
Abstract
Background:
Donor site morbidity after anterior cruciate ligament (ACL) reconstruction with a bone–patellar tendon–bone (BTB) autograft is clinically significant, but evidence with contemporary techniques is lacking.
Purpose:
To (1) evaluate donor site morbidity at a single institution using modern techniques of BTB autograft harvest at 2-year follow-up, (2) develop a 10-question donor site morbidity instrument, and (3) compare this instrument against traditional outcome tools.
Study Design:
Case series; Level of evidence, 4.
Methods:
We analyzed the 2-year follow-up outcomes of 200 consecutive patients who underwent ACL reconstruction with a BTB autograft performed by 2 surgeons at a single institution. The surgical technique utilized modern and consistent BTB autograft harvest, including graft sizing, patellar tendon and peritenon closure, and patellar and tibial donor site bone grafting. There were 187 patients included, with 13 patients undergoing revision ACL reconstruction excluded. An original 10-question scoring instrument evaluating donor site morbidity was administered to each patient (score, 0-100) and compared against each patient’s International Knee Documentation Committee (IKDC) and Lysholm scores.
Results:
Overall, 13.9% of patients were noted to have anterior knee pain with activity at 2-year follow-up. Moreover, 3.7% of patients reported an inability to kneel on hard surfaces but had no problems on soft surfaces; 5.9% of patients reported mild discomfort but were able to kneel on all surfaces. Additionally, 75.4% of patients had a perfect (100/100) donor site morbidity score. The mean donor site morbidity score at 2-year follow-up was 98.3 ± 3.4. There was a very strong correlation between the IKDC and Lysholm scores but only a strong and moderate correlation when the donor site morbidity score was compared with the IKDC and Lysholm scores, respectively.
Conclusion:
Donor site morbidity after ACL reconstruction with a BTB autograft was less frequent than reported in the existing literature. Some patients developed anterior knee pain; therefore, an informed discussion is advised. IKDC and Lysholm scores may not capture donor site symptoms after surgery. The 10-question donor site morbidity instrument may provide a more accurate assessment.
A bone–patellar tendon–bone (BTB) autograft has long been the gold standard for anterior cruciate ligament (ACL) reconstruction in young athletic patients. 24 Donor site morbidity, specifically anterior knee pain, from BTB autograft harvest has been a concern for certain patient populations; however, most data are from historical studies. Surgical techniques often included large incisions, violation of the peritenon, open patellar tendon defects, no bone grafting, and prolonged immobilization. 6,13 Kartus et al 14 described “knee walkers” after this graft choice and noted that 51% of patients were unable to walk on their knees postoperatively with a BTB autograft because of knee pain. In addition to anterior knee pain, studies have reported patellar tendon ruptures, patellar fractures, tendon contracture, numbness, and weakness as potential donor site morbidity after BTB graft harvest. 4,10,15,24 Thus, it is pivotal for current outcome measurement tools to adequately capture each of these potential complications after ACL reconstruction with a BTB autograft, as these factors may not be fully captured using general outcome scores.
The International Knee Documentation Committee (IKDC) subjective form has been recognized as the preferred instrument for capturing symptoms and disability after ACL reconstruction. 9 We believe that this survey, although capturing a patient’s overall symptoms after ACL reconstruction and his/her ability to return to activity, fails to fully quantify donor site morbidity. Furthermore, it remains unclear to what degree donor site morbidity influences the measurements of well-established and frequently used patient outcome tools. If donor site morbidity has been inadequately assessed, these unmeasured outcomes could ultimately influence the decision of autograft source.
The purposes of this study were to (1) evaluate donor site morbidity at a single institution using modern techniques of BTB autograft harvest and closure at 2-year follow-up, (2) develop a novel 10-question donor site morbidity instrument, and (3) compare this instrument with the traditional outcome measures of the IKDC form and Lysholm score. We hypothesized that modern techniques for graft harvesting would have lower donor site morbidity than historically reported in the literature.
Methods
Institutional review board approval was obtained before the initiation of data collection. Through a chart review, we collected 200 consecutive cases of ACL reconstruction with an ipsilateral BTB autograft performed by 2 surgeons (M.J.S., A.J.K.) at a single institution (Mayo Clinic) between the years of 2004 and 2016. Both surgeons preferred to use BTB grafts in young, skeletally mature athletes. Approximately 50% of ACL reconstruction procedures performed during this time period utilized a BTB autograft. A 2-year minimum follow-up was necessary for inclusion in the study; patients who underwent revision surgery were subsequently excluded. Ultimately, 187 patients met the criteria and were included in the data analysis (Table 1).
Patient Demographics (N = 187)

Surgical Technique
The technique utilized by both surgeons consisted of an incision located over the medial one-third of the patellar tendon and medial to the tibial tubercle to avoid direct incisional pressure with activities such as kneeling. Full-thickness skin flaps were created to expose the peritenon. The infrapatellar branch of the saphenous nerve was not routinely identified during dissection. A small central peritenon incision was extended both proximally and distally with the creation of medial and lateral flaps. The peritenon was preserved for closure at the end of the procedure. The tendon width was measured, and patient-specific graft sizing ensured a minimum of 10 mm of intact tendon medially and laterally. The width of the harvested tendon graft generally ranged between 9 and 11 mm. A double-blade knife of appropriate size was used to cut the central tendon in line with the fibers. The tendon was harvested with a 25-mm bone block from the tibia and a 20-mm bone block from the patella. Care was taken when harvesting the patellar bone block with a microsagittal saw to avoid cutting deeper than a 10-mm depth to prevent patellar fractures. All excess bone from the harvested bone blocks after BTB graft preparation was saved for later patellar and tibial bone grafting. The patellar tendon defect was loosely approximated with 2-0 Monocryl sutures (Ethicon), and the remainder of the procedure was then performed. After ACL reconstruction, a cancellous autograft was placed in the patellar and tibial defects and the peritenon closed from proximally to distally with a running 3-0 Monocryl suture, which held the bone graft securely in place. Care was taken to avoid bone graft propagation into the tendon closure.
Postoperatively, patients were allowed weightbearing as tolerated in the setting of isolated ACL reconstruction. No brace was routinely utilized unless the patient requested one. Range of motion was initiated immediately with a focus on terminal extension, followed by return of flexion motion. Controlled return of quadriceps function was initiated early with the avoidance of resisted knee extension in the early postoperative period. Patients progressed through a graduated activity protocol, with return to sport after 8 to 9 months depending on the patient’s progress.
Donor Site Morbidity Instrument
A new 10-question patient-oriented instrument was developed to adequately assess morbidity at the site of BTB harvest (Figure 1). The intent was to measure subjective outcomes, including donor site pain, numbness, function, strength, and physical appearance at the surgical site. All questions had 4 possible answers, each representing increasing symptom severity and patient dissatisfaction. Answer choices were assigned 0 to 10 points depending on the severity or functional restriction. A perfect score of 100 represented no complaints whatsoever. Total scores were subdivided into 4 categories representing overall morbidity after surgery: excellent (≥93.3 points), good (80.0-93.2 points), fair (50.0-79.9 points), and poor (≤49.9 points).
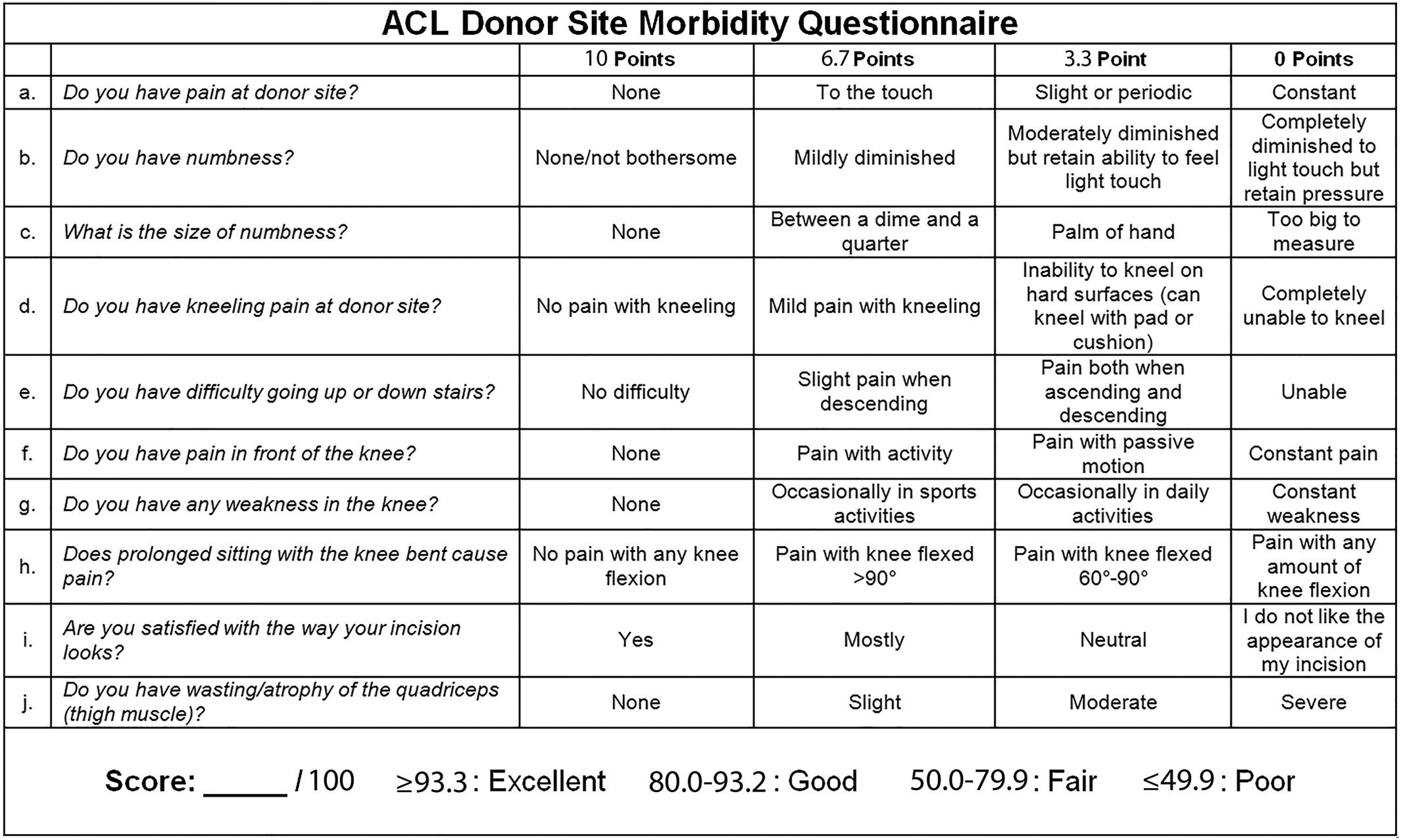
The donor site morbidity questionnaire that was used to measure postoperative outcomes. ACL, anterior cruciate ligament.
Evaluation of Donor Site Morbidity
Operative notes and progress reports were retrospectively reviewed for all study patients. Data were collected at 2-year follow-up, and IKDC, Lysholm, and donor site morbidity scores were then calculated for all patients. The donor site morbidity instrument was administered to determine harvest site morbidity. Other complications, such as patellar tendon ruptures, patellar fractures, and recurrent ACL tears, were documented by a thorough chart review. Finally, donor site morbidity scores were compared against IKDC and Lysholm scores using multivariate correlation analysis with JMP statistical software (SAS Institute).
Statistical Analysis
All patient data were inputted and stored in Excel (2010; Microsoft). Data analysis was performed using both Excel and JMP Pro (v 14.1.0). Demographic information was presented using descriptive statistics, including the mean, percentage, and range. Outcome scores were compared using multivariate correlation analysis with the coefficient (r value) indicating the degree of similarity.
Results
The mean follow-up of the 187 study patients was 2.7 years. Overall, 13.9% of patients at 2-year follow-up were noted to have anterior knee pain with activity. No patient had pain with passive knee range of motion, and no patient reported constant anterior knee pain. Only 3.7% of patients reported an inability to kneel on a hard surface but had no problems on a soft surface; another 5.9% of patients reported mild discomfort but were able to kneel on any surface. No patient reported the inability to kneel. Additionally, 8.5% of patients reported tenderness to palpation at the donor site, with the majority being mild.
Only 2 of 187 patients (1.1%) reported mild to moderate numbness near their incision; both areas of numbness were noted to be 18 to 25 mm in diameter. There were 4 patients (2.1%) who were not completely satisfied with the appearance of their incision. One patient (0.5%) reported subjective weakness in the operative extremity on an almost daily basis, and 2 patients (1.1%) reported slight atrophy of their quadriceps muscle. No patient experienced a patellar tendon rupture or patellar fracture. There were 11 patients (5.9%) who experienced a retear of their reconstructed ACL, with 45.5% of these occurring after 2 years from initial surgery. Radiographs showing incorporation of the bone graft at the donor site at 2 years postoperatively are shown in Figure 2.

Left radiograph shows tibial and patellar donor sites at the time of surgery. Right radiograph shows incorporation of the bone graft at both the patella and tibia at 2 years postoperatively.
Overall, 75.4% of patients had a perfect (100/100) donor site morbidity score. The mean donor site morbidity score at 2-year follow-up was 98.3 (SEM, 0.235 [95% CI, 97.9-98.9]), with scores ranging from 83.3 to 100.0 (Figure 3). There was a very strong correlation between the IKDC and Lysholm scores (r = 0.882). However, when the donor site morbidity score was compared with the IKDC and Lysholm scores, the correlation was only strong (r = 0.667) and moderate (r = 0.597), respectively (Table 2). Additionally, there was notable intrapatient variability between the donor site morbidity, IKDC, and Lysholm scores in select patients, as illustrated in Figure 4. No statistically significant correlation was found among outcome scores on the basis of age, sex, body mass index, or smoking status.
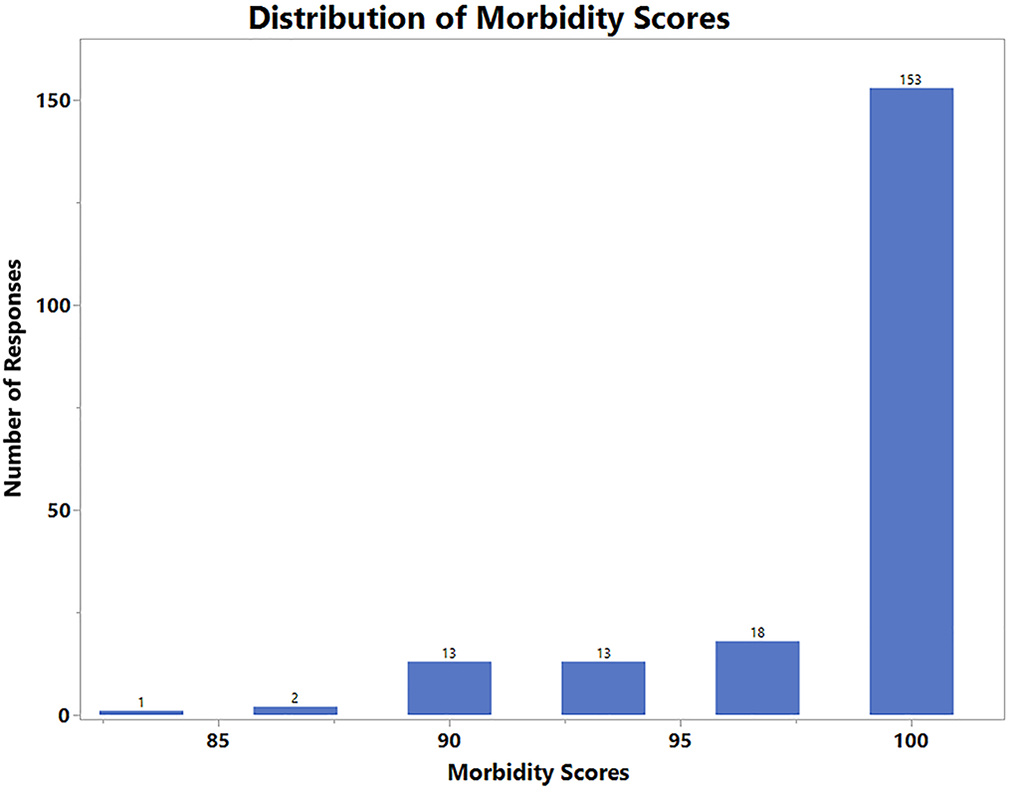
Histogram depicting the distribution of postoperative outcome scores using the donor site morbidity tool.
Multivariate Correlations a

a IKDC, International Knee Documentation Committee.

Intrapatient postoperative outcomes measured via the donor site morbidity (DSM), Lysholm, and International Knee Documentation Committee (IKDC) scores, with each line graphically representing an individual patient. Within each patient, all 3 scores were generated at the same time point.
Discussion
The decision to use a BTB autograft for ACL reconstruction has been a topic of much research and is often dictated by factors such as surgeon preference and patient characteristics. A BTB autograft may offer several advantages over a hamstring tendon (HT) autograft. Several large cohort community- and population-based studies, ranging from 13,647 to 45,998 patients, have shown lower rates of revision after using a BTB graft compared with an HT autograft. 8,18,23 Furthermore, a number of studies have suggested that patellar tendon autografts may have increased stability and reduced side-to-side laxity over HT grafts. 7,16,20,22,30,31
However, several disadvantages of a BTB autograft have been discussed in the literature. Anterior knee pain and donor site pain are well-studied to date, 1,7,20,22,26,28,31 although a more recent study suggests that this effect may diminish over time, with symptoms after a BTB autograft approaching those after an HT autograft at 15 years postoperatively. 30 Studies have shown a wide range of postoperative donor site morbidity with a BTB graft, from as low as 8% to more than 50% of patients with subjective complaints. 14,21,25 This spectrum of patient responses identifies a need for a more consistent outcome scoring tool to quantify complaints related to reconstruction with a BTB graft.
Mastrokalos et al 19 reported localized tenderness of varying severity in 58.3% of contralateral donor knees, suggesting that this pain may be caused by BTB graft harvest rather than the ACL reconstruction procedure. We found a lower incidence of donor site morbidity in our patient population as compared with the current literature, with only 13.9% of patients reporting anterior knee pain with activity and 3.7% reporting the inability to kneel on hard surfaces.
Modern techniques of meticulous surgical dissection and closure of all tissue layers as well as donor site bone grafting may play a significant role in our lower rates of postoperative knee pain. Other studies have reported on the effect of patellar tendon closure on donor site morbidity. Frank et al 6 performed a systematic review of randomized controlled trials, evaluating the effect of closure of the patellar tendon defect after BTB graft harvest for ACL reconstruction. A total of 221 patients in 4 studies were available for analysis (154 male and 67 female). These authors found no statistically significant or clinically relevant difference in outcomes with and without closure of the patellar tendon defect, but the studies were not consistent in their definition of an open or closed tendon defect. Some of the reviewed studies reported closure of the peritenon in all patients, while others left the peritenon open. 6
Another source of morbidity associated with BTB autografts is anterior knee numbness or dysesthesia resulting from transection of the infrapatellar branch of the saphenous nerve. 5,19 Tsuda et al 29 described a transverse incision graft-harvesting technique in an attempt to decrease the rate of infrapatellar nerve branch damage. However, they found that at a follow-up of longer than 2 years, 17% of patients still had decreased sensation in the infrapatellar nerve distribution. 29 Furthermore, transverse incisions may interfere with subsequent knee surgery, which should be taken into consideration when choosing a surgical approach. Tsuda et al also utilized bone grafting of the harvest sites in an attempt to decrease anterior knee pain. Ultimately, 17% of their patients experienced continued anterior knee pain at follow-up, which is less than what has been historically reported in the literature. Interestingly, our vertical graft harvest incision had a lower reported rate of anterior knee pain and numbness than the transverse incision technique.
Postoperative rehabilitation may also play a role in donor site morbidity. Kartus et al 14 confirmed the findings of Shelbourne and Trumper 26 that patients who failed to regain full terminal knee extension had higher rates of knee pain and inability to walk on their knees. Postoperative donor site morbidity is likely multifactorial and may be a combination of patient characteristics such as occupation and sport, surgical graft-harvesting technique, postoperative rehabilitation protocol, and restoration of knee motion.
More than 50 scoring tools exist to quantify the results of ACL reconstruction, 12 but clear outcomes are challenging to measure in the clinical setting. Many of these tools have fallen out of favor because of the growing emphasis on patient-reported measurements. The IKDC (subjective) form, Lysholm score, and Tegner scale are the most frequently used questionnaires in cited ACL trials. 2 The IKDC form has been accepted as the standard instrument for evaluating ACL reconstruction, and much of the donor site morbidity data in the literature stems from this instrument. Hambly and Griva 9 found that the IKDC score better captured patients’ symptoms after ACL reconstruction compared with the Knee injury and Osteoarthritis Outcome Score (KOOS). The IKDC score measures a few functional activities related to donor site morbidity, such as difficulty with kneeling and squatting, but fails to specify if these are related to donor site pain, joint instability, or other factors. In addition, the IKDC form fails to subjectively assess postoperative satisfaction with the incision and skin sensation. 11 The other 2 most used tools, the Tegner scale and Lysholm score, do not address donor site pain or numbness whatsoever. 17,27
We believe that our findings are generalizable to the average patient undergoing primary ACL reconstruction and that our novel 10-question donor site morbidity questionnaire will help standardize specific patient-reported outcomes dedicated to donor site morbidity. This will facilitate future objective comparisons across studies and also between graft types. A dedicated scoring instrument is clearly needed because the current study found a very strong correlation between the IKDC and Lysholm scores but only a strong and moderate correlation between those scores, respectively, and our novel donor site morbidity score. This suggests that this novel instrument captures functional outcomes that are not represented by traditional outcome measures.
Limitations of this study include its retrospective nature, the absence of preoperative scores, and the lack of a control group. Previous studies have examined anterior knee pain after ACL reconstruction using a patellar tendon autograft versus HT autograft and found no significant difference. 3 Therefore, this donor site morbidity questionnaire captures parameters likely specific to BTB graft harvest, such as numbness, and the incision appearance may not be specific to donor site morbidity. Symptoms such as anterior knee pain may be subsequent to the ACL reconstruction procedure itself or confounding factors such as tibial fixation rather than the donor site. We created this scoring system based on surgeon experience, but direct patient input was not utilized in developing the questionnaire, and all questions were given equal weight in the final score. A future follow-up study can examine contralateral BTB graft harvest with modern techniques to evaluate donor site morbidity. Additionally, a future study should include a control group and further assess functional outcomes, such as return to activity and sport. The 2-year follow-up of our patients failed to capture symptoms at 1 year, when many athletes are looking to return to sport. It is possible that patients may have been more symptomatic in the earlier postoperative period but improved over time. Last, there was a notable ceiling effect using this scoring tool, as most patients had high postoperative scores. While this was not unique to our scoring tool, this effect may limit applicability, particularly when the patient is far removed from the reconstruction procedure.
Conclusion
Donor site morbidity after ACL reconstruction with a BTB autograft using modern harvesting techniques, bone grafting, and closure was less frequent than reported in the existing literature. Some patients developed anterior knee pain; therefore, an informed discussion is advised. IKDC and Lysholm scores may not capture donor site symptoms after surgery. The 10-question donor site morbidity instrument may provide a more accurate assessment.
Footnotes
Final revision submitted February 5, 2020; accepted February 19, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.L. has a family member with the following disclosures: consulting fees from Arthrex, Linvatec, Ossur, and Smith & Nephew; research support and speaking fees from Smith & Nephew; and royalties from Arthrex, Ossur, Smith & Nephew, and Thieme. C.L.C. has received hospitality payments from Arthrex and Zimmer Biomet. B.A.L. has received research support from Arthrex, Biomet, Smith & Nephew, and Stryker; educational support from Linvatec; consulting fees from Arthrex; speaking fees from Arthrex and Smith & Nephew; and royalties from Arthrex. M.J.S. has received research support from Arthrex and Stryker and consulting fees, speaking fees, and royalties from Arthrex. A.J.K. has received research support from Aesculap/B. Braun, Ceterix, Exactech, Gemini Medical, and Histogenics; has received consulting fees from Arthrex, JRF Ortho, and Vericel; has received royalties from Arthrex; is a board member for the Musculoskeletal Transplant Foundation; and has stock/stock options in Responsive Arthroscopy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mayo Clinic (study No. PR15-000601-04).