
Abstract
Background:
Several surgical methods have been developed for medial patellofemoral ligament reconstruction (MPFLR). However, the question of which patellar fixation method, suture anchor (SA) or transosseous tunnel (TO) fixation, achieves better overall outcomes remains to be answered.
Hypothesis:
SA patellar fixation will present comparable clinical outcomes and a lower complication rate compared with TO patellar fixation for MPFLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively reviewed the outcomes of 46 patients who underwent MPFLR with either TO fixation (n = 21; mean age, 24.4 ± 6.1 years) or SA fixation (n = 25; mean age, 24.1 ± 12.1 years) for the treatment of recurrent patellar dislocation. Clinical findings (International Knee Documentation Committee [IKDC] subjective score, Lysholm score, and Tegner activity score), radiological findings (congruence angle and patellar tilt angle), and complications (redislocation, patellar fracture, patellofemoral osteoarthritis progression, infection, and stiffness) were compared between the TO and SA groups at the 2-year follow-up visit.
Results:
The mean postoperative IKDC subjective and Lysholm scores did not differ significantly between groups. However, postoperative Tegner activity scores were significantly higher in the TO group than in the SA group (TO, 5.8 ± 1.4; SA, 4.9 ± 1.2; P = .012). Congruence angle did not differ significantly between the groups (TO, −3.2 ± 22.8; SA, −7.6 ± 17.8; P = .464). Patellar tilt angle was lower in the TO group than in the SA group (TO, 10.5 ± 5.4; SA, 13.7 ± 2.8; P = .015). During the follow-up period, the TO group had 1 redislocation and 2 patellar fractures, whereas the SA group had no redislocations or fractures. Patellofemoral osteoarthritis progression was significantly higher in the TO group than in the SA group at the 2-year follow-up visit (TO, 9/21; SA, 2/25; P = .006).
Conclusion:
Both TO and SA patellar fixation methods for MPFLR showed improved clinical outcomes. When compared with TO fixation, SA fixation presented comparable clinical outcomes and a lower complication rate.
Keywords
Medial patellofemoral ligament reconstruction (MPFLR) is commonly used to treat recurrent patellar dislocation. 10,11,13 In the presence of anatomic deformities, MPFLR is combined with realignment osteotomy or trochleoplasty. 15,18 Isolated MPFLR surgery is indicated in patients without anatomic problems such as genu valgum, patella alta, a lateralized tibial tubercle, or severe trochlear dysplasia. 23 According to the literature, appropriate patient selection for isolated MPFLR is linked to good clinical results and low complication rates. 11,12
To date, several surgical methods have been developed for MPFLRs, particularly those for patellar fixation. 1,2,25,26 The techniques for patellar fixation can be classified into 2 groups: suture anchor (SA) fixation and transosseous tunnel (TO) fixation. However, there is a lack of consensus on which of these 2 fixation methods presents a better overall outcome. A biomechanical study demonstrated the advantage of strong fixation at the level of ultimate failure load in patients who underwent TO fixation. 21 However, TO fixation appears to be associated with postoperative complications, such as patellar fracture and patellofemoral osteoarthritis (PFOA). 17
Most studies on clinical outcomes of SA or TO fixation for MPFLR have been case series without any comparison between the techniques. 10 A recent single-arm meta-analysis compared SA fixation and double transpatellar tunnel fixation and found no differences in the redislocation rate between 2 groups. 7 In addition, the authors reported good clinical outcomes associated with SA fixation. 7 Notably, few studies have compared the clinical results of these 2 fixation methods for MPFLR in a single cohort. The question of which patellar fixation method, SA or TO, achieves better clinical outcomes remains to be answered.
The purpose of our study was to compare the clinical and radiological outcomes, as well as the complications, between these 2 patellar fixation methods for MPFLRs. We hypothesized that SA patellar fixation would present comparable clinical outcomes and a lower complication rate compared with TO patellar fixation for MPFLR.
Methods
Patient Selection and Study Design
After receiving study approval from our institutional review board, we retrospectively reviewed the participants’ medical records and radiological data. We included patients who underwent primary isolated MPFLR from October 2007 to January 2016. Until October 2012, we had used TO patellar fixation for all cases of MPFLR. Thereafter, we changed the surgical method to SA patellar fixation. The indication for MPFLR was the same for both surgical methods. Patients with the following contraindications for MPFLR were excluded: tibiofemoral valgus greater than 5°, femoral anteversion greater than 30°, tibial tuberosity–trochlear groove (TT-TG) distance greater than 20 mm, trochlear dysplasia types C and D, and severe patella alta based on radiography and magnetic resonance imaging findings (Insall-Salvati ratio >1.5). 22,24
A total of 62 patients underwent primary MPFLR with the TO or SA method from 2007 to 2016. Patients with concomitant distal femoral varus osteotomy (n = 2), tibial tubercle osteotomy (n = 5), severe PFOA of Kellgren-Lawrence grade 3 or 4 (n = 2), and follow-up of less than 2 years (n = 7) were excluded from the study, and 46 patients were enrolled (Figure 1). Among them, 21 patients (mean age, 24.4 ± 6.1 years) had undergone MPFLR with the TO tunnel method (TO group) and 25 patients (mean age, 24.1 ± 12.1 years) had undergone MPFLR with the SA method (SA group). Preoperative demographic data did not differ significantly between patients in the 2 groups (Table 1).

Flowchart of patient enrollment. DFO, distal femoral osteotomy; K-L, Kellgren-Lawrence; MPFLR, medial patellofemoral ligament reconstruction; PFOA, patellofemoral osteoarthritis; SA, suture anchor; TO, transosseous tunnel; TTO, tibial tuberosity osteotomy.
Preoperative Demographic Data a

a Values are presented as mean ± SD unless otherwise noted. SA, suture anchor; TO, transosseous tunnel; TT-TG, tibial tuberosity–trochlear groove.
Surgical Technique and Rehabilitation
All operations were performed by a single experienced surgeon (K.H.Y.). Diagnostic arthroscopy was performed for all patients. At the time of surgery, osteochondral lesions were refixed or removed depending on the fragment size. Osteochondral fragments of 1 to 2 cm2 were fixed through use of an internal device, ActivaPin (Bioretec), whereas those smaller than 1 cm2 were removed. Chondroplasty or microfracture was performed to repair the osteochondral defects.
For TO patellar fixation, 3-cm longitudinal double incisions were made on the medial and lateral aspects of the patella. Then, 2 transverse or slightly converged patellar tunnels were prepared in the proximal one-third and at the center of the medial edge of the patella by use of 2 guide pins, followed by 4.5-mm reaming with an intervening space of at least 10 mm between tunnels. A femoral guide pin was inserted at the isometric point between the adductor tubercle and medial epicondyle. Fluoroscopy was not used to identify the isometric point. Instead, a dynamic evaluation was performed via the method of Farr and Schepsis. 4 A 6-mm reamer was used to drill a tunnel over the guide pin to a depth of 25 mm (Figure 2A). A tibialis allograft of 4.5 mm in diameter was shuttled into the transverse patellar tunnels to form a loop on the lateral side. A blunt dissection was carried out to create a tunnel in the second layer of the medial soft tissue structures, from the patellar insertion point to the femoral insertion point, carefully leaving the capsule intact. Next, 2 ends of the graft were passed into the soft tissue tunnel and fixed with a 6-mm bioabsorbable interference screw in the femoral tunnel. Femoral fixation was performed at 30° of knee flexion and in neutral rotation, with the lateral patellar edge positioned in line with the lateral trochlear border.

Three-dimensional computed tomography showing the femoral and patellar tunnel position. (A) Transosseous patellar fixation. (B) Suture anchor patellar fixation.
For SA patellar fixation, a 2-cm longitudinal incision was made on the patellar medial margin. After detachment of soft tissue, a medial patellofemoral ligament insertion site was identified at the distal border of the vastus medialis obliquus muscle. A 3.4-mm suture anchor (Healix Transtend BR; DePuy Mitek) was inserted at this point (Figure 2B). A double-stranded tibialis allograft of 6 mm in diameter was prepared (Figure 3). Next, 2 free ends of the graft were fixed to the patella via a suture anchor with 2 pairs of FiberWire. Each FiberWire was used to fix 1 free end of the graft. A femur tunnel was made in the same manner as that used in TO fixation. The methods used in TO fixation were also used for graft passage, femoral tunnel fixation, and graft tension.

A double-stranded tibialis allograft with 2 free ends (4.5 mm in diameter) and a looped end (6 mm in diameter) was used for suture anchor patellar fixation. Two free ends of the graft were fixed to the patella by use of a suture anchor (3.4 mm; Healix Transtend BR). The looped end of the graft was fixed to the femoral tunnel via a 6-mm bioabsorbable interference screw.
The rehabilitation program did not differ regardless of the patellar fixation technique. Tolerable weightbearing ambulation was allowed in a 30° of flexion cast for the first 6 weeks after surgery. After the sixth week, patients were encouraged to perform tolerable range of motion exercises. At 3 months after the surgery, full range of motion was attained in all patients.
Outcome Measurements
Clinical evaluations were performed by use of the International Knee Documentation Committee (IKDC) subjective score, Lysholm score, and Tegner activity score preoperatively as well as at the 2-year follow-up visit by a senior resident who was not involved in this study. A further 2 clinical fellows who were not involved in this study conducted radiological evaluations using congruence and patellar tilt angles preoperatively as well as at the 2-year follow-up visit (Figure 4). Postoperative complications such as redislocation, patellar fracture, PFOA progression, infection, and stiffness were compared between the groups.

Measurement of the congruence angle and patellar tilt angle on a left-knee skyline view (inferior-superior projection of the patella in 45° of flexion). (A) Congruence angle measurement. The highest point of the medial (M) and lateral (L) condyles and the lowest point of the intercondylar sulcus (S) were identified. The zero-reference line (SO, dotted line) was established bisecting the sulcus angle (∠MSL). The lowest point on the articular ridge of the patella (A) was identified, and a line from S to A was drawn. Congruence angle was measured as ∠ASO (α). All values medial to the zero-reference line SO are designated as negative and those lateral as positive. (B) Patellar tilt angle (β) was measured as the angle between a line intersecting the widest bony structure of the patella and a line tangent to the anterior surface of the femoral condyles on a skyline view.
PFOA progression was defined as an arthritic change that is more progressive than that in the preoperative state of the patellofemoral joint on skyline radiographs at the 2-year follow-up. Arthritic change was qualitatively evaluated via the Kellgren-Lawrence classification. 6
Statistical Analyses
All statistical analyses were performed with SPSS Version 20.0 (IBM Corp). Chi-square tests were used to compare qualitative variables (sex, injured side, cartilage injury, and complications), whereas independent t tests were used to compare quantitative variables (age, body mass index, follow-up period, Insall-Salvati ratio, clinical scores, and radiological angle). For preoperative and postoperative comparisons of the clinical scores and radiological angles, a paired-samples t test was used. A P value less than .05 was considered statistically significant.
Intra- and interobserver reliabilities were determined by calculating the intraclass correlation coefficient (ICC) for radiological measurements, including Insall-Salvati ratio, TT-TG distance, congruence angle, and patellar tilt angle. An ICC of less than 0.40 was considered poor, whereas ICCs of 0.40-0.59, 0.60-0.74, and 0.75-1.00 were considered fair, good, and excellent, respectively. 5
Results
Clinical Outcomes
Postoperatively, all clinical scores improved significantly in both groups. At the 2-year follow-up visit, the IKDC subjective and Lysholm scores were not significantly different between the groups. However, the Tegner activity score was significantly higher in the TO group than in the SA group (TO, 5.8 ± 1.4; SA, 4.9 ± 1.2; P = .012) (Table 2).
Comparison of Pre- and Postoperative Clinical Scores a
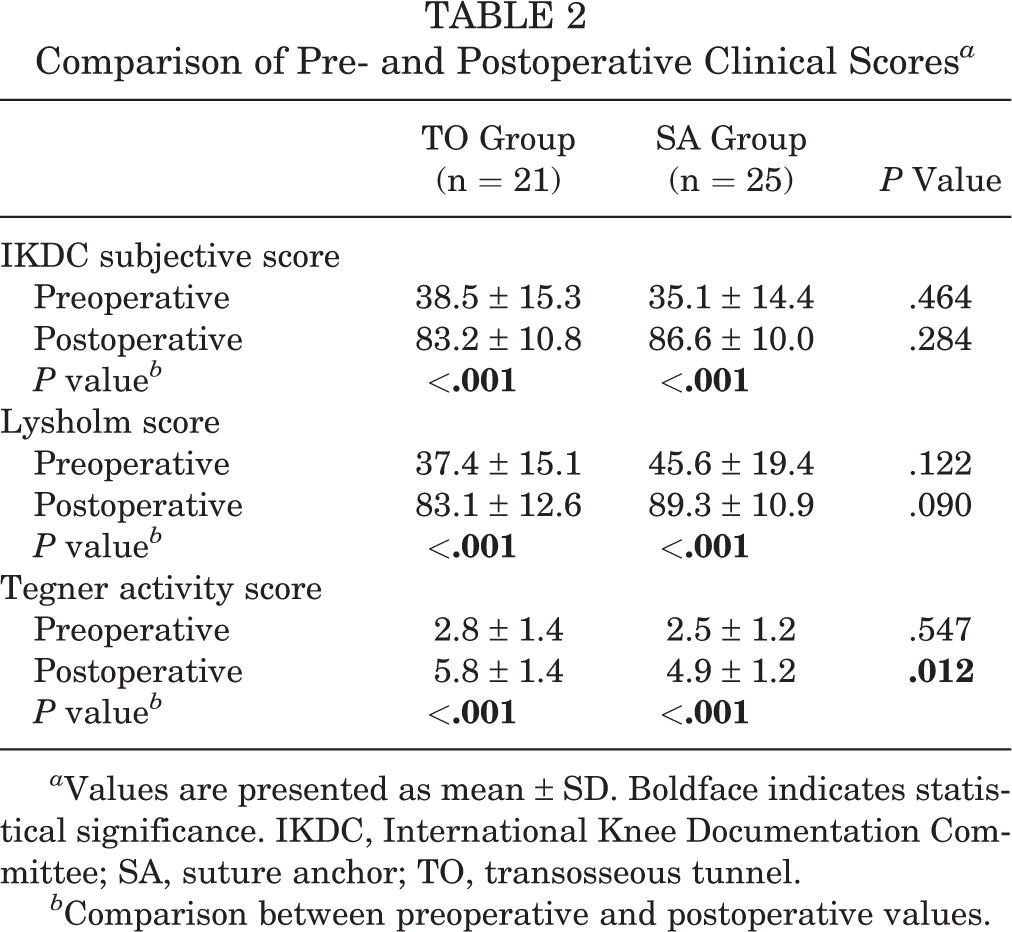
a Values are presented as mean ± SD. Boldface indicates statistical significance. IKDC, International Knee Documentation Committee; SA, suture anchor; TO, transosseous tunnel.
b Comparison between preoperative and postoperative values.
Radiological Outcomes
ICCs for all measurements were greater than 0.8. Preoperative congruence and patellar tilt angle were not significantly different between the 2 groups. In both groups, congruence angles did not show significant improvement at the 2-year follow-up visit. In contrast, the TO group presented significant improvement in the patellar tilt angle at the 2-year follow-up visit (P = .001), but the SA group did not. Moreover, the postoperative patellar tilt angle was lower in the TO group than in the SA group (TO, 10.5 ± 5.4; SA, 13.7 ± 2.8; P = .015) at the 2-year follow-up visit (Table 3).
Comparison of Pre- and Postoperative Radiological Outcomes a

a Values are presented in degrees as mean ± SD. Boldface indicates statistical significance. SA, suture anchor; TO, transosseous tunnel.
b Comparison between preoperative and postoperative values.
Complications
The TO group had significantly more complications than the SA group (TO group, 12/21; SA group, 2/25; P < .001) (Table 4). Redislocation occurred in 1 patient and patellar fracture occurred in 2 patients in the TO group during the 2-year follow-up. Further, 2 patients with patellar fracture underwent open reduction and internal fixation (Figure 5). At the 2-year follow-up visit, PFOA progression was significantly higher in the TO group than in the SA group (TO, 9/21; SA, 2/25; P = .006) (Tables 4 and 5). No other complications, such as infection or stiffness, were observed in either group.
Comparison of Postoperative Complications a
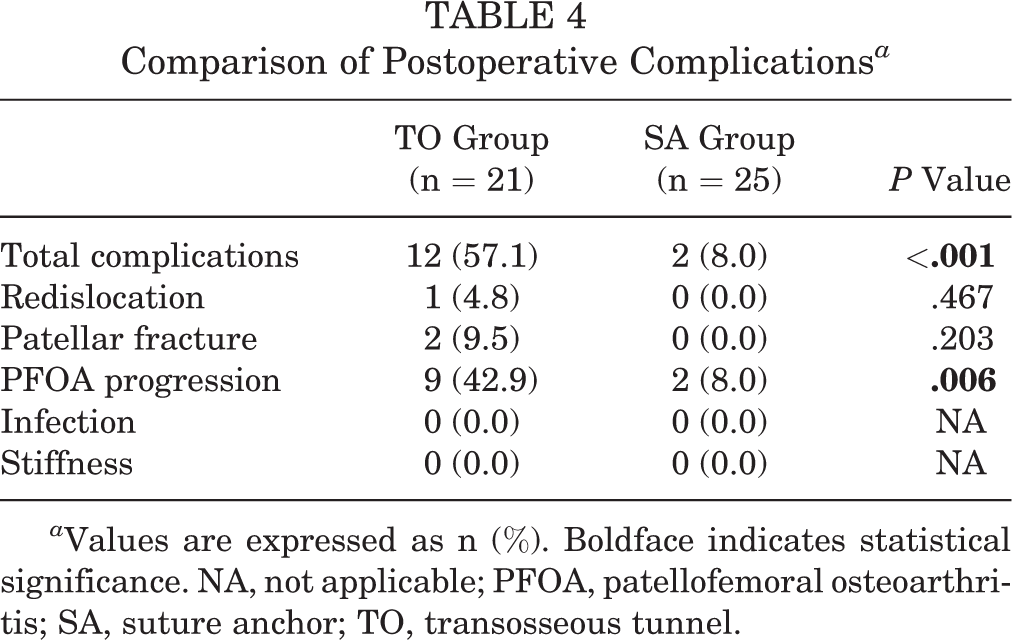
a Values are expressed as n (%). Boldface indicates statistical significance. NA, not applicable; PFOA, patellofemoral osteoarthritis; SA, suture anchor; TO, transosseous tunnel.

A case of patellar fracture following medial patellofemoral ligament reconstruction using transosseous patellar fixation. (A) Postoperative lateral radiograph. (B) Lateral radiograph showing patellar fracture at the level of the upper patellar tunnel at 1 year postoperatively. (C) Lateral radiograph obtained after open reduction and internal fixation. Note: The staples are not related to the medial patellofemoral ligament reconstruction.
Patellofemoral Osteoarthritis According to Kellgren-Lawrence Classification at 2-Year Follow-up a

a Values are expressed as n (%). Boldface indicates statistical significance. SA, suture anchor; TO, transosseous tunnel.
b Comparison between preoperative and postoperative values.
Discussion
The most important finding of this study was that the TO group had a greater number of complications than the SA group at the 2-year follow-up visit, although SA patellar fixation for MPFLR resulted in comparable clinical outcomes. The two fixation methods presented disparate complication rates, especially concerning patellar fracture and PFOA progression. Of 21 patients in the TO group, 2 (9.5%) had postoperative patellar fracture and 9 (42.9%) had PFOA progression during the 2-year follow-up. In addition, the TO group revealed greater radiological improvement than the SA group, but no significant intergroup differences were observed in the redislocation rates.
Several studies have compared the clinical outcomes between TO and SA patellar fixation methods in MPFLR; however, the results are conflicting. For example, Ji et al 8 demonstrated that the mean Kujala and Lysholm scores in the TO group were significantly higher than those in the SA group. In contrast, a 2019 meta-analysis showed that the mean improvement in the Kujala score after MPFLR was higher in patients who underwent SA fixation than in those who underwent TO fixation. 7 However, the mean improvement in the Lysholm score did not differ significantly between the 2 fixation techniques. 7 Although the Kujala score was not used in the present study, significant intergroup differences were not observed in the IKDC subjective or Lysholm scores.
The TO group showed better radiological outcomes than the SA group in terms of the postoperative patellar tilt angle at the 2-year follow-up visit. Recent clinical studies have also reported a greater improvement in the patellar tilt angle and lateral patellar angle in the TO group than in the SA group, 8 which can be explained by the results from previous biomechanical studies that compared the peak force versus fixation failure between patellar fixation techniques. 9,14 These biomechanical studies reported that the TO fixation method had greater biomechanical strength than the SA fixation method. 9,14 As expected from these previous findings, the TO group in the current study was found to have a more rigid fixation as well as greater radiological improvement than the SA group.
Shah et al 23 reported complications such as patellar fracture after MPFLR surgery. In our study, 2 cases of patellar fracture occurred in the TO group, but none occurred in the SA group. This result suggests that two 4.5-mm transverse patellar tunnels can pose a risk for patellar fracture. Using magnetic resonance imaging, Yoo et al 27 confirmed that the mean longitudinal length of the articular surface was 32.9 mm (range, 27.2-40.6) whereas the mean thickness was 22.3 mm (range, 17.9-28.4) in a Korean population. Because the patella is small, the risk of patellar fracture is high with TO fixation; therefore, SA patellar fixation can be used as a safe alternative method to prevent patellar fractures, especially in patients with a small patella.
The TO group had a more substantial PFOA progression at the 2-year follow-up visit than the SA group. As mentioned earlier, TO patellar fixation has greater biomechanical strength than SA patellar fixation. 9,14 However, previous studies have reported that rigid fixation using the TO method for MPFLR increased the patellofemoral pressure 3 to 5 times in flexion angles ranging from 60° to 110°, which might cause PFOA progression in patients. 20 Another possible reason for PFOA progression in the TO group is direct or thermal injury to the subchondral bone during drilling and reaming of the patellar tunnel, as subchondral bone injury affects cartilage degeneration and causes arthritic changes. 3,19 Finally, PFOA progression in the TO group might be affected by the malposition of the patellar tunnel. We tried to make 2 patellar tunnels in the proximal one-third and at the center of the medial edge of the patella. However, in some patients, the distal tunnel was formed below the center of the patella (Figure 5). This might increase the patellofemoral pressure and contribute to PFOA progression.
This study has several limitations. First, it was a retrospective and nonrandomized study; therefore, it may have been influenced by selection bias. Second, the number of cases included in this study was small, although this study showed a significant difference in complication rates between the groups. Additional studies with larger sample sizes are needed to make more precise conclusions. Third, 2 surgical methods were performed during 2 different periods. Clinical outcomes and complications may have been influenced by surgical proficiency in femoral tunnel location and/or graft tension. However, the bias would be minimized because all operations were performed by a single experienced surgeon. Fourth, femoral tunnel position was not evaluated in this study. Femoral tunnel malposition in MPFLR is associated with poor clinical outcomes. However, only the patellar fixation technique was used as an independent parameter in this study. Fifth, we used 3 scores (IKDC subjective, Lysholm, and Tegner activity scores) to evaluate patient-reported clinical outcomes. Although several studies have used these scores to evaluate the clinical outcomes after MPFLR, 16 these scores were not based on questionnaires designed for patellofemoral disorders. The scores we assessed in this study could evaluate knee function and patient activity. However, they might not be as efficient as specific evaluation tools such as the Kujala score for assessing patellofemoral symptoms. Finally, a 2-year follow-up period might be not sufficient for evaluating some complications such as PFOA progression. Therefore, mid- to long-term follow-up studies are needed in the future.
Despite these limitations, this study was the first to compare clinical outcomes and complications of 2 patellar fixation methods for MPFLR in a single cohort. In this study, SA fixation for MPFLR obtained comparable results in clinical scores as TO fixation at the 2-year follow-up visit. In addition, SA fixation for MPFLR reduced the incidence of complications such as patellar fracture and PFOA progression. The findings of this study may be helpful for orthopaedic surgeons when treating patients with recurrent patellar dislocation.
Footnotes
Final revision submitted January 8, 2020; accepted January 29, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital (file No. KHUH 2018-06-067).