
Abstract
Purpose:
To (1) better define the anatomy of the proximal shoulder in relation to the long head of the biceps tendon, (2) compare the length-tension relationship of the biceps tendon in the native shoulder with that after arthroscopic and open tenodesis techniques using interference screws, and (3) provide surgical recommendations for both procedures based on study findings.
Study Design:
Descriptive laboratory study.
Methods:
Twenty fresh-frozen cadaveric shoulders were dissected for analysis. Initial anatomic measurements involving the proximal long head of the biceps tendon (BT) were made, which included: the labral origin to the superior bicipital groove (LO-SBG), the total tendon length (TTL), the musculotendinous junction (MTJ) to the inferior pectoralis major tendon border, the MTJ to the superior pectoralis major tendon border, and the biceps tendon diameter (BTD) at 2 different tenodesis locations. These same measurements were made again after completing a simulated suprapectoral arthroscopic and open subpectoral tenodesis, both with interference screw fixation. Statistical comparisons were then made between the native anatomy and that after tenodesis, with the goal of assessing the accuracy of re-establishing the normal length-tension relationship of the long head of the BT after simulated arthroscopic suprapectoral and open subpectoral tenodesis with tenodesis screws.
Results:
For all cadavers, the mean TTL was 104.1 mm. For the arthroscopic suprapectoral technique, the mean LO-SBG was 33.6 mm, and the mean tendon resection length was 12.8 mm in males and 5.0 mm in females. The mean BTD was 6.35 mm at the arthroscopic suprapectoral tenodesis site and 5.75 mm at the open subpectoral tenodesis site. Males were found to have statistically longer TTL and LO-SBG measurements (111.6 vs 96.5 mm [P = .027] and 37.2 vs 30.0 mm [P = .009], respectively). In the native shoulder, the mean distances from the MTJ to the superior and inferior borders of the pectoralis major tendon were 23.8 and 31.7 mm, respectively. No statistically significant differences were found in the location of the MTJ after simulated arthroscopic or open tenodesis with tenodesis screws as compared with the native shoulder. Mean hole depth in the open subpectoralis tenodesis was 22.4 mm (males) and 18.6 mm (females), with a mean of 20.5 mm for both sexes.
Conclusion:
This study better defines the anatomy of the proximal shoulder in relationship to the long head of the BT. Using our surgical techniques and recommendations, both arthroscopic and open tenodesis procedures adequately restored the native length-tension relationship of the long head of the biceps. Surgical recommendations are as follows: For arthroscopic suprapectoral tenodesis with tenodesis screws, the anatomic landmark of the SBG should be used. The tendon resection length should be approximately 1 cm in males and 5 mm in females when using a 25-mm tunnel. For subpectoral tenodesis, the site of tenodesis should be placed approximately 3 cm above the inferior border of the pectoralis major tendon in the bicipital groove; whipstitching and preserving approximately 2 cm of the biceps tendon above the MTJ is also recommended. The diameter of the screws in either location should be based on patient anatomy. However, this study shows the need for slightly longer screws for the subpectoral tenodesis, as the average hole depth was 20.5 mm. The system used in this study has 7 × 10–mm and 8 × 12–mm screws available. Based on study findings, a screw length of 15 to 18 mm may be needed.
Proximal biceps tendon pathology is a problem commonly encountered by the orthopaedic surgeon. Pathology associated with the need for treatment includes biceps tendonitis/tendinosis, partial tearing or rupture, subluxation, and superior labrum anterior and posterior (SLAP) lesions. 1 This pathology commonly requires surgical intervention, which includes tenotomy or tenodesis. 2,5,8 –10,13 –15,21,24 There has been a long-standing debate as to the most effective procedure for relieving symptoms associated with proximal biceps tendon pathology. Review of the literature would suggest similar subjective outcomes between tenotomy and tenodesis. 10,13 However, tenodesis is generally associated with lower rates of distal migration, weakness with supination, and continued spasm requiring reoperation as well as improved cosmesis. 5,8 –10,13 –15,21,24
Tenodesis of the biceps tendon is a common procedure performed during operative management of shoulder pathology. 3,6,7,14,16,21 –23 Multiple surgical techniques have been described for tenodesis of the biceps tendon; however, little consensus exists as to which technique best reproduces the physiologic length-tension relationship found in the native shoulder. 3 –5,9,15,17,18 There are also few papers that address the anatomy of the biceps tendon and its optimal tenodesis position to reproduce normal anatomy. 17,18
There have been studies that have documented a high rate of revision after arthroscopic biceps tenodesis. One such study is an unpublished review article by Friedman et al 11 that cited a 36% revision rate after arthroscopic biceps tenodesis. A major contributing factor to this high rate is probably attributed to residual pain and tendonitis secondary to the inadequate restoration of the physiologic length-tension relationship of the biceps.
The purpose of this study was to (1) better define the anatomy of the proximal shoulder and long-head of the biceps tendon, (2) compare the length-tension relationship of the biceps tendon in the native shoulder with that after arthroscopic and open tenodesis, and (3) provide surgical recommendations for both procedures based on our findings.
Materials and Methods
Twenty fresh-frozen upper extremity cadavers were dissected for analysis. The extremities were obtained from 20 separate cadavers. No bilateral specimens were used. There were 10 male and 10 female cadavers with an age range of 57 to 61 years. There were 10 right-sided and 10 left-sided extremities examined. Exclusion criteria included any cadaver with evidence of prior surgery or significant shoulder pathology that was encountered during dissection (eg, full-thickness rotator cuff tear, labral derangement, biceps rupture). Both open and arthroscopic tenodesis were performed on the same cadaver, starting with the arthroscopic technique then moving to the open technique.
All dissections were performed by 1 of 3 examiners: a fellowship-trained shoulder and elbow specialist and 2 senior orthopaedic residents. Each specimen contained an anatomic shoulder girdle with a complete clavicle, scapula, and all supporting soft tissue structures, including the entire arm down to the hand (Figure 1). The scapula was used to mount the specimens in a table-vise with the arm hanging free for dissection. A Steinman pin was used to stabilize the glenohumeral joint and maintain the anatomic relationship of the joint throughout dissection with the shoulder in a position of 30° of forward flexion, abduction, and external rotation. The pin was placed from the lateral humeral cortex, through the joint, and into the glenoid.

Each specimen was provided with an intact shoulder girdle with a complete clavicle, scapula, and all supporting soft tissue structures, including the entire upper extremity. The scapula was used to mount the specimens in a table-vise, with the arm hanging free for dissection.
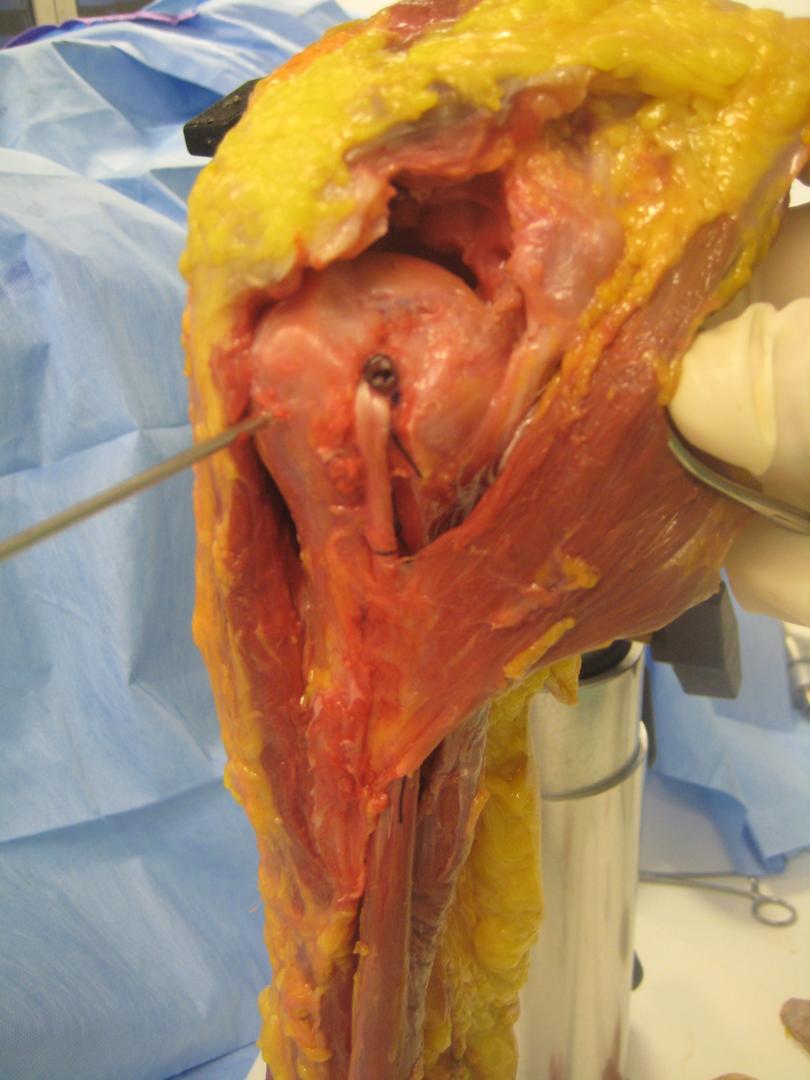
Formal dissection began with the removal of skin and subcutaneous tissue from the anterior half of the shoulder, brachium, and distally to the elbow. A standard deltopectoral approach was then developed. Care was taken to ensure the insertion of the pectoralis major tendon remained intact and uninjured. As we used the insertion of the pectoralis tendon on the humerus as our reference point, we do not feel that the location of the pectoralis tendon was affected by the absence of the thorax in the cadaver specimens. The anterior half of the deltoid was then removed to expose the rotator cuff below. The cuff was then inspected for integrity and pathology (eg, rotator cuff tears, evidence of prior arthroscopic surgery). Next, the biceps tendon was identified and used as a landmark to develop the rotator interval. Portions of the supraspinatus and subscapularis tendon were released at their insertions to allow better visualization of the biceps tendon and its course from the labral origin to the intertubercular groove (Figure 2).

Reflected portions of the supraspinatus and subscapularis tendons that were released at their insertions to allow better visualization of the biceps tendon and its course from the labral origin to the intertubercular groove. The Steinman pin was used to stabilize the glenohumeral joint in 30° of forward flexion, abduction, and external rotation.
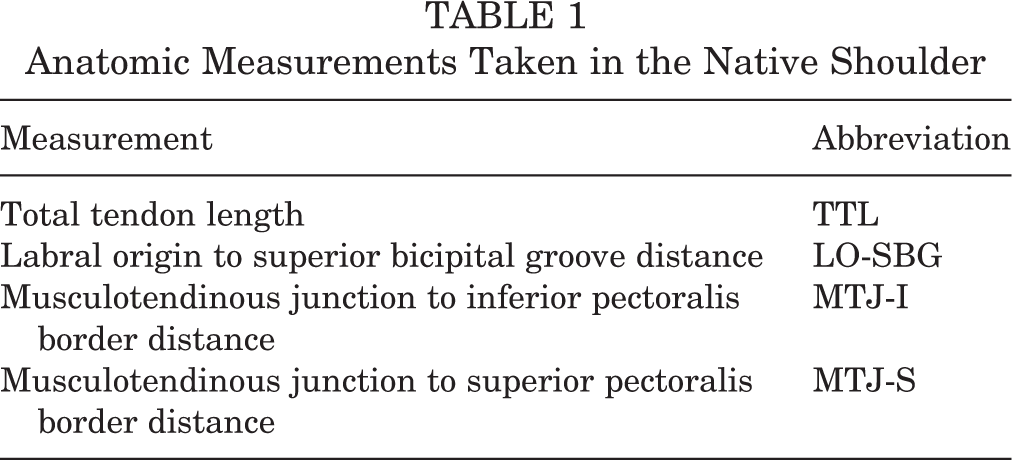
Anatomic measurements gathered in the native shoulder were taken as described (Figure 3). Tagging sutures and pins were placed at specific locations along the biceps tendon to facilitate anatomic length measurements. Table 1 lists the measurements that were gathered in the native shoulder prior to any biceps tenotomy or tenodesis. All length measurements were made using a caliper and checked twice for accuracy. The total biceps tendon length (TTL) was measured from the labral origin to the musculotendinous junction (LO-MTJ). Next, the distance from the labral origin to the superior biceps groove (LO-SBG) was measured. This measurement was taken lateral to the articular margin of the humeral head at the superior aspect of the bicipital groove just before it transitions inferior and distal. Next, the superior and inferior borders of the pectoralis major tendon were identified. Measurements were then gathered from the biceps MTJ to the inferior (MTJ-I) and superior (MTJ-S) borders of the pectoralis tendon. This concluded all measurements that were gathered in the native shoulder.

Location of measurement landmarks in relation to the long head of the biceps. (A) Labral origin (LO); (B) superior bicipital groove (SBG); (C) superior border of the pectoralis tendon (S); (D) musculotendinous junction (MTJ); and (E) inferior border of the pectoralis tendon (I).
Anatomic Measurements Taken in the Native Shoulder
Next, an arthroscopic suprapectoral tenodesis was performed and measurements were recorded. We performed a simulated suprapectoral biceps tenodesis following the same technique and steps that would commonly be used in an arthroscopic setting. The biceps was first tenotomized sharply at its labral origin, which had previously been marked by our tagging suture. Next, the biceps tendon was prepared for tenodesis. This required resecting a specific length of tendon to maintain an appropriate length-tension relationship. We termed this the proximal tendon resection length (TRL-A), and it was calculated in each shoulder by subtracting 25 mm (the amount of tendon length that was placed up in the drill hole) from the LO-SBG measurement, as shown in the following equation:
TRL-A = LO-SGD − 25 mm
The tendon was next whipstitched with a No. 2 Fiberwire (Arthrex, Naples, Florida, USA) for a distance of 25 mm. The proximal tendon diameter (BTD-A) was measured utilizing the Arthrex tendon-sizing guide using a best-fit technique (Figure 4). The superior bicipital groove just lateral to the articular margin was the site for tenodesis. The arthroscopic tenodesis docking sites were all reamed with either 7- or 8-mm drills, depending on the diameter of the proximal tendon. If the tendon diameter was 7 mm or less, a 7-mm reamer was used with a 7 × 23–mm tenodesis screw. If the tendon diameter was >7 mm, then an 8-mm reamer was used with an 8 × 23–mm tenodesis screw. Only 7- and 8-mm screws at lengths of 23 mm are available from the manufacturer system we chose to use. All docking sites were reamed to a depth of 25 mm, as recommended by the device manufacturer for proper seating of the graft.

Use of whipstitch and tendon-sizing guide utilizing a best-fit technique.
The free ends of the stitch were passed through a cannulated arthroscopic screwdriver. We completed the tenodesis using an interference screw of either 7 or 8 mm in diameter, depending on the size of the tendon (Figure 5). With the arthroscopic tenodesis now complete, we remeasured the distance between the MTJ and the inferior and superior borders of the pectoralis major tendon, termed MTJ-I(A) and MTJ-S(A), respectively (we labeled arthroscopic measurements with an “(A)”) (Figure 6). The position of the MTJ after our arthroscopic suprapectoral tenodesis could now be compared to the same measurements in the native shoulder, allowing us to assess the accuracy of our tenodesis at restoring the native length-tension relationship.

The tenodesis is inserted using an interference screw of either 7 or 8 mm in diameter, depending on the size of the tendon.
Completed arthroscopic tenodesis as well as the inferior and superior borders of the pectoralis major tendon.
We then performed a standard open subpectoral tenodesis technique, and measurements were taken and recorded. Our previous arthroscopic tenodesis was taken down, and we prepared for an open subpectoral tenodesis. The drill hole depth in an open tenodesis is variable depending on the diameter of the humeral shaft. To determine the depth required, we used a tenodesis guide pin. The guide pin was placed bicortically at the level of the native MTJ, which had been previously marked. To accurately measure the tenodesis hole length (and not the diameter of the entire humerus), the guide pin was disengaged from the far cortex and placed directly adjacent to the cortical hole along the intramedullary wall. The guide pin was then marked at the near cortical surface, removed, and measured using a caliper. The measurement obtained represents our anticipated hole depth (HD-O) (open tenodesis measurements are denoted by an “O”).
Next, the biceps tendon was prepared for tenodesis, and the diameter was measured in the same manner as described previously for the suprapectoral technique. We identified the MTJ and measured a distance proximally that was equal to our anticipated hole depth. The tendon was marked at this point, and a whipstitch was placed along this same distance using No. 2 Fiberwire. The tendon was then cut just proximal to the whipstitch. In a similar fashion, our proximal tendon resection length for an open procedure (TRL-O) was then calculated from our previous measurements, as shown in the following equation:
TRL-O = TTL − HD-O
We next turned our attention to preparing the tenodesis site. Our guide pin was repositioned bicortically, and we reamed the near cortex with a 7-mm reamer drill. A 7 × 10–mm tenodesis screw was used for all the specimens since none of the tendon diameters measured over 7 mm. An EndoButton (Arthrex) was placed on the tails of our whipstitch and mounted onto the inserting tool (Figure 7). The button was then inserted through the distal cortex and the inserting guide was removed, thereby flipping the button against the far cortex. By alternating tension on the suture tails, we delivered the tendon securely into the docking hole. The tenodesis screw was then placed over the tendon into the hole using the inserter. A free needle was then used to pass one of the Fiberwire suture limbs through the MTJ for additional fixation (Figure 8).

EndoButton placed on the tails of the whipstitch and ready for insertion.

Completed subpectoral biceps tenodesis with interference screw fixation.
With our open subpectoral tenodesis complete, we once again evaluated the new position of the MTJ. We remeasured the distance between the MTJ and the inferior and superior borders of the pectoralis major tendon (MTJ-I[O] and MTJ-S[O], respectively). Finally, the distance between the arthroscopic and open tenodesis sites were measured and recorded.
Statistical Analysis
Descriptive statistics were produced using means, ranges, and standard deviations for continuous variables. Independent variables included sex, tendon lengths, and diameters. Inferential statistics determined statistically significant differences between variables using the independent sample t test. The statistical analyses were performed using SPSS v15.0 (IBM Corp, Armonk, New York, USA).
Results
For all cadavers, the mean biceps total tendon length (TTL) was 104.1 mm, and the mean tendon length from the labral origin to superior biceps groove (LO-SBG) was 33.6 mm. The MTJ was found to be on average 23.8 mm below the superior border of the pectoralis major tendon and 31.7 mm above the inferior border. The mean biceps tendon diameter at the arthroscopic tenodesis site (BTD-A) was 6.4 mm. The tendon was found to be smaller at the open tenodesis site (BTD-O), with a mean diameter of 5.75 mm.
Table 2 lists these same measurements separated for male and female cadavers. Statistically significant differences between sexes were found for TTL and LO-SBG measurements, with P values of .027 and .009, respectively. For both measurements, males were found to have longer tendon lengths. All other measurements taken in the native shoulder failed to show significant differences between the sexes. The location of the MTJ was reanalyzed after performing a simulated arthroscopic suprapectoral tenodesis. For all cadavers, the MTJ was found to be on average 23.6 mm below the superior border of the pectoralis major tendon and 31.8 mm above the inferior border. No significant difference in the location of the MTJ was found after arthroscopic tenodesis as compared with the native anatomy. Similarly, no difference was seen in the location of the MTJ between sexes after arthroscopic tenodesis, as listed in Table 3. Sex-specific analysis did produce 1 significant difference with regard to the proximal tendon cut length that was needed for tenodesis.
Native Anatomic Differences (in Millimeters) Between Male and Female Bicep Tendons a

Differences (in Millimeters) Between Males and Females After Arthroscopic Tenodesis a

a SD, standard deviation. Boldfaced P values indicate statistically significant difference (P < .05).
Males were found to need longer resections than females, as would be expected given the longer LO-SBG distance found in males. These results are also listed in Table 3. A 7-mm diameter interference screw was used on the majority of cadavers. For 3 cadavers with larger tendon diameters, an 8-mm diameter screw was used.
The location of the MTJ was assessed again after performing an open subpectoral tenodesis. For all cadavers, the MTJ was found to be on average 23.1 mm below the superior border of the pectoralis major tendon and 32.4 mm above the inferior border. Again, no significant difference in the location of the MTJ was found after open tenodesis as compared with the native anatomy. Similarly, no difference in the location of the MTJ was seen between sexes after open tenodesis, as listed in Table 4. The mean length of tendon needing to be resected for a subpectoral tenodesis was 83.4 mm. For this measurement, no significant difference was seen between sexes.
Differences (in Millimeters) Between Males and Females After Open Tenodesis a
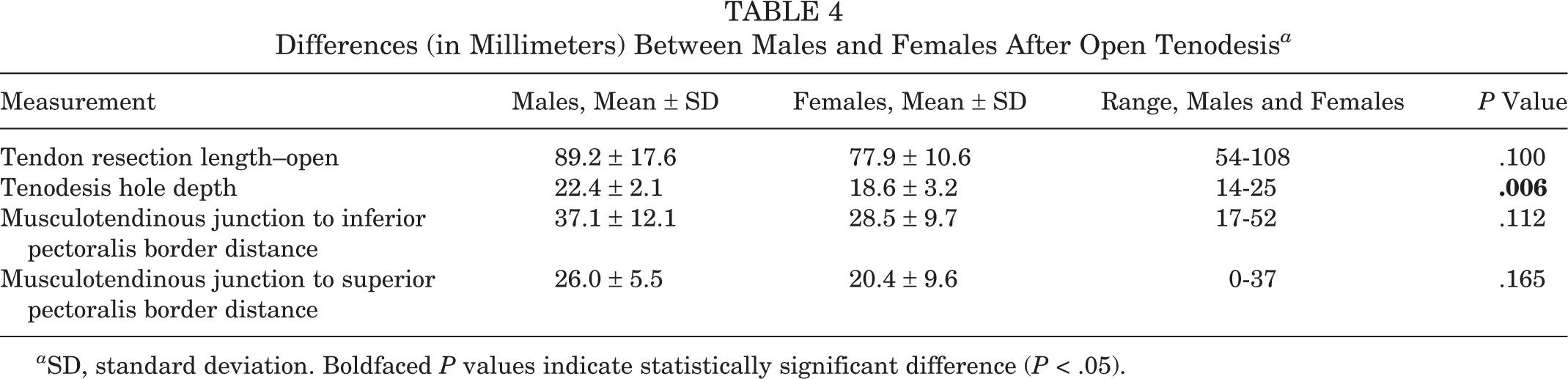
a SD, standard deviation. Boldfaced P values indicate statistically significant difference (P < .05).
All open tenodesis procedures were performed with 7-mm-diameter interference screws given the smaller diameter of the tendon at the MTJ. The average depth of the tenodesis docking hole (HD-O) was found to be 20.5 mm for all cadavers. A difference in drill hole depth did exist between males and females, with males having deeper docking sites. The measurements and analysis from our open tenodesis are listed in Table 4. Finally, the mean distance between the arthroscopic and open tenodesis sites was measured at 68.8 mm for all cadavers. This distance was not significantly different between the sexes. The average distance was 70.1 mm for males and 67.4 mm for females.
Discussion
The proximal long head of the biceps tendon is being addressed surgically at an increasing rate. 5,8 –10,13 –15,17,21,24 Many authors recommend tenodesis over tenotomy for cosmesis or for improved symptom relief 5,8 –10,13 –15,17,21,24 ; however, there are few anatomic studies comparing arthroscopic versus open tenodesis techniques and their effects on restoration of a normal length-tension relationship. There is also a lack of literature describing normal anatomy and its impact on various techniques for tenodesis. The purposes of this study were to (1) better define the normal anatomy of the proximal shoulder in relation to the long head of the biceps tendon, (2) compare the length-tension relationship of the biceps tendon in the native shoulder with that after arthroscopic and open tenodesis, and (3) provide surgical recommendations for both procedures based on our findings.
Recently, there has been debate in the literature as to the effectiveness of arthroscopic versus open techniques, with many authors recommending subpectoral biceps tenodesis. 8,15,17,19,24 Reasons cited have included less need for revision surgery and decreased risk of recurrent pathology. The literature has demonstrated that many authors are reporting persistent anterior shoulder pain with increased need for revision surgery with arthroscopic tenodesis as compared with open subpectoral tenodesis. 25 This has been speculated to be a result of inadequate restoration of the length-tension relationship of the native biceps tendon and/or residual tendonitis that was unrecognized at the original surgery. 5,8 –10,12 –15,17,20,21,24 Denard et al 9 published on the anatomy of the long head of the biceps tendon with some recommendations for performing tenodesis with interference screw fixation. Our study was able to demonstrate the effectiveness of both arthroscopic and open techniques to restore the appropriate length-tension relationship when identifying the appropriate anatomic landmarks.
Jarrett et al 13 found that the musculotendinous junction of the biceps lies 22 mm distal to the upper border of the pectoralis major tendon and 31 mm proximal to the lower border of the pectoralis major tendon, which is similar to our findings. In contrast, a recent study by Denard et al 9 found the musculotendinous junction was approximately 25 mm distal to the upper border of the pectoralis major tendon and approximately 20 mm proximal to the lower border of the pectoralis major tendon, which was different from our findings. This study used specimens amputated above the elbow and did not stabilize the glenohumeral joint, which may have affected the measurements. In our study, we stabilized the glenohumeral joint with a large Steinman pin with the joint in 30° of forward flexion, abduction, and external rotation, simulating normal position during the surgical procedure. We also used specimens that included the entire arm from the scapula to the hand. We believe that this enabled us to obtain the most accurate measurements possible for our study.
Some authors advocate the use of the articular margin of the humeral head as the landmark for the insertion and drill hole for the arthroscopic biceps tenodesis. Denard et al 9 were the most recent authors who used this landmark in their cadaver study. They found that, on average, this landmark was 25 mm from the labral origin. Consequently, they did not have to excise any portion of the proximal biceps tendon during their arthroscopic tenodesis using the same system. We used the SBG as the landmark for the insertion and drill hole for the tendon. This landmark is farther lateral from the articular margin, and we feel using this landmark helps avoid inadvertent damage to the articular cartilage and violation of the rotator cuff and interval during an arthroscopic technique.
We did use an EndoButton Tightrope with our open subpectoral tenodesis, which the senior author (T.J.K.) currently uses in his practice. The senior author’s opinion is that it gives superior strength when combined with a tenodesis screw. It is especially useful with larger and more muscular patients. There has been recent literature published on the neurovascular structures in harm’s way during the subpectoral tenodesis. 8,15,17,19,24 The most common structure at risk is the radial nerve from drilling the humerus posteriorly. If the pin is drilled at our recommendation of 3 cm above the inferior border of the pectoralis major tendon, then the radial nerve should not be at risk. The senior author has been performing this technique for several with no reported nerve-related injuries.
Based on this study, our recommendations are as follows: For the arthroscopic suprapectoral tenodesis using tenodesis screws, we recommend using the anatomic landmark of the SBG as the tenodesis site, which minimizes violation of the rotator cuff and interval. The tendon resection length (TRL-A) should be approximately 1 cm in males and 5 mm in females when using a 25-mm tunnel. This will maintain the normal length-tension relationship. For the subpectoral tenodesis, we recommend the site of tenodesis be placed approximately 3 cm above the inferior border of the pectoralis major tendon in the bicipital groove. We also recommend whipstitching and preserving approximately 2 cm of the biceps tendon above the musculotendinous junction. The hole depth (HD-O) was on average 20.5 mm for males and females. This will help in maintaining the normal length-tension relationship. The diameter of the screws in either location should be based on patient anatomy. However, our study shows the need for slightly longer screws for the subpectoral tenodesis because of the hole depth, which averaged 20.5 mm. Currently, the system used in this study has 7 × 10–mm and 8 × 12–mm screws available. We feel screw length of 15 to 18 mm may be needed based our findings.
As a side note, the senior author does recommend an open subpectoral tenodesis over a suprapectoral arthroscopic tenodesis when there is any sign of proximal biceps tendonitis or tendinosis. The subpectoral technique removes all the tendon proximally, which should alleviate any residual pain and need for revision surgery.
The strengths of this study included the use of 20 cadaveric shoulders (10 male and 10 female), no bilateral specimens, a narrow age range of 57 to 61 years, and no evidence of prior pathology. In addition, the accuracy of our measurements was enhanced by using specimens in which the entire arm was preserved and by securely pinning all glenohumeral joints at 30° of abduction, forward flexion, and external rotation. Based on our study findings, we are able to make recommendations regarding the amount of tendon to be resected and the ideal location for tenodesis (both arthroscopic and subpectoral) to restore the normal length-tension relationship. These guidelines can help surgeons better re-create the normal anatomy of the biceps length-tension relationship and theoretically reduce the incidence of residual pain and revision surgery.
The weaknesses of this study included the following: Our sample did not include specimens with pathology. There may be changes associated with the normal anatomy, which could affect the restoration of the length-tension relationship. Also, there is further need to explore the differences between the normal anatomy of males and females. Finally, there have been no studies that have validated the suspected benefit to restoration of the normal length-tension relationship using our technique.
To our knowledge, there are no studies directly comparing the anatomic length-tension relationship between open subpectoral biceps tenodesis, arthroscopic suprapectoral biceps tenodesis, and its comparison with the native anatomic length tension relationship. In our opinion, open subpectoral biceps tenodesis and arthroscopic biceps tenodesis can effectively restore the normal length-tension relationship when following the guidelines set forth in the article. One can use any commercially available proximal biceps tenodesis system or any technique and utilize the landmarks and measurements presented in this study as a guide to accurately re-establish the native length-tension relationship of the long head of the biceps tendon.
Conclusion
Some controversy exists regarding biceps tenodesis and which surgical technique and location optimally restores the length-tension relationship found in the native shoulder. Using our data and landmarks with the surgical techniques, both arthroscopic and open tenodesis procedures were found to adequately restore this physiologic relationship. This should theoretically reduce residual biceps pain and need for revision surgery. Small anatomic variations do exist between males and females, with males typically having longer tendon lengths throughout the shoulder and deeper drill hole depths during subpectoral tenodesis. These anatomic variations should be considered when performing arthroscopic and open tenodesis of the biceps tendon. Our results and surgical recommendations will help other orthopaedic surgeons when preparing for both open and arthroscopic biceps tenodesis procedures.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: T.J.K. has been a consultant for and receives support from Arthrex, DJO Surgical, Upex, and Mitek DePuy.