
Abstract
Background:
Medial patellofemoral ligament (MPFL) reconstruction is a commonly employed surgical approach for recurrent patellar dislocation. However, the impact of elevated body mass index (BMI) on postoperative complication rates remains controversial.
Purpose:
To compare the clinical, radiographic, and functional outcomes of patients with normal BMI (18.5-24.9 kg/m2) and those with elevated BMI (≥25 kg/m2) who underwent MPFL reconstruction for recurrent acquired lateral traumatic patellar dislocation.
Study Design:
Cohort Study; Level of evidence, 3.
Methods:
A total of 70 patients who underwent MPFL reconstruction for recurrent patellar dislocation were included in this study. Patients with recurrent patellar dislocation were categorized into 2 groups based on their BMI: the normal BMI group and the elevated BMI group. Functional scores (Lysholm, International Knee Documentation Committee [IKDC], Tegner, and Kujala scores) and radiological measurements (patellar tilt angle, patellofemoral trochlear congruence, lateral patellofemoral angle, and lateral patellar displacement) were evaluated both preoperatively and at the last follow-up. The occurrence of postoperative complications at the last follow-up was also recorded. Differences in functional scores and radiological parameters before and after surgery were analyzed with paired-samples t tests or Wilcoxon signed-rank tests. Comparisons between groups were conducted using independent-samples t tests or the Kolmogorov-Smirnov test.
Results:
In the normal BMI group, there were 13 male patients and 27 female patients, with a mean follow-up duration of 26.15 ± 13.16 months. The mean age in this group was 21.93 ± 7.94 years. The elevated BMI group consisted of 12 male patients and 18 female patients, with a mean follow-up duration of 27.50 ± 15.79 months and a mean age of 23.30 ± 8.43 years. At the final follow-up, the incidence of surgical failure (patellar redislocation or subluxation and necessitating secondary surgery) was significantly higher in the elevated BMI group (6 out of 30 patients; 20.0%) compared with the normal BMI group (1 out of 40 patients; 2.5%) (P < .05). Both groups demonstrated significant improvement in postoperative Lysholm, IKDC, Tegner, and Kujala scores compared with the preoperative period (P < .05). Notably, the normal BMI group had significantly higher preoperative Lysholm and Tegner scores compared with the elevated BMI group (P < .05). Furthermore, the elevated BMI group exhibited less improvement in Tegner and Kujala scores compared with the normal BMI group (P < .05). Postoperative radiological parameters in both groups returned to the normal range (P < .05). There were no statistically significant differences between the 2 groups in terms of radiological parameters and their corresponding differences.
Conclusion:
Our study demonstrated statistically significant increases in postoperative clinical scores for both groups, although the intergroup differences varied. Specifically, patients with elevated BMI demonstrated poorer preoperative Lysholm and Tegner scores. The postoperative improvement in radiological parameters was equally good between the 2 groups.
Keywords
The medial patellofemoral ligament (MPFL) is the primary stabilizer restraining lateral displacement of the patella and is injured in up to 94% of traumatic lateral patellar dislocations. 21 As a result, MPFL reconstruction continues to be the most preferred approach despite the emergence of various surgical techniques for managing patellar dislocations in recent years.9,26 In addition, MPFL reconstruction can be supplemented by several bony procedures that can address anatomic abnormalities. For example, trochleoplasty handles severe trochlear dysplasia, 19 and tibial tuberosity transfer handles excessive tibial tuberosity to trochlear groove distance. 1
Patients with elevated body mass index (BMI) will be exposed to a greater load on injured cartilage, leading to worse pain after acute patellar dislocation. 2 Moreover, Milinkovic et al 18 have proven that elevated BMI predicts poor disease-specific quality of life after lateral patellar instability. One study reported that elevated BMI was significantly associated with poor clinical outcomes after MPFL reconstruction alone or with bony surgery. 30 However, Sherman et al 25 demonstrated significant improvement in patient-reported outcomes and a lower complication rate in obese patients undergoing MPFL reconstruction. These studies present conflicting findings on the topic.
This study aimed to investigate the effect of BMI on clinical outcomes after MPFL reconstruction by comparing functional outcomes, complication rates, and radiographic outcomes in patients with normal BMI (18.5-24.9 kg/m2) and elevated BMI (
Methods
This study was designed as a retrospective analysis of patients who underwent MPFL reconstruction between July 2017 and March 2022. It was approved by the local ethics committee (Lanzhou University Second Hospital, No. 2022A-224). The patient’s height and weight were measured at the initial visit using stadiometers and calibrated scales. BMI was calculated by a standard equation (BMI = weight/height2, kg/m2). We classified the included patients as normal BMI group (18.5-24.9 kg/m2) and elevated BMI group (
Patients were included if they met 1 of the following criteria: (1) exhibited patellar lateral overhang as demonstrated on computed tomography (CT); (2) underwent MPFL reconstruction for recurrent lateral patellar dislocation of traumatic onset (
Surgical Intervention and Postoperative Protocol
Under subarachnoid anesthesia, the patient was placed in the supine position with lateral support. A tourniquet was used to reduce intraoperative bleeding during the operation. Initially, under arthroscopy, the intra-articular damage was assessed, followed by the removal of intra-articular hematomas and fracture fragments. Subsequently, the semitendinosus was retrieved for MPFL reconstruction.
Patellar Fixation
A longitudinal incision of approximately 4 cm was made along the medial margin of the patella to expose the patella and the proximal half of its bone surface. The double semicurve tunnel locator was utilized to guide the insertion of a 2-mm Kirschner wire at the junction of the proximal one-third of the medial edge of the patella, ensuring the protection of the patellar cartilage. Another Kirschner wire was inserted in the same manner at the midpoint of the medial edge of the patella. Subsequently, the drill was used to create tunnels along the 2 Kirschner wires, with the drilling width matching that of the graft. The distal ends of the 2 tunnels extended to half the diameter of the patella. The third and fourth tunnels were created in a similar manner, running in a front-to-back direction and connecting vertically to the first and second tunnels (Figure 1). The semitendinosus tendon was then passed through the 2 tunnels sequentially, starting from the inner edge of the patella, and the 2 free ends were sutured together laterally, forming a double-bundle tendon autograft.
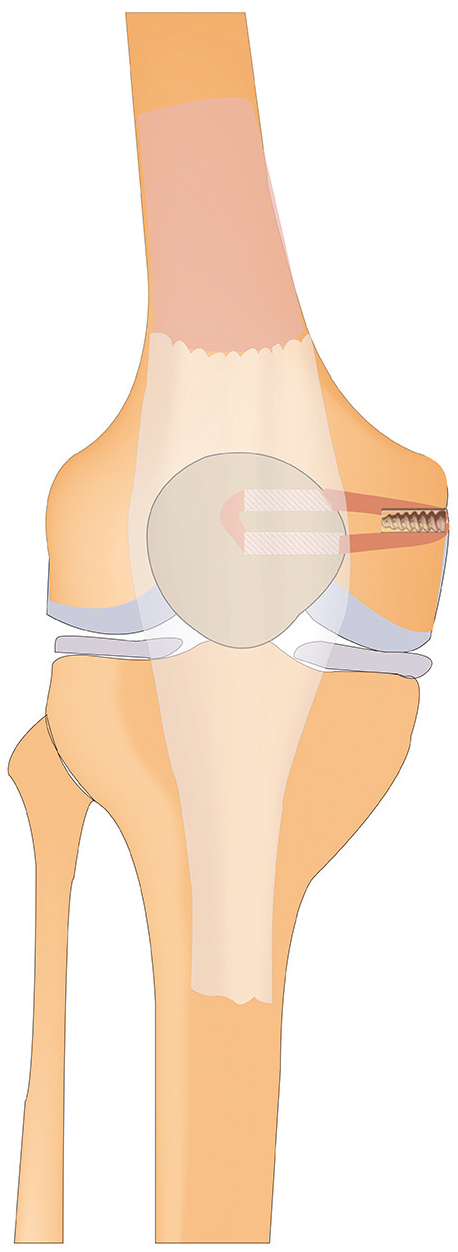
The drawing depicts the creation of the double semicurve tunnel by drilling from the proximal one-third and midpoint of the medial edge of the patella.
Femoral Fixation
A 2 cm–long longitudinal incision was made on the medial epicondyle of the femur to expose the femoral attachment site of the MPFL, located between the adductor tubercle and the medial epicondyle. With the aid of a fluoroscopic C-arm, a Kirschner wire with a diameter of 2 mm was inserted from the crest of the adductor tubercle and the medial epicondyle to the outside of the femur. The femoral fixation point was situated approximately 1.3 mm anterior to the posterior cortical line of the femur and 2.5 mm distal to the starting point of the femoral medial condyle, known as the Schöttle point. 23 This positioning was crucial for maintaining the isometric nature of the reconstructed ligament, ensuring optimal isometry of the femoral lateral ligament. A 7 mm–diameter drill was used to create a tunnel along the Kirschner wire, and the distal end of drill reached the lateral femoral cortex. The suture end of the graft was passed through the hole of the femoral tunnel to assist the graft in passing through the tunnel. The appropriate tension was applied to the graft at 30° of knee flexion, and femoral fixation was performed after ensuring that the patella smoothly entered the femoral trochlea. After reconfirmation of normal patellar tracking during knee flexion, it was fixed with a bioabsorbable interference screw (Arthrex) (Figure 1). Finally, the patellar tracking was reconfirmed under knee arthroscopy.
Rehabilitation Protocol
All patients followed similar rehabilitation training protocols. The affected limb was treated with ice compress and pressure bandage immediately after the operation. An adjustable knee joint brace was initiated at this time to keep the affected limb in full extension, and nonsteroidal anti-inflammatory drugs were taken to relieve pain. On the first day after recovering from anesthesia, the affected limb underwent quadriceps femoris contraction training, and the patella was gently pushed inward at regular intervals as needed to prevent soft tissue adhesion. For 2 weeks, the patient was allowed to stand with the use of a crutch to keep the braced knee straight.. Achievement of 90° of knee flexion by 4 weeks postoperatively and full range of motion by 8 weeks postoperatively were required to ensure optimal recovery and functional outcomes. `Full range of motion’ refers to the ability to flex and extend the knee through its complete natural range without restriction. All patients wore the knee brace to the 3-month postoperative time point for ongoing protection while the affected limb regained normal motion. Sports activities were gradually carried out at 6 months postoperatively.
Clinical and Radiographic Evaluation
Demographic data (age, sex, side, and follow-up time), medical history (osteochondral fractures, time to surgery, and length of stay), subjective functional outcomes (Lysholm, International Knee Documentation Committee [IKDC], Tegner, and Kujala scores), and radiographic parameters were collected preoperatively. Patellar tilt angle (≥20° was considered abnormal), 6 patellofemoral trochlear congruence (>16° was found to be abnormal), 17 lateral patellofemoral angle (inward opening or parallel to the 2 lines was considered abnormal), 13 and lateral patellar displacement (more than half the width of the patella was considered abnormal) 11 were measured in the transverse plane on CT. On the postoperative CT, the measurement of patellar tilt angle, patellofemoral trochlear congruence, lateral patellofemoral angle, and lateral patellar displacement was repeated. Radiological parameters were measured by 3 authors (Q.W., J.Z. and Z.W.), and the final analysis was based on the mean values. In addition, at the last follow-up, postoperative objective functional outcomes were re-evaluated and the occurrence of complications (eg, surgical failure, anterior knee pain, wound infection, and wound scar) was recorded. Surgical failure was defined as patellar redislocation or subluxation and necessitated secondary patellar stabilization surgery. 16
Statistical Analysis
All statistical analyses were performed using SPSS Version 26.0 (IBM). The Shapiro-Wilk test was used to check the normal distribution of the data before performing the descriptive statistical analysis. Continuous variables were described as means and standard deviations when their distributions conformed with normal distributions and as medians with interquartile ranges otherwise. The dichotomous variables were described as frequencies with percentages. Preoperative and postoperative differences in functional scores and radiological parameters were tested using paired-samples t tests or Wilcoxon signed-rank tests. Functional scores and radiological parameters were compared between groups using 2 independent-samples t tests or the Kolmogorov-Smirnov test. Chi-square test or Fisher exact test was used for intergroup comparisons of dichotomous variables. Statistical significance was set at P < .05 for all analyses.
Results
A total of 70 patients (70 knees) were included for analysis. The demographic results, medical history, and radiological parameters were summarized and are presented in Table 1. The overall mean follow-up time for patients was 26.72 ± 14.24 months. The percentage and mean age of female patients were 64.3% and 22.51 ± 8.12 years, respectively. There were 40 participants in the normal BMI group and 30 in the elevated BMI group. Patients with concomitant osteochondral fractures accounted for 32.5% in the normal BMI group and 26.7% in the elevated BMI group, with no statistically significant difference between the 2 groups. In terms of the mechanisms of injury, we categorized them as falling from a height, motor vehicle crash, sprain during exercise, and other. Other included instances such as slipping, standing up after prolonged sitting, and walking without a clear precipitating cause. Chondroplasty was employed as a therapeutic approach for addressing osteochondral fractures, with the removal of fragments deemed necessary in instances where osteochondral fracture fragments had become dislodged, forming loose bodies.
Demographic Results, Medical History, and Surgical Information

Data presented as mean ± SD, unless otherwise indicated. BMI, body mass index; IQR, interquartile range.
Functional Scores
The results of the clinical scores (Lysholm, IKDC, Tegner, and Kujala scores) for normal BMI and elevated BMI groups are presented in Table 2. The scores in both groups exhibited a statistically significant increase at the last follow-up compared with preoperatively (P < .05). Notably, for preoperative functional scores, the normal BMI group had significantly greater Lysholm scores and Tegner scores compared with the elevated BMI group (P < .05). Additionally, the normal BMI group did statistically just as well in terms of improvement in Lysholm and IKDC scores as the elevated BMI group, while showing significantly greater improvement in Tegner and Kujala scores (P < .05).
Comparison of the Functional Scores a

Data presented as mean ± SD or median (interquartile range). BMI, body mass index; IKDC, International Knee Documentation Committee.
Radiographic Parameters
The results of the radiological parameters (patellar tilt angle, patellofemoral trochlear congruence, lateral patellofemoral angle, and lateral patellar displacement) in both groups are presented in Table 3. At the final follow-up, the patellar tilt angle, patellofemoral trochlear congruence, lateral patellofemoral angle, and lateral patellar displacement returned to normal values in both groups, with a statistically significant improvement compared with the preoperative period (P < .05). Additionally, there were no statistically significant differences between the 2 groups in radiological parameters.
Comparison of Radiographic Parameters a

Data presented as mean ± SD. BMI, body mass index.
Complications
During the final follow-up, 4 patients in the normal BMI group and 9 patients in the elevated BMI group experienced postoperative complications. A significant difference was observed between the 2 groups (P < .05). Notably, it was observed that 1 patient from the normal BMI group experienced failure, whereas 6 patients from the elevated BMI group experienced failure, with a statistically significant difference between the 2 groups (P < .05). Importantly, patients with these surgical failures all experienced recurrent subluxations; however, none of these patients exhibited marked dislocation of the patella. Two patients in the normal BMI group and 2 patients in the elevated BMI group reported anterior knee pain. However, there was no statistically significant difference between the 2 groups. No patients in either group experienced redislocation. In terms of other complications, 1 case of surgical wound infection was observed in the normal BMI group, while 1 patient in the elevated BMI group exhibited a surgical wound scar. However, there was no statistically significant difference between the 2 groups (Table 4).
Comparison of Complications a

BMI, body mass index.
Dashes indicate that Fisher’s exact test was used, and the χ2 statistic is not available.
Discussion
The most important findings of this study reveal that the normal BMI group exhibited a significantly greater improvement in Tegner and Kujala scores when compared with the elevated BMI group (P < .05), while there was no significant difference in improvement in Lysholm and IKDC scores. The normal BMI group demonstrated significantly higher preoperative Lysholm and Tegner scores compared with the elevated BMI group (P < .05). Additionally, the incidence of postoperative complication was significantly higher in the elevated BMI group as compared with the normal BMI group (P < .05). However, there were no statistically significant differences observed in radiological outcomes between the 2 groups. Therefore, our hypothesis was valid.
In this study, we found that the elevated BMI group showed significantly less improvement in Tegner and Kujala scores compared with the normal BMI group, while there was no significant difference in improvement in Lysholm and IKDC scores. This finding aligns with a previous study by Žlak et al, 30 who investigated potential predictors of patient-reported outcome measures in a retrospective analysis of 116 patients. They found a negative association between BMI and patient-reported outcome measures. Another prospective study examined the impact of elevated BMI on the quality of life in patients with patellar instability using backward stepwise multiple regression analysis. 18 The results indicated a significant influence of elevated BMI on patient-reported outcome measures. Similarly, Sherman et al 25 used a BMI cutoff of 30 kg/m2 to compare the clinical outcomes of patients undergoing MPFL reconstruction between groups that were obese and nonobese. They observed that patients who were nonobese had greater improvements in the Knee injury and Osteoarthritis Outcome Score Quality of Life subgroup and Tegner scores compared with patients who were obese. Hart et al 7 demonstrated a significant correlation between BMI and the severity of chronic knee pain. Patients with patellar dislocation often experience intense patellofemoral pain, which contributes to a fear of redislocation. Consequently, an elevated BMI can further limit their ability to engage in daily activities. 27
The current study indicated that preoperative Lysholm and Tegner scores were significantly lower in the elevated BMI group compared with the normal BMI group. This finding aligns with a retrospective study conducted by Zaffagnini et al, 29 where a significant association was observed between elevated BMI and inferior preoperative scores. This observation can be attributed to the increased strain placed on the articular cartilage of the medial and lateral compartments due to elevated BMI, resulting in more severe symptoms after patellar dislocation.4,28
Our study demonstrated a significant association between elevated BMI and an increased incidence of surgical failure, surpassing that observed in the normal BMI group. Previous studies have indicated that the reasons for MPFL reconstruction failure include patella alta, 22 trochlear dysplasia,8,12 and J-sign. 22 Furthermore, studies by Sharma et al 24 and Lewallen et al, 15 based on adult and pediatric populations, respectively, with patellar dislocation, showed no significant correlation between BMI and recurrent dislocation. However, based on the patients included in the present study, it was found that the incidence of surgical failure was significantly higher in the elevated BMI group compared with the normal BMI group. The increased rate of surgical failure may be attributed to a higher BMI, which can enhance the strain on the graft during knee joint movement, thereby affecting the stability of the patellofemoral joint.
This study discovered that MPFL reconstruction alone significantly restored the patient’s preoperative patellar position–related radiological parameters to normal, regardless of BMI. However, there was no significant difference in the improvement between the 2 groups. Consistent with our findings, Lee et al 14 observed significant restoration of the preoperative patellar tilt angle and patellofemoral trochlear congruence to normal in patients with recurrent patellar dislocation after MPFL reconstruction. Another study also reported similar results for both single-tunnel and double-tunnel fixation techniques. 3 Furthermore, studies have indicated that the postoperative change in patellar position after MPFL reconstruction is primarily influenced by surgical technique.5,10
However, there are certain limitations to consider in this study. First, it is important to note that our study is retrospective in nature and based on a small sample size obtained from a single-center hospital. Consequently, caution should be exercised when generalizing the findings to the wider population. To establish more robust conclusions, it is advisable to conduct future prospective studies with larger sample sizes involving multiple centers. Second, due to the minimum follow-up period of 12 months, the long-term impact of elevated BMI on the efficacy of MPFL reconstruction could not be adequately assessed. Third, it is important to note that the patients in the 2 groups were not enrolled concurrently, potentially leading to the introduction of selection bias. Furthermore, this study included patients with recurrent patellar dislocations of ≥2 episodes. However, the number of dislocations varied among patients, which may introduce potential bias. Last, it is worth noting that potential biases in measuring radiological parameters and collecting subjective functional scores might introduce challenges in drawing reliable conclusions. We did not measure intra- or interobserver reliability, nor were the radiological images blinded to our observers. This oversight could lead to variations in data interpretation, potentially affecting the study’s overall validity.
Based on the study findings, it is crucial to give increased attention to patients with recurrent patellar dislocation and elevated BMI during clinical diagnosis and treatment. Moreover, implementing an intensified weight reduction rehabilitation program after MPFL reconstruction surgery is essential to mitigate the risk of postoperative patellar subluxation.
Conclusion
Our study demonstrated statistically significant increases in postoperative clinical scores for both groups, although the intergroup differences varied. Specifically, patients with elevated BMI demonstrated poorer preoperative Lysholm and Tegner scores. The postoperative improvement in radiological parameters was equally good between the 2 groups.
Footnotes
Final revision submitted December 22, 2023; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received funding from the National Natural Science Foundation of China (81874017, 81960403 and 82160422), Lanzhou Science and Technology Plan Program (2021-RC-102), Natural Science Foundation of Gansu Province and Cuiying Scientific (21JR7RA393, 22JR5RA956 and 22JR5RA984) and Technological Innovation Program of Lanzhou University Second Hospital (CY2021-BJ-A13, CY2021-MS-A07 and CY2020-BJ03). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Lanzhou University Second Hospital (ref No. 2022A-224).