
Abstract
Background:
Plantar fasciitis is the most common cause of plantar heel pain. Several recent randomized control trials (RCTs) have been published comparing the use of platelet-rich plasma (PRP) and corticosteroids (CSs) for the treatment of plantar fasciitis.
Purpose:
To perform a systematic review of RCTs to compare whether PRP or CS injections result in decreased pain levels and improved patient outcomes in the treatment of plantar fasciitis.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
Medline, EMBASE, and the Cochrane Library were screened according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to identify RCTs comparing PRP and CS injections for plantar fasciitis. The visual analog scale (VAS) pain scores and the American Orthopaedic Foot and Ankle Society (AOFAS) scores were compared between groups at 1, 1.5, 3, 6, and 12 months, where possible. Statistical analysis was performed using RevMan, and P < .05 was considered to be statistically significant.
Results:
A total of 9 RCTs were identified comparing 239 patients with PRP with 240 patients with CS injections. At the follow-up time points, including 1-1.5, 3, 6, and 12 months, there were statistically significant differences in VAS scores in favor of PRP (P = .004, P < .00001, P < .00001, and P < .00001, respectively). At 1 and 3 months, there was no difference in AOFAS scores (P = .76 and P = .35, respectively). However, at 6 and 12 months, there was a difference in AOFAS scores in favor of PRP (P < .00001 and P < .00001, respectively).
Conclusion:
In patients with chronic plantar fasciitis, the current clinical evidence suggests that PRP may lead to a greater improvement in pain and functional outcome over CS injections.
Plantar fasciitis is a common and debilitating degenerative condition of the plantar fascia resulting from repetitive microtrauma and excessive strain on the plantar surface of the foot. 22 Plantar fasciitis is the most common cause of plantar heel pain, and its prevalence is estimated up to 7% in the general population. 4,9,13 In fact, up to 12.7% of runners have experienced plantar fasciitis at some point in their career. 21 Typically, the first-line treatment for plantar fasciitis is nonoperative therapy with anti-inflammatory medication, shoe inserts, and physical therapy providing relief. This type of nonoperative treatment is successful in up to 90% of patients with the condition. 22 In patients who do not respond to nonoperative treatment, injection therapies may be utilized.
Corticosteroid (CS) injections have served as the traditional method of injection therapy for many years. CS injections are effective because of their inherent anti-inflammatory properties; however, they are also associated with a risk of plantar fascia rupture and fat pad atrophy. 1 Furthermore, while CS may provide short-term pain relief, its long-term benefit in plantar fasciitis is questionable. A recent Cochrane review did not find any long-term benefit of CS over a placebo at 6-month follow-up. 7 With concerns regarding the long-term benefits of CS mounting, attention has been directed at other injection therapies that may offer longer term benefits. Platelet-rich plasma (PRP) has become increasingly utilized as a biologic option in the treatment of plantar fasciitis. 35 Similar to CS, PRP has strong anti-inflammatory properties, but without known adverse effects on the plantar fascia structure. PRP contains high levels of growth factors and anti-inflammatory cytokines, which basic science studies have shown to potentially ameliorate degenerative conditions. 3 While PRP has been shown to be beneficial for other degenerative conditions, there is no consensus on its use for plantar fasciitis.
The purpose of this study was to perform a meta-analysis on the randomized controlled trials (RCTs) in the literature to ascertain whether PRP or CS results in decreased pain levels and improved patient outcomes in plantar fasciitis. It was hypothesized that PRP would lead to decreased pain levels and improved patient outcomes compared with CS.
Methods
Search Strategy and Study Selection
Two independent reviewers (E.T.H., C.P.H.) performed a literature search based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and reviewed the search results, with the senior authors (E.T.H., Y.S., and J.G.K.) arbitrating in the event of persistent disagreement. 25 All studies in the Medline, EMBASE, and the Cochrane Library databases were queried from their inception to September 2019 using the following search algorithm: (plantar fasciitis OR plantar fascia) AND (prp OR platelet-rich plasma OR autologous blood OR autologous conditioned plasma OR ACP). The titles and abstracts were reviewed, and potentially eligible studies received a full-text review. In addition, the reference lists of all included studies and all literature reviews found via the search were manually screened for additional articles that met the inclusion criteria.
Eligibility Criteria
The inclusion criteria were as follows: (1) RCTs, (2) comparison of PRP and CS, (3) equivalent baseline outcome measures, (4) published in a peer-reviewed journal, (5) published in English or full translation freely available, and (6) availability of full text of studies. The following criteria were utilized as exclusion criteria: (1) nonrandomized studies, (2) retrospective studies, (3) studies that did not directly compare PRP with CS, (4) nonclinical studies, (5) review studies, and (6) studies with no full text available or that were not published in English.
Data Extraction
All relevant information was collected by the 2 independent reviewers. The level of evidence (LOE) was assessed using the criteria from the Oxford Centre for Evidence-Based Medicine. 15 The quality of the included randomized studies was assessed using the Cochrane Collaboration risk of bias tool. 11 Studies were considered to have a low risk of bias when on every item of bias a “low risk” was scored. Studies were considered to be moderate risk of bias when “high risk” or “unsure risk” on 1 or 2 items of bias were scored. Studies were considered to be high risk of bias when more than 2 items were scored as “high risk” or “unclear risk.”
Outcomes Analyzed and Statistical Analysis
The primary outcome measure was the visual analog scale (VAS) score for pain, and the secondary outcome measure was the American Orthopaedic Foot and Ankle Society (AOFAS) score. The outcome measures were reported at 1, 1.5, 3, 6, and 12 months, where possible. Statistical analysis was performed using Review Manager (RevMan Version 5.3; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration). Heterogeneity between studies was quantified using the I 2 statistic. 12 We chose an I 2 value of <25% to represent low heterogeneity and an I 2 value of >75% to indicate high heterogeneity. Fixed-effects models were used. When range was given instead of a standard deviation, the methods of Hozo et al 16 were used to calculate the standard deviation. Results were presented in terms of mean difference (MD) for continuous outcomes, with a 95% CI. A P value of < .05 was considered to be statistically significant.
Results
Literature Search
The initial literature search resulted in 278 total studies. Once duplicates were removed, 215 studies were assessed for eligibility and 15 full texts were reviewed. Nine clinical trials with 479 patients were ultimately included in this review (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) study selection flow diagram. CS, corticosteroid.
Study and Patient Characteristics
There were 9 RCTs included (LOE 1), in which 239 patients were treated with PRP and 240 were treated with CS. 2,18,19,26 –28,30 –32 Four studies (44%) were considered to be at “low risk” of bias, whereas 5 (56%) were considered “high risk” of bias. Of the studies that commented on the PRP preparation systems used, each study reported using a different system. Two studies (22%) did not report the system they used. Only 1 study (11%) reported a measurement to assure a minimum platelet concentration, and only 3 studies (33%) reported the leukocyte concentration obtained from the preparation. Additionally, 7 (78%) studies 2,18,19,27,30 –32 reported that they used a local anesthetic at the time of injection. Methylprednisolone was the most commonly utilized CS (n = 4), followed by triamcinalone utilized in 2 studies. Of note, just 2 studies (22%) utilized ultrasound guidance for their injections. 27,31
The study and patient characteristics are reported in Table 1. The injection characteristics are reported in Tables 2 and 3.
Study Characteristics a

a CS, corticosteroid; LOE, level of evidence; PRP, platelet-rich plasma.
Platelet-Rich Plasma (PRP) Injection Characteristics a

a LP, leukocyte poor; LR, leukocyte rich; N/R, not reported; RPM, revolutions per minute.
Corticosteroid (CS) Injection Characteristics a

a N/R, not reported.
VAS Pain Score
At 1-1.5 months, there was a statistically significant difference in the VAS scores in favor of PRP (6 studies, 329 patients) (MD, –0.54; 95% CI, –0.90 to –0.18; I 2 = 89%; P = .004), as shown in Figure 2A. 2,19,28,30 –32 At 3 months, there was a statistically significant difference in the VAS scores in favor of PRP (7 studies, 409 patients) (MD, –0.62; 95% CI, –0.87 to –0.36; I 2 = 68%; P < .00001), as shown in Figure 2B. 2,18,19,28,30 –32 At 6 months, there was a statistically significant difference in VAS scores in favor of PRP (4 studies, 279 patients) (MD, –0.88; 95% CI, –1.19 to –0.57; I 2 = 73%; P < .00001), as shown in Figure 2C. 18,19,31,32 At 12 months, there was a statistically significant difference in VAS scores in favor of PRP (2 studies, 139 patients) (MD, –1.63; 95% CI, –2.95 to –0.30; I 2 = 0%; P = .02), as shown in Figure 2D. 18,32

Forest plots of VAS scores at (A) 1-1.5 months, (B) 3 months, (C) 6 months, and (D) 12 months. CS, corticosteroid; PRP, platelet-rich plasma; VAS, visual analog scale.
AOFAS Score
At 1 month, there was no statistically significant difference in the AOFAS scores between the 2 treatment groups (2 studies, 110 patients) (MD, 0.64; 95% CI, –3.39 to 4.67; I 2 = 0%; P = .76), as shown in Figure 3A. 2,19 At 3 months, there was no statistically significant difference in the AOFAS scores between the 2 treatment groups (5 studies, 260 patients) (MD, 1.00; 95% CI, –1.09 to 3.10; I 2 = 64%; P = .35), as shown in Figure 3B. 2,18,19,26,27 At 6 months, there was a statistically significant difference in the AOFAS scores in favor of PRP (3 studies, 180 patients) (MD, 12.88; 95% CI, 9.94 to 15.82; I 2 = 93%; P < .00001), as shown in Figure 3C. 18,19,27 At 12 months, there was a statistically significant difference in AOFAS scores in favor of PRP (2 studies, 100 patients) (MD, 32.30; 95% CI, 28.80 to 35.80; I 2 = 95%; P < .00001), as shown in Figure 3D. 18,27 Additionally, Monto 27 found at 24 months that the PRP group had significantly improved AOFAS scores compared with the CS group.
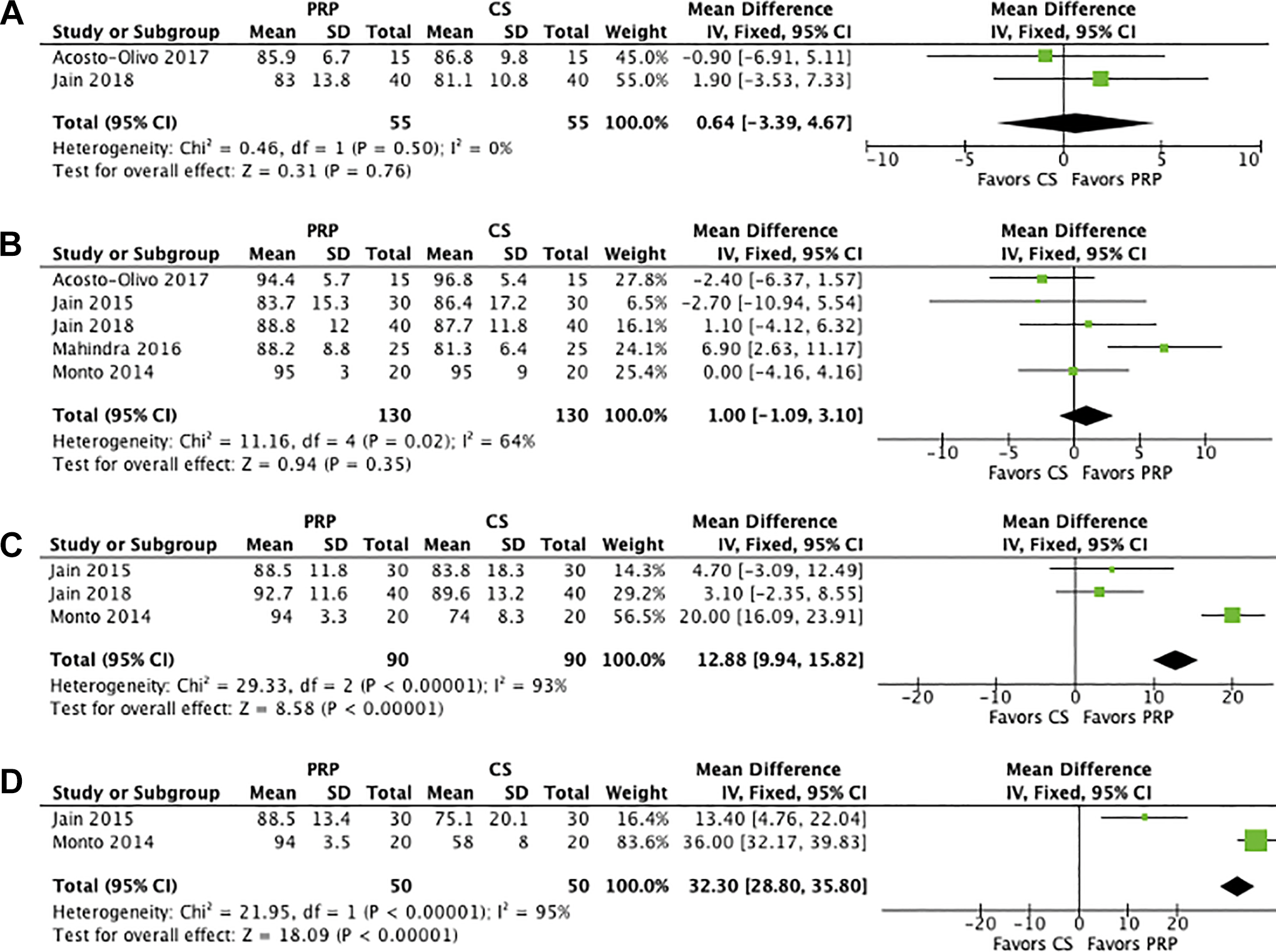
Forest plots of AOFAS scores at (A) 1 month, (B) 3 months, (C) 6 months, and (D) 12 months. AOFAS, American Orthopaedic Foot and Ankle Society; CS, corticosteroid; PRP, platelet-rich plasma.
Complications
There were no reported complications with either PRP or CS injections in any of the included studies. Six of the studies specifically reported that there were no complications. 2,18,19,30 –32
Discussion
The principal findings from the current study showed that PRP significantly reduced plantar fasciitis pain when compared with CS injection up to 6 months following treatment. Additionally, at 6-month and 1-year follow-up, the functional outcome scores were significantly improved in the PRP group compared with the CS group.
Plantar fasciitis was previously thought to be purely an inflammatory condition; however, recent evidence suggests primarily a degenerative pathology. 23 This degeneration of the plantar fascia is thought to be because of microtears, which in turn contribute to recurrent inflammation, further microtears, and a cycle of degenerative inflammation. Histologically, plantar fasciitis demonstrates myxoid degeneration, disorientation of collagen fibers, and collagen necrosis similar to tendinopathy. 23 While both PRP and CS can decrease inflammation, PRP may be advantageous over CS as it may modulate the plantar fascia degeneration because of its biological regenerative properties. PRP contains an abundance of growth factors and bioactive cytokines, which are believed to influence healing by augmenting cellular migration, improving cellular proliferation, promoting angiogenesis, and increasing matrix deposition. 3 This results in increasing fiber organization and tensile strength in soft tissue. 3 PRP also releases vascular endothelial growth factor, which promotes angiogenesis and may facilitate healing of degenerative condition by improving neovascularization and repair. 14 By contrast, CS has no such regenerative capacity, and consequently its effect will be solely in reducing inflammation and thus is short-lived.
The current study demonstrated that the functional outcomes at both 3- and 6-month follow-up were similar between the 2 groups. At 12 months, the group treated with PRP had higher functional outcome scores. This improved function may have been because of a combination of decreased pain as indicated on the VAS and the regenerative effects of the PRP. At the earlier follow-up time points, both PRP and CS had similar effects, both acting as primary anti-inflammatory agents. Therefore, early time points may result in similar outcomes. Over the course of the 12-month follow-up, the potential regenerative effects of PRP may have allowed for healing to occur, which could explain the improved outcomes in the AOFAS score with the longer follow-up. This is further substantiated by Monto, 27 who reported improved AOFAS with PRP-treated plantar fasciitis at a 24-month follow-up by comparison with 12-month follow-up. However, there are no long-term data on PRP in treating plantar fasciitis, and it is unknown whether these improved functional outcome results are maintained in the long term.
The VAS score was significantly improved in favor of PRP at all time points up to 6 months and 12 months in all studies. This finding suggests that in the setting of plantar fasciitis, PRP may be a potent pain moderator, although the exact mechanism of its action on the plantar fascia is unclear. To our knowledge, no study exists comparing the effect of PRP and CS on inflammatory cytokines in plantar fasciitis, and thus this remains of interest for further study. However, preclinical studies 6 have shown that PRP acts to reduce interleukin-1, tumor necrosis factor, and other inflammatory cytokines, thus reducing pain generators. It is not unreasonable to speculate that such a mechanism exists when injected into plantar fascia. Li et al 24 utilized ultrasound guidance for their injections, which have also been shown to improve outcomes in the patients who received CS injection therapies for plantar fasciitis. This benefit may be increased when using PRP, as the ultrasound may allow for a more localized injection into the damaged tissue and concentration of the regenerative effect.
There are several potential downsides to using CS to treat plantar fasciitis. It is a temporizing measure that may reduce inflammation, but it does not treat the underlying cause, thus recurrence may occur. Additionally, there are several complications associated with CS use, including plantar fascia rupture and skin and fat pad atrophy. Kim et al 20 reported that plantar fascia rupture was observed in 2.4% of patients who received CS injections. There are no known adverse effects other than initial local swelling and transient pain with PRP injections. However, in the current investigation, none of the included studies reported any complications with either injection.
There was poor reporting on the cytological composition of the PRP used throughout the studies, with no study measuring the platelet count and only 1 study reporting a minimum concentration. The poor reporting of the contents of PRP is not unique to plantar fasciitis. Chahla et al 5 found that the majority of orthopaedic studies poorly report the PRP preparation methods, to the extent that the studies would not be possible to reproduce based on the methods described. Future studies should include standardized reporting measures on PRP preparation. Additional studies should also focus on the leukocyte concentration of the PRP, as previous studies have shown that leukocyte-rich or leukocyte-poor PRP preparations can have differing effects on various pathologies, although no study has compared this in plantar fasciitis. 6,8,17,29 Leukocyte-poor PRP has been shown in human rotator cuff tendons to promote normal collagen synthesis and decrease inflammatory cytokines to a greater extent than leukocyte-rich PRP. 6 Similarly, Yan et al 34 found in a rabbit model for Achilles tendinopathy that leukocyte-poor PRP resulted in improved healing rates on histological analysis and decreased catabolic markers with polymerase chain reaction analysis. However, Fitzpatrick et al 10 found in a meta-analysis of PRP for tendinopathy that leukocyte-rich PRP resulted in a greater reduction in pain scores. The optimal timing and number of PRP injections would also be of great interest.
Limitations
The limitations inherent in the studies are present in this meta-analysis. The follow-up in the studies was short, and only 2 studies evaluated the outcomes at 1-year follow-up. There was a significant heterogeneity and underreporting with the AOFAS scores, which limited our conclusions regarding functional outcome. There were differences in the preparation methods of the PRP across each study and a lack of reporting on PRP composition, which may further contribute to this heterogeneity. The number of injections and the volumes and composition represent a major confounding factor in the current literature with respect to comparability between studies, and there were no data on preinjection treatment or duration of symptoms. Several of the studies did not report the randomization protocols and have the potential for selection bias, and as such, they were rated as having a high risk of bias according to the Cochrane Collaboration tool. The main outcome scores used (AOFAS and VAS scores) do not have a minimal clinically important difference score for plantar fasciitis, and the AOFAS score is not as discriminative as other outcome scores. Additionally, the included studies did not report on the athletic participation of the patients. All of the trials were also small and have the potential to be underpowered. Finally, there was no placebo control group, which would be important to evaluate in a pathology that is often self-resolving, and there were no data on postinjection physical therapy, which may be important for healing/resolution of symptoms.
Despite the inherent limitations of the current meta-analysis, there is sufficient level 1 evidence to suggest a recommendation of treatment. Using the previously described recommendation protocol by Wright et al, 33 the current study can ascribe a grade A recommendation to the use of PRP in the treatment of plantar fasciitis. No such LOE can be ascribed to CS at this time.
Conclusion
In patients with chronic plantar fasciitis, the current clinical evidence suggests that PRP may lead to a greater improvement in pain and functional outcome as compared with CS injections.
Footnotes
Final revision submitted October 8, 2019; accepted October 17, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.G.K. is a consultant for Arteriocyte. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.