
Abstract
Background:
Cost analysis studies in medicine were uncommon in the past, but with the rising importance of financial considerations, it has become increasingly important to use available resources most efficiently.
Purpose:
To analyze the current state of cost-effectiveness analyses in shoulder surgery.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of the current literature was performed following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. All full economic analyses published since January 1, 2010 and including the terms “cost analysis” and “shoulder” were checked for usability. The methodological quality of the studies was assessed using the Oxford Centre for Evidence-Based Medicine levels of evidence and established health economic criteria (Quality of Health Economic Studies [QHES] instrument).
Results:
A total of 34 studies fulfilled the inclusion criteria. Compared with older studies, recent studies were of better quality: one level 1 study and eight level 2 studies were included. The mean QHES score was 87 of 100. The thematic focus of most studies (n = 13) was rotator cuff tears, with the main findings as follows: (1) magnetic resonance imaging is a cost-effective imaging strategy, (2) primary (arthroscopic) rotator cuff repair (RCR) with conversion to reverse total shoulder arthroplasty in case of failure is the most cost-effective strategy, (3) the platelet-rich plasma augmentation of RCR seems not to be cost-effective, and (4) the cost-effectiveness of double-row RCR remains unclear. Other studies included shoulder instability (n = 3), glenohumeral osteoarthritis (n = 3), proximal humeral fractures (n = 4), subacromial impingement (n = 4), and other shoulder conditions (n = 7).
Conclusion:
Compared with prior studies, the quality of recently available studies has improved significantly. Current studies could help decision makers to appropriately and adequately allocate resources. The optimal use of financial resources will be of increasing importance to improve medical care for patients. However, further studies are still necessary.
For a long time, economic evaluations including cost analysis studies were uncommon in medicine, especially in orthopaedic surgery. Because of the increasing importance of financial factors, the efficient use of available resources has become more important. In 2017, the United States spent 17.2% of its gross domestic product in the health care sector, much more than any other country (eg, Germany: 11.3%; Japan: 10.7%) and much more than in 2000, when only 12.5% of the United States gross domestic product was spent in the health care sector. 44
The purpose of economic evaluations is to analyze alternative courses of action (eg, different treatments) in terms of both their costs and consequences (eg, patient outcomes). 15 The aim should be to increase value for the patients, with “value” defined as the health outcome per dollar spent. 48 The outcome is not only the achieved health status but also the process of regeneration and the achievement of sustainable health. If a more expensive treatment method leads to faster regeneration and earlier return to work, then this method can still be cost-effective.
Cost analysis can be performed using different methods, with cost-effectiveness analysis, cost-utility analysis, and cost-benefit analysis being most common. 4,15 As a measure of outcome, the use of quality-adjusted life years (QALYs) has been widely established. 4,50 QALYs facilitate the comparison of different treatment options, and incremental cost analysis can be performed (incremental cost-effectiveness ratio [ICER]). QALYs are calculated using generic quality of health measurement tools such as the EuroQol 5 Dimensions index (EQ-5D) or Short Form–6 Dimensions (SF-6D). 5,56 However, better measurement tools for the “outcome” have not yet been established, and suitable instruments that are more specific than the EQ-5D/SF-6D but still allow comparisons between different diseases are still under development. 40,49 Investigators should study and report evidence-based results from validated, disease-specific, and patient-reported outcome measures as well as health-related quality of life measures.
By defining the threshold of what a QALY (1 year in perfect health, usually US$50,000-$100,000/QALY) may cost, resources can be better distributed among different treatment strategies. 37,39 For example, it would be more useful to support a therapy that increased quality of life by 2.0 QALYs for the cost of $50,000 than a similar therapy that also cost $50,000 but increased the QALY only by 1.0. For mathematical calculations, different models (eg, Markov, Monte Carlo) are used and various statistical methods applied to compensate for uncertainty (eg, probabilistic sensitivity analysis, 1- or 2-way sensitivity analysis) as well as the future inflation of costs (eg, discounting). See Table 1 for a brief explanation of key concepts.
Overview and Explanations of Abbreviations, Terms, and Concepts a

a EQ-5D, EuroQol 5 Dimensions; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year; QHES, Quality of Health Economic Studies; SF-6D, Short Form–6 Dimensions.
Multiple cost analysis studies and reviews have been published in sports orthopaedics over the past years, especially focusing on anterior cruciate ligament reconstruction. 41,53 In shoulder surgery, cost analysis studies have rarely been performed or are of lower quality, as stated in a review from 2012 that included literature before 2010. 27 Therefore, the aim of this work was to analyze the current state of cost-effectiveness analyses in shoulder surgery since 2010.
Methods
This systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 36 A systematic electronic search of the PubMed database was conducted in November 2019 to identify clinical studies investigating cost analysis in shoulder surgery. The following search terms were used in all fields: (cost analysis AND shoulder). Studies were limited to articles published after December 2009. In addition to the electronic search, the reference lists of all included articles were manually searched for additional relevant articles.
For the purpose of this systematic review, only clinical studies that specifically investigated full economic analyses (defined by comparing ≥2 alternative treatments and including both costs and effects) were included. Additional inclusion criteria were as follows: English-language studies, studies published online, or studies in print in a peer-reviewed journal. The exclusion criteria were as follows: narrative or systematic reviews, meeting abstracts, and proceedings.
The titles and abstracts of all articles were screened for relevance according to the inclusion and exclusion criteria. If no abstract was available, the full-text article was obtained to assess the relevance of the study. The full text was obtained and subsequently reviewed for possible inclusion in the systematic review for all articles that were not excluded during the initial screening process.
Quality Assessment
All included studies were assessed and assigned a level of evidence (level 1-5) according to the Oxford Centre for Evidence-Based Medicine (OCEBM) criteria for economic studies. 32 Level 1 and 2 studies include complex computer simulation models (Monte Carlo simulation, Markov model) with inputs derived solely from level 1 or 2 studies. 32 Additionally, the Quality of Health Economic Studies (QHES) instrument was used to assess the quality of the included studies as used in other studies in orthopaedic surgery. 41,43 There were 2 authors (T.T. and C.L.) who independently performed the evaluation, and a consensus was reached by a discussion. The QHES instrument consists of 16 “yes” or “no” questions, with each question weighted between 1 and 9 points and a total score range from 0 to 100. Scores in the range of 80 to 100 are generally considered high quality, whereas scores below 50 are typically not deemed worthy of publication. 43
Results
In the scope of this systematic literature review, 406 articles published after the end of 2009 were found that reported on cost analysis and the shoulder (Figure 1). After the exclusion criteria were applied, 34 studies that performed full economic analyses were included (Table 2). The detailed results are displayed in individual tables: 13 studies considered the topic of rotator cuff tears (RCTs) (Table 3), 3 considered shoulder instability (Appendix Table A1), 3 considered glenohumeral osteoarthritis (Appendix Table A2), 4 considered proximal humeral fractures (Appendix Table A3), 4 considered subacromial impingement (Appendix Table A4), and 7 considered other shoulder conditions (Appendix Table A5). The high-quality studies included in this systematic review show cost-effective therapeutic strategies.
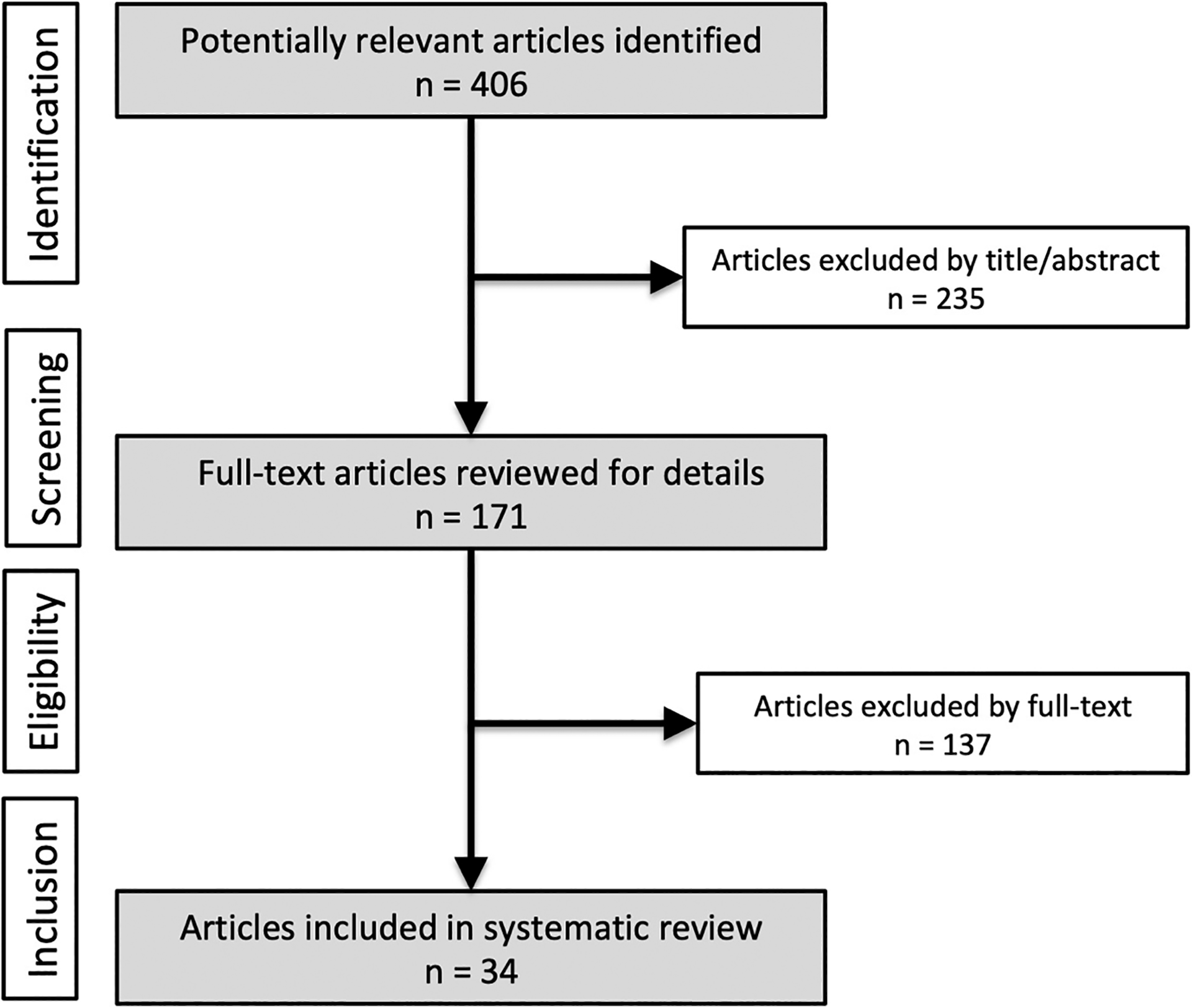
Flowchart of the search strategy in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Characteristics of Included Studies a

a ICER, incremental cost-effectiveness ratio; NHS, National Health Service; OSS, Oxford Shoulder Score; PSA, probabilistic sensitivity analysis; QALY, quality-adjusted life year; QHES, Quality of Health Economic Studies; SPADI, Shoulder Pain and Disability Index; THA, total hip arthroplasty; —, no information provided.
b All 3 studies were related to the PROFHER (PROximal Fracture of the Humerus: Evaluation by Randomisation) trial. The two Handoll et al studies were considered a single study for the purposes of this review.
Economic Evaluations Concerning RCTs (n = 13) a

a EQ-5D, EuroQol 5 Dimensions index; HA, hemiarthroplasty; ICER, incremental cost-effectiveness ratio; MRI, magnetic resonance imaging; PRP, platelet-rich plasma; QALY, quality-adjusted life year; RCR, rotator cuff repair; RCT, rotator cuff tear; RTSA, reverse total shoulder arthroplasty; SF-36, 36-Item Short Form Survey; SF-6D, Short Form-6 Dimensions; TSA, total shoulder arthroplasty.
Quality Analysis
The quality of the studies included in this systematic review was higher compared with studies before 2010. In total, there was one level 1 study, eight level 2 studies, nine level 3 studies, nine level 4 studies, and seven level 5 studies. The eight level 2 studies used complex Markov models and appropriate sensitivity analyses (Monte Carlo simulation, probabilistic sensitivity analysis). Levels of evidence and QHES scores are shown in Table 2. Before 2010, sensitivity analyses and discounting were rarely used in the shoulder literature, whereas these methods have now become common in the included studies. 27 Table 2 shows the country in which the economic analysis was performed and which models and sensitivity analyses were used. Another important criterion for a high-quality study is whether the aim of the study is clear, specific, and measurable. 8 This criterion was fulfilled by all the included studies. The quality of the data on which the models were based was the most difficult aspect to evaluate. In all except 1 presented study, 57 expert opinion was included in various amounts, as opposed to data. Therefore, only 1 level 1 study according to the OCEBM criteria could be included in this review. The mean QHES score showed that the overall study quality/methodology was good, with a mean score of 87 (range, 38-100) (Table 2). Figure 2 presents information regarding how each QHES criterion was met by the 34 studies.
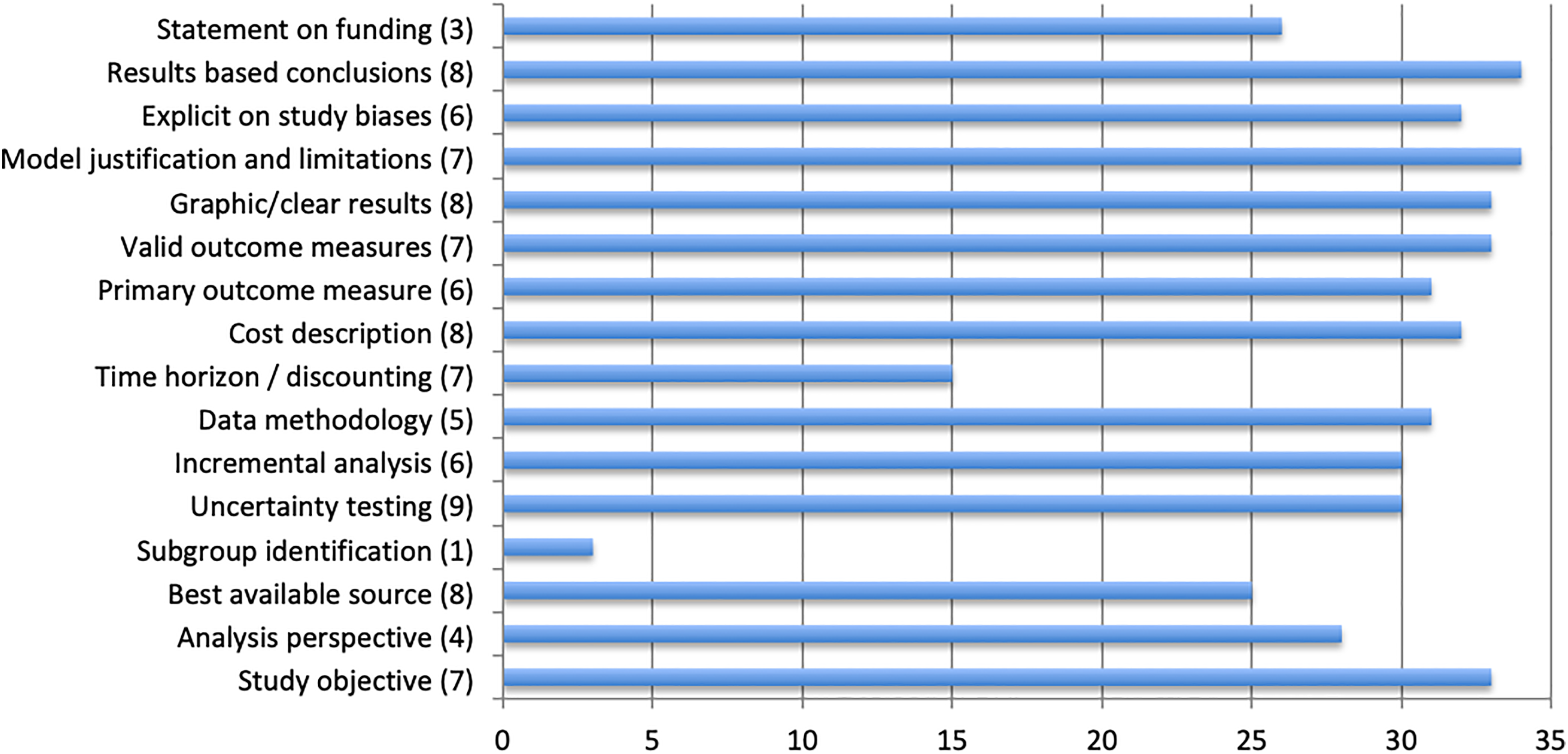
Breakdown of the overall Quality of Health Economic Studies instrument categories for all 34 included studies. The point value for each criterion is shown in parentheses.
Cost Analysis in RCTs
In total, there were 13 studies focusing on RCTs. Only 1 study fulfilled the criteria of a level of evidence 2 study, while 7 studies were level 3 (Table 3). The main findings were the following: (1) Although additional factors must be considered, such as available resources and workflow, magnetic resonance imaging is the first-choice imaging strategy based on cost-effectiveness criteria. 19 (2) Primary (arthroscopic or open) rotator cuff repair (RCR) is the most cost-effective strategy. 13,30,33 In case of failure, conversion to reverse total shoulder arthroplasty (RTSA) seems to be a cost-effective strategy. 13 Primarily, RTSA is the most cost-effective treatment option for the elderly (age not specifically defined). 26 (3) Platelet-rich plasma as a biological augmentation of RCR seems not to be cost-effective. 54 (4) The cost-effectiveness of double-row RCR remains unclear. While it does not seem to be cost-effective for any sized RCTs, the variability in costs and probability of retears might have a profound effect on the results and may create an environment in which double-row repair becomes the more cost-effective option. 16 The findings of the five level 4 and 5 studies focusing on the treatment of RCTs can be found in Table 3.
Cost Analysis in Other Abnormalities
Cost analysis for the treatment of shoulder instability showed the cost-effectiveness of both arthroscopic Bankart repair and the open Latarjet procedure in comparison with nonoperative treatment. 11,35 The Latarjet procedure was more cost-effective than revision arthroscopic Bankart repair. 29 Total shoulder arthroplasty was found to be the most cost-effective treatment option for glenohumeral arthritis. 2,3,34 Regarding proximal humeral fractures, RTSA showed economic advantages over hemiarthroplasty in the elderly (base case of 70 and 72 years) and in complex fracture situations. 42,45 A prophylactic administration of local vancomycin powder during arthroplasty was found to be highly cost-effective. 22 For the treatment of subacromial impingement, corticosteroid injections plus exercise delivered by a therapist were cost-effective when compared with exercise alone. 25 Furthermore, ultrasound-guided injections were found to be the most cost-effective option for the initial steroid-based treatment of adhesive capsulitis. 18 A 2019 level 1 study on the cost-effectiveness of surgical treatment for displaced midshaft clavicular fractures showed that surgical treatment was not cost-effective (considering a threshold of €34,000/QALY). 57 In patients with professions imposing high loads on the shoulder, however, surgical treatment was described to potentially be more cost-effective compared with nonsurgical treatment. 57 Paoli et al 46 compared superior labral from anterior to posterior (SLAP) repair, biceps tenodesis, and nonoperative treatment in their cost-effectiveness study on symptomatic SLAP tears. Primary biceps tenodesis was described to be the most cost-effective treatment option among the 3 evaluated procedures for type II SLAP tears in middle-aged patients. 46 Detailed findings of the analyzed studies can be found in Appendix Tables A1 to A5.
Discussion
Within the scope of this systematic review, 34 full economic analyses concerning shoulder abnormalities were included that have been published more recently than 2010, expanding the older reviews by Kuye et al 27 and Teusink et al. 58 In contrast to these reviews, only full economic analyses were included. Simple comparisons of costs or cost-minimization studies were disregarded. Most available studies had the perspective of the health care sector. The overall quality of recent studies has significantly improved compared with studies from 2009 and before. The results of cost-effectiveness studies are rarely transferred to daily clinical practice; in most health care systems, medical treatment is customized to the individual patient by doctors, mostly independent of costs. However, exploding costs in health care systems will inevitably lead to an emphasis on more cost-effective therapies in the future.
Representing almost 50% of all included studies, sufficient evidence now exists for the cost-effectiveness of various RCT treatment options. Magnetic resonance imaging was described to be a cost-effective imaging strategy. Primary RCR with conversion to RTSA in case of failure was the most cost-effective strategy. Platelet-rich plasma augmentation of RCR was not cost-effective, and the cost-effectiveness of double-row RCR remained unclear. For displaced proximal humeral fractures (involving the surgical neck), a randomized trial comparing surgical and nonsurgical treatment found no significant between-group differences in quality of life over time. 21 For most other abnormalities such as shoulder instability, glenohumeral osteoarthritis, or subacromial impingement, fewer high-quality studies have been published so far.
Despite several high-level studies that recently complemented the available body of literature, uncertainty remains regarding the most cost-effective treatment option for older patients with large or massive RCTs. Makhni et al 30 in 2016 analyzed the cost-effectiveness of primary RTSA versus arthroscopic RCR in patients older than 65 years. Although clinical outcomes seemed to be similar in both treatment groups, the authors highlighted the fact that the overall costs were significantly lower in the RCR treatment group, even in cases of postsurgical retears. The authors emphasized this finding by various sensitivity analyses showing that patients with retears would require progression rates to end-stage RCT arthropathy of 89% to justify early RTSA. Similarly, considering a 100% progression rate to RCT arthropathy, the authors calculated a required retear rate of 65% after arthroscopic RCR of RCTs to justify early RTSA. For newer techniques, such as superior capsular reconstruction, no cost-effective analyses are available yet.
Cost analysis on surgical techniques in arthroscopic RCR also revealed varying results. While Genuario et al 16 reported in their analysis on the cost-effectiveness of single-row RCR versus double-row RCR that double-row RCR was not cost-effective for any sized RCTs, Huang et al 23 found double-row RCR to be more cost-effective than single-row RCR in some cases, especially in larger RCTs. This discrepancy most likely results from the varying underlying costs of surgery that were used for calculations, depending on the health care system. While Huang et al based their calculations on surgery costs of $1654.76 (single-row RCR) and $2134.41 (double-row RCR) for primary and revision surgery, respectively, Genuario et al referred to surgery costs being 5 to 7 times higher. This difference strongly influences the ICER per QALY and therefore makes a direct comparison of both studies difficult.
Mather et al 33 investigated whether the operative treatment of RCTs is cost-effective from a societal perspective. A complex Markov model was therefore used based on lifelong direct and indirect costs in connection with RCTs. The surgical treatment of RCTs led to cost savings compared with nonoperative treatment depending on the patient’s age at the time of treatment (cost savings of $77,662 in 30- to 39-year-old patients). The model was validated using 1-, 2-, and 3-way sensitivity analyses and Monte Carlo simulations. The response to nonoperative treatment was found to have the biggest impact on the results. If the success rate of nonoperative therapy was increased to 88%, it would be more cost-effective. However, this high success rate is outside of the reported outcome rates for nonoperative therapy. The study by Mather et al 33 emphasizes the complexity of these models, which factors are to be included, and how errors can be minimized using simulations. However, the most important aspect is the data on which the model is based, as highlighted by Castagna et al. 7 The authors evaluated the subacromial spacer as a new treatment option, but no valid outcome data are available for this treatment method yet. 7 Therefore, the model used in the study was based on expert opinion and was prone to errors, regardless of the quality level of the study. 7 The performed sensitivity analysis showed that if the success rate of the subacromial spacer is only reduced by 20%, it would no longer be the most cost-effective strategy. This accentuates the immense importance of exact outcome measurements for economic evaluations. 48,49
The only study focusing on the prevention of infections after shoulder arthroplasty proved the cost-effectiveness of local vancomycin powder. 22 However, these results must be evaluated critically, as only 16 patients were included in a single-center study setup.
Attention should also be paid to the interpretation of the study by Paoli et al, 46 who focused on the cost-effectiveness of 3 different treatment options for symptomatic SLAP tears in middle-aged patients (mean age, 40 years). While the authors described primary biceps tenodesis to be the most cost-effective treatment option among the 3 evaluated procedures for type II SLAP tears, it needs to be highlighted that biceps tenotomy was not evaluated. 46 This efficient surgical treatment option, however, might also be cost-effective. 46
In our study, the QHES score was high (mean, 87), but according to the OCEBM level of evidence, there was only one level 1 study. This crucial difference is based on the fact that the underlying data quality is of utmost importance for OCEBM evidence levels, while the QHES score focuses on study methodology. Thereby, the study quality is rated according to the “best available” source of data. In our opinion, good study quality cannot compensate for poor underlying data, even if they are the “best available.” The example shown for Castagna et al 7 highlights that fact, and the discrepancy between both tools needs to be considered. In this regard, sensitivity analyses are very valuable.
Compared with other areas in medicine and orthopaedic subspecializations, shoulder surgery was comparable and magnitudes less expensive than, for example, new drugs, in which the ICER could exceed US$100,000 (Table 4). Therefore, the development and use of suitable quality parameters will be of utmost importance in the future to measure, evaluate, and compare the quality of medical therapies. High-quality studies (level 1) will be required to generate the needed data for economic analyses. An improved outcome (or more inexpensive therapy with the same outcome) must be proven to justify the increased costs and to compare established therapies, especially for new treatments and new medical products. Surgeons today, more than ever, have to incorporate cost-efficiency into their daily treatment strategies. Nevertheless, decisions must, of course, always be based on patient- and disease-specific factors.
Different Therapy Options for Various Diseases and Their Economic Evaluation a
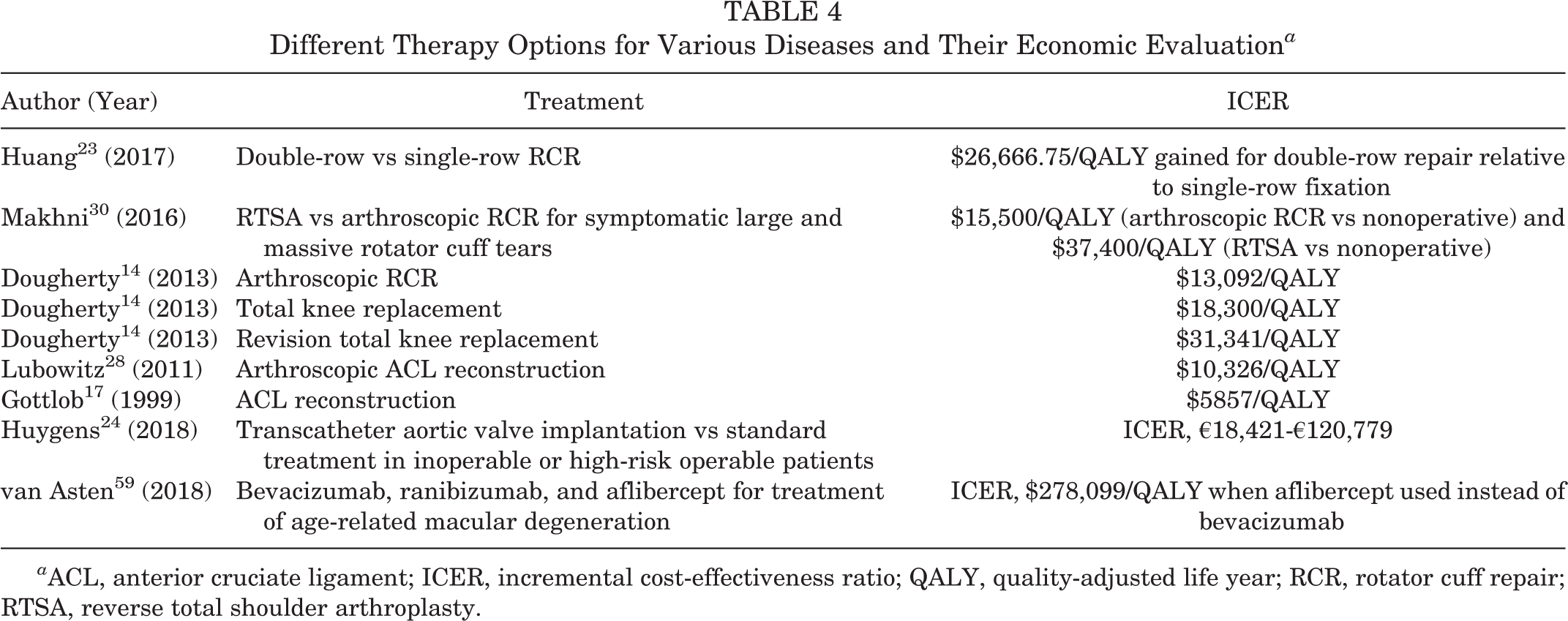
a ACL, anterior cruciate ligament; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year; RCR, rotator cuff repair; RTSA, reverse total shoulder arthroplasty.
Limitations
This study has several limitations. First, while having tried to assess the available literature as thoroughly as possible by using wide search terms, there is still a chance of having missed available studies. Second, the QHES instrument to assess research methodology represents a potential source of biased scoring. Therefore, two of the authors independently performed the evaluation, and a consensus was reached by a discussion. Third, even though most of the studies are based on good or excellent quality of data, some of the included articles do refer to studies with slightly lower OCEBM levels and QHES scores.
Conclusion
Compared with a 2012 review, 27 the study quality improved greatly. The current studies might help decision makers to appropriately and adequately allocate resources. However, further studies are still necessary.
Footnotes
Final revision submitted December 3, 2019; accepted January 21, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.T. is a paid consultant for Arthrex and Bauerfeind. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
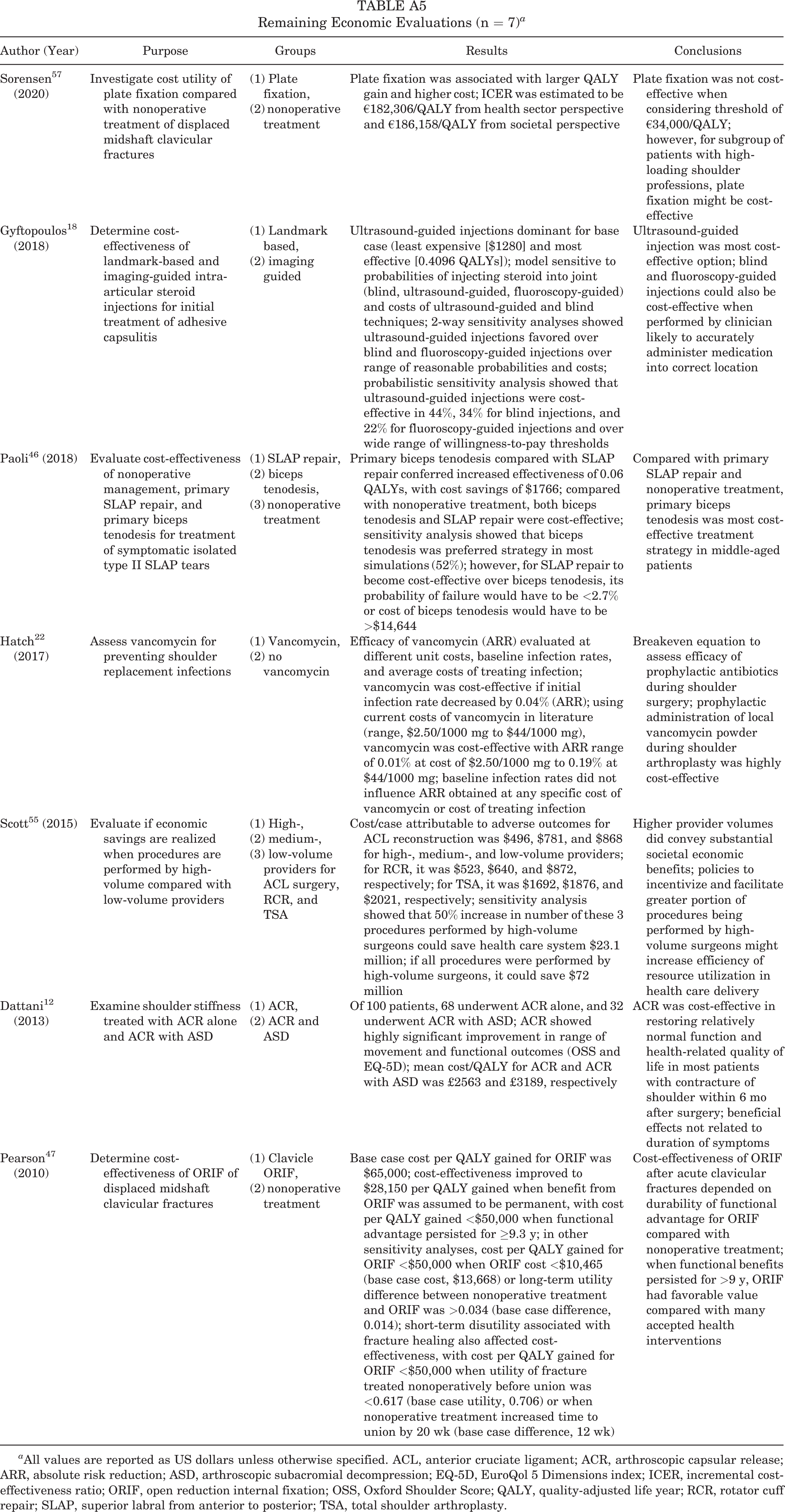
Remaining Economic Evaluations (n = 7) a
| Author (Year) | Purpose | Groups | Results | Conclusions |
|---|---|---|---|---|
| Sorensen 57 (2020) | Investigate cost utility of plate fixation compared with nonoperative treatment of displaced midshaft clavicular fractures | (1) Plate fixation, (2) nonoperative treatment | Plate fixation was associated with larger QALY gain and higher cost; ICER was estimated to be €182,306/QALY from health sector perspective and €186,158/QALY from societal perspective | Plate fixation was not cost-effective when considering threshold of €34,000/QALY; however, for subgroup of patients with high-loading shoulder professions, plate fixation might be cost-effective |
| Gyftopoulos 18 (2018) | Determine cost-effectiveness of landmark-based and imaging-guided intra-articular steroid injections for initial treatment of adhesive capsulitis | (1) Landmark based, (2) imaging guided | Ultrasound-guided injections dominant for base case (least expensive [$1280] and most effective [0.4096 QALYs]); model sensitive to probabilities of injecting steroid into joint (blind, ultrasound-guided, fluoroscopy-guided) and costs of ultrasound-guided and blind techniques; 2-way sensitivity analyses showed ultrasound-guided injections favored over blind and fluoroscopy-guided injections over range of reasonable probabilities and costs; probabilistic sensitivity analysis showed that ultrasound-guided injections were cost-effective in 44%, 34% for blind injections, and 22% for fluoroscopy-guided injections and over wide range of willingness-to-pay thresholds | Ultrasound-guided injection was most cost-effective option; blind and fluoroscopy-guided injections could also be cost-effective when performed by clinician likely to accurately administer medication into correct location |
| Paoli 46 (2018) | Evaluate cost-effectiveness of nonoperative management, primary SLAP repair, and primary biceps tenodesis for treatment of symptomatic isolated type II SLAP tears | (1) SLAP repair, (2) biceps tenodesis, (3) nonoperative treatment | Primary biceps tenodesis compared with SLAP repair conferred increased effectiveness of 0.06 QALYs, with cost savings of $1766; compared with nonoperative treatment, both biceps tenodesis and SLAP repair were cost-effective; sensitivity analysis showed that biceps tenodesis was preferred strategy in most simulations (52%); however, for SLAP repair to become cost-effective over biceps tenodesis, its probability of failure would have to be <2.7% or cost of biceps tenodesis would have to be >$14,644 | Compared with primary SLAP repair and nonoperative treatment, primary biceps tenodesis was most cost-effective treatment strategy in middle-aged patients |
| Hatch 22 (2017) | Assess vancomycin for preventing shoulder replacement infections | (1) Vancomycin, (2) no vancomycin | Efficacy of vancomycin (ARR) evaluated at different unit costs, baseline infection rates, and average costs of treating infection; vancomycin was cost-effective if initial infection rate decreased by 0.04% (ARR); using current costs of vancomycin in literature (range, $2.50/1000 mg to $44/1000 mg), vancomycin was cost-effective with ARR range of 0.01% at cost of $2.50/1000 mg to 0.19% at $44/1000 mg; baseline infection rates did not influence ARR obtained at any specific cost of vancomycin or cost of treating infection | Breakeven equation to assess efficacy of prophylactic antibiotics during shoulder surgery; prophylactic administration of local vancomycin powder during shoulder arthroplasty was highly cost-effective |
| Scott 55 (2015) | Evaluate if economic savings are realized when procedures are performed by high-volume compared with low-volume providers | (1) High-, (2) medium-, (3) low-volume providers for ACL surgery, RCR, and TSA | Cost/case attributable to adverse outcomes for ACL reconstruction was $496, $781, and $868 for high-, medium-, and low-volume providers; for RCR, it was $523, $640, and $872, respectively; for TSA, it was $1692, $1876, and $2021, respectively; sensitivity analysis showed that 50% increase in number of these 3 procedures performed by high-volume surgeons could save health care system $23.1 million; if all procedures were performed by high-volume surgeons, it could save $72 million | Higher provider volumes did convey substantial societal economic benefits; policies to incentivize and facilitate greater portion of procedures being performed by high-volume surgeons might increase efficiency of resource utilization in health care delivery |
| Dattani 12 (2013) | Examine shoulder stiffness treated with ACR alone and ACR with ASD | (1) ACR, (2) ACR and ASD | Of 100 patients, 68 underwent ACR alone, and 32 underwent ACR with ASD; ACR showed highly significant improvement in range of movement and functional outcomes (OSS and EQ-5D); mean cost/QALY for ACR and ACR with ASD was £2563 and £3189, respectively | ACR was cost-effective in restoring relatively normal function and health-related quality of life in most patients with contracture of shoulder within 6 mo after surgery; beneficial effects not related to duration of symptoms |
| Pearson 47 (2010) | Determine cost-effectiveness of ORIF of displaced midshaft clavicular fractures | (1) Clavicle ORIF, (2) nonoperative treatment | Base case cost per QALY gained for ORIF was $65,000; cost-effectiveness improved to $28,150 per QALY gained when benefit from ORIF was assumed to be permanent, with cost per QALY gained <$50,000 when functional advantage persisted for ≥9.3 y; in other sensitivity analyses, cost per QALY gained for ORIF <$50,000 when ORIF cost <$10,465 (base case cost, $13,668) or long-term utility difference between nonoperative treatment and ORIF was >0.034 (base case difference, 0.014); short-term disutility associated with fracture healing also affected cost-effectiveness, with cost per QALY gained for ORIF <$50,000 when utility of fracture treated nonoperatively before union was <0.617 (base case utility, 0.706) or when nonoperative treatment increased time to union by 20 wk (base case difference, 12 wk) | Cost-effectiveness of ORIF after acute clavicular fractures depended on durability of functional advantage for ORIF compared with nonoperative treatment; when functional benefits persisted for >9 y, ORIF had favorable value compared with many accepted health interventions |
a All values are reported as US dollars unless otherwise specified. ACL, anterior cruciate ligament; ACR, arthroscopic capsular release; ARR, absolute risk reduction; ASD, arthroscopic subacromial decompression; EQ-5D, EuroQol 5 Dimensions index; ICER, incremental cost-effectiveness ratio; ORIF, open reduction internal fixation; OSS, Oxford Shoulder Score; QALY, quality-adjusted life year; RCR, rotator cuff repair; SLAP, superior labral from anterior to posterior; TSA, total shoulder arthroplasty.