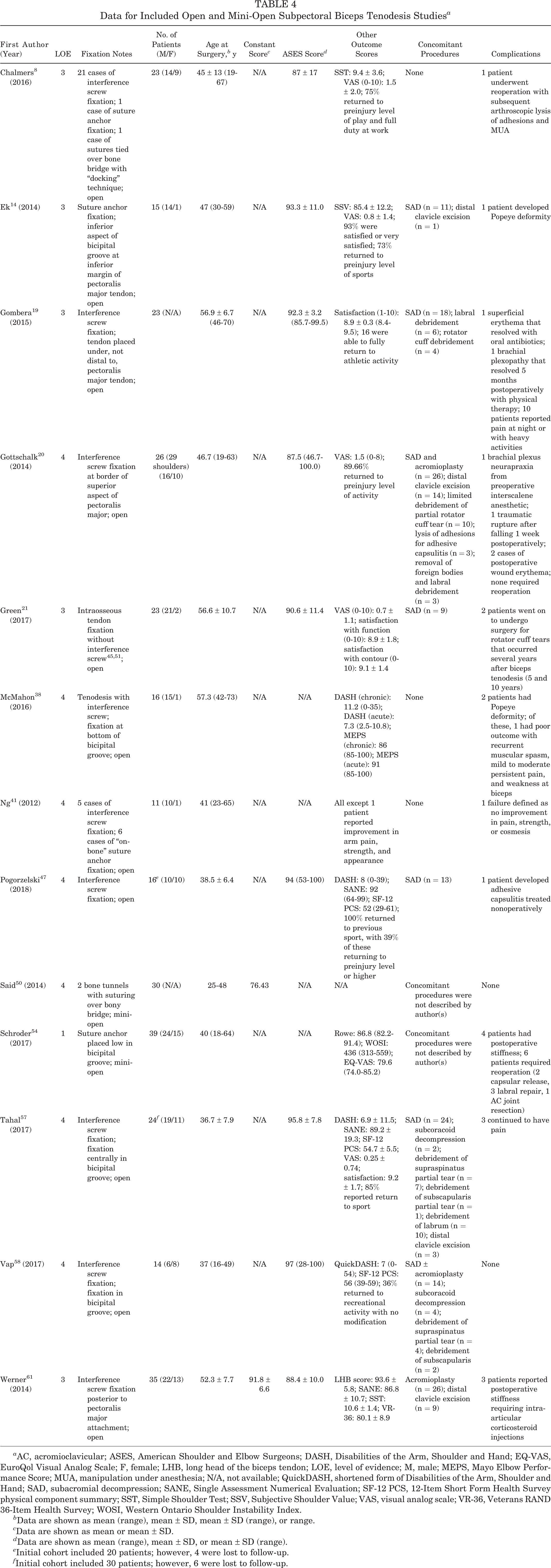
a AC, acromioclavicular; ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; EQ-VAS, EuroQol Visual Analog Scale; F, female; LHB, long head of the biceps tendon; LOE, level of evidence; M, male; MEPS, Mayo Elbow Performance Score; MUA, manipulation under anesthesia; N/A, not available; QuickDASH, shortened form of Disabilities of the Arm, Shoulder and Hand; SAD, subacromial decompression; SANE, Single Assessment Numerical Evaluation; SF-12 PCS, 12-Item Short Form Health Survey physical component summary; SST, Simple Shoulder Test; SSV, Subjective Shoulder Value; VAS, visual analog scale; VR-36, Veterans RAND 36-Item Health Survey; WOSI, Western Ontario Shoulder Instability Index.
b Data are shown as mean (range), mean ± SD, mean ± SD (range), or range.
c Data are shown as mean or mean ± SD.
d Data are shown as mean (range), mean ± SD, or mean ± SD (range).
e Initial cohort included 20 patients; however, 4 were lost to follow-up.
f Initial cohort included 30 patients; however, 6 were lost to follow-up.
Complications a

a Data are shown as n (%).
b Subsequent to a fall 1 week after surgery.
Method of Fixation Used in Arthroscopic Suprapectoral and Open Subpectoral Biceps Tenodesis
As seen in Tables 3 and 4, the fixation method and hardware used in each of the 18 studies varied, but the majority used interference screw fixation (277/471 or 58.8%). The second most commonly used fixation method was suture anchors (125/471 or 26.5%). In particular, 180 of the 295 (61.0%) patients in the open group and 97 of the 176 (63.6%) patients in the arthroscopic group underwent interference screw fixation.
Meta-analysis: Mean ASES Score
Only 3 studies 19,21,61 collected mean ASES scores comparing arthroscopic suprapectoral with open subpectoral biceps tenodesis. The meta-analysis included a total of 65 patients in the arthroscopic suprapectoral group compared with 81 in the open subpectoral group. There was a mean difference of 1.63 (95% CI, –5.13 to 1.87) in favor of ASES scores in patients who underwent open subpectoral biceps tenodesis; however, this failed to reach statistical significance (P = .36) with moderate heterogeneity (I 2 = 37%) (Figure 2).

Mean ASES scores: arthroscopic suprapectoral versus open subpectoral biceps tenodesis. AS, arthroscopic; IV, inverse variance.
Meta-analysis: All-Cause Postoperative Complications
All-cause postoperative complications were reported by all 3 studies. Green et al, 21 however, did not have any complications in the arthroscopic suprapectoral group. Although patients who underwent arthroscopic biceps tenodesis had a lower odds of experiencing a complication than those who underwent open biceps tenodesis, the result failed to reach statistical significance (OR, 0.76 [95% CI, 0.13-4.48]; P = .26) with low heterogeneity (I 2 = 20%) (Figure 3).

All-cause postoperative complications: arthroscopic suprapectoral versus open subpectoral biceps tenodesis. AS, arthroscopic; M-H, Mantel-Haenszel.
Discussion
Clinical Results
The present systematic review and meta-analysis compared the clinical outcomes and postoperative complications of 2 common surgical methods for the treatment of SLAP or biceps tendon injuries: arthroscopic suprapectoral biceps tenodesis and open subpectoral biceps tenodesis. The meta-analysis demonstrated that both arthroscopic suprapectoral and open subpectoral biceps tenodesis had similar ASES scores (P = .36). The weighted mean ASES score for arthroscopic biceps tenodesis was 90.0, while the weighted mean ASES score for open biceps tenodesis was 91.1. Taking into consideration a previously reported minimal clinically important difference of 11 points for the ASES score, 48 the scores were comparable between both methods of tenodesis, as there was a 1.1-point difference. The mean Constant score for the arthroscopic group was 88.7, while the mean Constant score for the open group was 84.7, which is similar between the 2 groups. Although our study did not show a statistically significant difference between complication rates (arthroscopic suprapectoral: 9.1%; open subpectoral: 13.5%), this may be related to sample size limitations. However, our more in-depth analysis did show that the arthroscopic suprapectoral biceps tenodesis group had 24% lower odds of developing a complication compared with the open subpectoral biceps tenodesis group (OR, 0.76 [95% CI, 0.13-4.48]; P = .26), which may be a clinically relevant finding. This is likely related to the higher reoperation (3.0% vs 0.0%, respectively), wound complication (1.0% vs 0.0%, respectively), and nerve injury (0.7% vs 0.0%, respectively) rates seen in the open subpectoral biceps tenodesis group.
Our results are in line with a previous systematic review by Abraham et al 1 comparing subjective and objective outcomes between open and arthroscopic biceps tenodesis in the setting of rotator cuff repair. The authors created a grading system to analyze their included studies and found “good to excellent” results in 98% of cases. 1 Additionally, regarding functional outcome scores, our findings are similar to a recent systematic review by Hurley et al 27 in which the authors found no difference in functional ASES or Constant scores. However, Hurley et al demonstrated a slightly higher complication rate in the arthroscopic group, with 1 study demonstrating a higher rate of overall complications (P < .05), 30 whereas another showed a higher rate of stiffness (P < .05). 62 An important distinction from our study is that the aforementioned reviews did not exclude rotator cuff repair and included a number of different tenodesis locations (subpectoral, suprapectoral, and intracuff). The articles included in our study only consist of patients undergoing primary arthroscopic suprapectoral biceps tenodesis or open subpectoral biceps tenodesis for either SLAP tears or biceps abnormalities and no associated rotator cuff repair.
Tenodesis Location and Fixation Method
As seen in Tables 3 and 4, the fixation method and hardware of each of the 18 articles varied, but the majority used interference screw fixation (277/471 or 58.8%). The second most commonly used fixation method was suture anchors (125/471 or 26.5%). In particular, 180 of the 295 (61.0%) patients in the open group and 97 of the 176 (63.6%) patients in the arthroscopic group underwent interference screw fixation. Most of the current literature suggests that interference screw fixation is superior to other methods, although some debate still exists. 28,35,36,39 Millett et al 39 compared open subpectoral biceps tenodesis with suture anchor versus interference screw fixation and found that the suture anchor group had a higher rate of reported pain, although both groups demonstrated similar improvements in their modified Constant scores. Scheibel et al 53 compared arthroscopic soft tissue tenodesis versus bony fixation anchor tenodesis and found significantly better long head of the biceps tendon (LHB) scores with bony fixation anchor tenodesis (80.9 vs 91.8, respectively); however, they did not find a statistically significant difference in overall Constant scores (75.0 vs 78.3, respectively) between the 2 groups.
It is expected that individual surgeons have personal preferences on how to perform biceps tenodesis, along with which type of hardware or size to use as well as tensioning technique, and this is a source of heterogeneity that should be considered when looking at our results, especially regarding specific postoperative complications. Future studies on fixation or tensioning methods and hardware may shed more light on the optimal fixation method and hardware size that will improve outcomes and minimize failure.
The exact site of tenodesis fixation is another source of heterogeneity, and the effect that it plays on our results is difficult to assess statistically because of the lack of detail provided by the authors as well as the small sample sizes. Within the arthroscopic suprapectoral group, fixation sites were all described as somewhere around the top of the bicipital groove, which may be intra- or extra-articular in location, albeit with differing terminology. In contrast, some of the open biceps tenodesis studies either did not clarify fixation location, stated only that it was subpectoral, or described that the site was somewhere within the bicipital groove itself below the pectoralis major insertion. The debate regarding the best site of fixation is ongoing, as there is concern that more proximal tenodesis locations result in persistent bicipital groove or residual pain and the need for revision. 7,34,52 Sanders et al 52 found that proximal tenodesis resulted in significantly higher rates of revision (45.4%) compared with distal tenodesis techniques. However, their study included patients with rotator cuff tears and other concomitant shoulder injuries, which could bias their results and revision rates. Conversely, Brady et al, 7 in a large multicenter study, concluded that a tenodesis site at the articular margin performed arthroscopically in the groove resulted in a low rate of residual pain and substantially low reoperation rate (4.1%). Unlike our study, both of these studies included patients with concomitant rotator cuff repair. In the patients with either SLAP tears or biceps tendon abnormalities and no rotator cuff tears, we found no difference in the outcome (residual pain or Popeye deformity) between the 2 different locations of biceps tenodesis (arthroscopic suprapectoral vs open subpectoral). With regard to residual pain in particular, in the studies reviewed, it could be specified further either as residual pain from the bicipital groove or residual pain from all causes. It is very difficult to clinically differentiate groove versus nongroove pain. In our systematic review of primary arthroscopic or open techniques for either SLAP tears or LHBT abnormalities, we found no difference in residual groove pain, residual nongroove pain, or residual all-cause pain between arthroscopic suprapectoral and open subpectoral biceps tenodesis.
Complications
A number of complications were reported among the articles (see Table 5). The open group was observed to have individual complications that were not seen in the arthroscopic group and vice versa. Of the various individual complications, there was a higher rate of reoperation associated with open biceps tenodesis (3.0%) compared with the arthroscopic group (0.0%). However, none of these reoperations were related to the tenodesis procedure, as the majority of these complications were reported by Schroder et al 54 and included 2 patients who underwent capsular release, 3 patients who underwent labral repair, and 1 patient who underwent AC joint resection. Green et al 21 reported that 2 patients required reoperations at 5 and 10 years after their biceps tenodesis, both for rotator cuff repair. They suggested that the higher incidence of reoperations was seen because of their longer than average follow-up of 4.5 years. Chalmers et al 8 reported that 1 patient required a reoperation for subsequent arthroscopic lysis of adhesions and manipulation under anesthesia. The secondary operative procedures reported in these studies were unrelated to biceps tenodesis, and taking this information into consideration, we found no difference in the reoperation rate associated with open biceps tenodesis versus arthroscopic biceps tenodesis for the treatment of SLAP tears and LHBT-related abnormalities.
Arthroscopic biceps tenodesis had a similar incidence of residual pain compared with open biceps tenodesis (5.7% vs 4.7%, respectively). The source of persistent pain after biceps tenodesis is controversial, as mentioned above, with previous literature showing conflicting results. Jeong et al 30 noted persistent bicipital tenderness in 24.2% of patients who underwent arthroscopic intracuff tenodesis as compared with 2.5% who underwent open subpectoral tenodesis (P = .012). Of note, they used soft tissue tenodesis for their arthroscopic group. Conversely, Duchman et al 13 noted no significant difference in the frequency of bicipital groove tenderness between the open and arthroscopic groups (20.0% vs 10.0%, respectively; P = .437). The differences in bicipital groove pain reported in the literature could be related to the technique, patient factors, or the ability to accurately diagnose or report residual groove pain from a physical examination.
The rate of postoperative stiffness was slightly lower for the arthroscopic versus open biceps tenodesis group (1.7% vs 2.7%, respectively). This is in contrast to a 2014 study by Werner et al 62 in which the authors examined 249 patients, of whom 143 underwent open subpectoral biceps tenodesis and the remaining 106 underwent arthroscopic suprapectoral biceps tenodesis. These authors found a significantly increased incidence of postoperative stiffness in the arthroscopic group compared with the open group (17.9% vs 5.6%, respectively; P = .002). They suggested several possibilities that could explain this outcome, including increased soft tissue manipulation and dissection inherent to the arthroscopic suprapectoral technique, increased fluid extravasation, and increased risk of bleeding in the region of the bicipital sheath. However, in our comprehensive review of the literature, we found very low rates of postoperative stiffness in both groups after biceps tenodesis.
Several unique complications were noted in the open biceps tenodesis group that were not seen in the arthroscopic group. Notably, there were 3 cases of postoperative wound erythema suggestive of a surgical site infection (2 from Gottschalk et al 20 and 1 from Gombera et al 19 ) and 2 nerve-related injuries (1 from Gombera et al and 1 from Gottschalk et al). Both of these complications might be related to the nature of the open biceps tenodesis technique being a more invasive procedure. An increased rate of infections after open versus arthroscopic surgery is a well-noted phenomenon in rotator cuff repair. Jensen et al 29 evaluated complications after open and arthroscopic rotator cuff repair and found that patients in the open group were significantly more likely to incur an infection within 6 months postoperatively versus the arthroscopic group (0.86% vs 0.37%, respectively; P < .001). Nho et al 42 examined complications after subpectoral biceps tenodesis, and while the overall rate was low (2.0%), the complications that did result were severe, including a patient who developed a deep wound infection necessitating irrigation and debridement with intravenous antibiotics. Similarly, Abtahi et al 2 examined complications after open subpectoral biceps tenodesis and found a complication rate of 7%, with 4 (4%) cases of superficial wound infections.
Furthermore, the open approach may lend itself to more accidental damage to nerves. In our review, Gombera et al 19 reported that 1 patient developed brachial plexopathy with triceps weakness, and Gottschalk et al 20 reported that 1 patient developed brachial plexus neurapraxia that was eventually determined to be the result of preoperative interscalene anesthesia. Previous literature has described cases of nerve injuries after open biceps tenodesis. Rhee et al 49 looked at 4 patients who developed iatrogenic brachial plexus injuries after open subpectoral biceps tenodesis. The close proximity of the terminal branches of the plexus to the tenodesis site, in particular the musculocutaneous nerve, increases the risk of inadvertent damage via retraction. 12
Concomitant Procedures
Many biceps tenodesis procedures are performed in patients with concomitant rotator cuff tears, which may influence the overall results. To reduce bias and rotator cuff repair as a confounding factor, articles with concomitant rotator cuff repair were excluded from our systematic review during both the screening and the eligibility phases of article selection. A total of 6 of the arthroscopic biceps tenodesis studies reported concomitant procedures during surgery; the most common of these were subacromial decompression, acromioplasty, and distal clavicle excision. 11,19,21,26,55,61 Furthermore, 8 of the open biceps tenodesis articles reported concomitant procedures that were performed, with the most common being subacromial decompression, acromioplasty, and distal clavicle excision. 14,19 –21,47,57,58,61 Given the frequency of concomitant procedures and the qualitative similarity of the number and types of concomitant procedures between the 2 surgical method groups (excluding rotator cuff repair), it is likely that these concomitant procedures have minimal influence over the differences in clinical outcomes and rates of complications between arthroscopic and open biceps tenodesis. However, it was not possible for us to stratify patients between those who underwent biceps tenodesis with versus without any concomitant procedures, so it is also possible that the benefits seen in patients undergoing biceps tenodesis (arthroscopic or open) are also related to these commonly performed concomitant procedures.
Limitations
The results of the present study should be interpreted within the limitations associated with the study design. The data were extracted from studies that were performed at different time points, with surgery performed by many different surgeons on patients of varying ages and surgical indications as well as varying concomitant procedures. Additionally, considering that there are a number of different standardized shoulder outcome scores utilized in the assessment of outcomes after shoulder surgery, each of the 18 articles included in this study used its own unique combination of standardized scores to assess their clinical outcomes. We chose to use the ASES and Constant scores in this review because of their consistent application in the majority of included articles. As such, much of the other clinical outcome information obtained via other standardized clinical outcome scores was reported but not analyzed.
When comparing ASES scores, the arthroscopic biceps tenodesis group had fewer patients than the open biceps tenodesis group (roughly a 1:2 ratio) and vice versa when comparing Constant scores (roughly a 3:1 ratio). These uneven sample sizes led to differences in sample size, power, and variance, which should still be taken under consideration even if only the calculated means were used as the measure of comparison between the 2 groups. In addition, the type of injury being treated (SLAP tear vs LHBT disorder) was not always explicitly stated, and differences in these 2 patient populations in terms of demographics and patient factors may have biased the study results. Unfortunately, given the current body of literature, we were unable to separate these 2 patient groups and analyze the data separately.
Last, the comparison of complication rates between arthroscopic and open biceps tenodesis should be considered in light of 3 problems. First, the sample size was relatively small. Second, the documentation of complications was not uniform between studies, and individual studies disproportionately contributed more to select complications. In particular, the double-blind study from Schroder et al 54 contributed to 6 of the 9 cases of reoperations in the open biceps tenodesis group. Alternatively, there were articles that neither addressed nor reported on any patient complications. Third, the fixation hardware and techniques used by the surgeons varied widely and added to the difficulty of comparing the results and controlling for confounding variables. These considerations should be fully understood before drawing conclusions about the risks of arthroscopic versus open biceps tenodesis.
Conclusion
Patients undergoing arthroscopic suprapectoral biceps tenodesis for either SLAP tears or LHBT abnormalities had similar outcome scores and complication rates compared with open subpectoral biceps tenodesis. Furthermore, both residual pain (groove or nongroove pain) and Popeye deformity rates were similar between the 2 groups. Future studies with larger sample sizes and without concomitant procedures (subacromial decompression, AC joint resection, etc) are warranted to further investigate the postoperative outcomes and complication profiles between these 2 treatment methods.
Footnotes
Final revision submitted March 17, 2020; accepted March 31, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: X.L. has received consulting fees from DePuy, FH Ortho, and Tornier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.