
Abstract
Background:
The increase in ulnar collateral ligament (UCL) elbow reconstructions over the past 20 years has affected younger athletes more than any other age group. Although return to play and postoperative performance have been extensively studied in professional baseball players, outcomes in collegiate baseball players are less known.
Purpose/Hypothesis:
The purpose of this study was to characterize return to play and changes in performance after UCL reconstruction (UCLR) in collegiate baseball players. We hypothesized that collegiate baseball players would have similar return-to-play rates compared with professional athletes and no significant differences in performance compared with matched controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Collegiate athletes undergoing UCLR by a single surgeon were identified. Postoperatively, individual collegiate career paths were analyzed through use of publicly available data from team websites, injury reports, and press releases. Data obtained included time to return to competition, number of collegiate seasons played after surgery, total games started and played, seasonal wins, losses, saves, innings played, hits, earned run average (ERA), home runs, shutouts, strikeouts, walks, and walks plus hit per inning pitched (WHIP). The UCLR group was compared with a matched control group of collegiate pitchers without elbow injury.
Results:
Of the 58 collegiate baseball players analyzed (mean ± SD age, 19.95 ± 1.19 years), 84.5% returned to play at the collegiate level. Players returned to competition at 16.98 ± 6.16 months postoperatively and competed for 1.60 ± 0.84 seasons postoperatively. In terms of career longevity, 81.0% of collegiate pitchers either completed their collegiate eligibility or remained on active rosters, and 2 players (4.1%) ultimately played at the professional level after UCLR. Compared with a matched cohort, the UCLR group had no significant differences in collegiate pitching performance statistics after surgery.
Conclusion:
College baseball players returned to play at a rate comparable with the rate published in prior literature on professional pitchers and often completed their collegiate playing eligibility postoperatively. Compared with controls, the UCLR group had no statistically significant differences in pitching performance postoperatively. Further studies are needed to determine the exact reasons why college players retire despite having endured extensive surgical and postoperative rehabilitation processes related to UCLR. Younger populations are experiencing elbow injuries at an increasing rate secondary to increased workloads at the amateur level. As these athletes matriculate into the collegiate ranks, they are at continued risk of sustaining UCL injury, and little explicit information is available on their prospects of return to play and career longevity after UCLR.
Ulnar collateral ligament reconstruction (UCLR) is a common procedure performed in high-level baseball athletes who experience UCL injury. Several studies 1,14 have noted the increasing prevalence of UCLR, with estimated increases in surgical volume as high as 343% from 2003 to 2014. At the professional level, high rates of return to play reaching 80% to 97% have been reported, with longer term data highlighting high postoperative satisfaction and return-to-play rates near 83% across multiple levels of competition. 1,5,9,11,15,21,22 However, despite favorable subjective satisfaction scores and rates of return to play, there are conflicting reports on postoperative statistical performance data in Major League Baseball (MLB) pitchers. 5,11,15
The effect of UCL injury on younger populations is an area of interest, given the increasing prevalence of UCLR. 6,10,14 Year-round participation has become commonplace within amateur baseball, which has further contributed to the increasing risk of elbow-related overuse injuries in this population. 25 To date, much of the UCL literature has focused primarily on postoperative outcomes and return to play at the professional level, with scant information available on amateur baseball. In a study of adolescent baseball players who underwent UCLR, Saper et al 24 found return-to-play rates reaching 97%, with high satisfaction scores in patients younger than 19 years. At the collegiate level, the incidence of UCL injury in Division I baseball is estimated at 2.53%, with 56.8% of teams ultimately losing at least 1 player per year to UCL injury. Although collegiate return-to-play rates have ranged from 88% to 92%, career longevity and postoperative player performance have not been specifically investigated in this population. 1,3,22,23
Therefore, the purpose of our study was to evaluate return to play and postinjury performance of collegiate baseball pitchers after UCLR. Our primary objective was to characterize return-to-play rates, career longevity, and collegiate eligibility status after surgery. Our secondary aim was to analyze postoperative performance outcomes in collegiate baseball pitchers compared with matched controls with no history of UCLR. In addition, factors preventing players from returning to play were assessed. We hypothesized that return-to-play rates would be comparable with prior studies at the professional level and that no differences would be found in postoperative pitching performance compared with matched controls.
Methods
After obtaining approval from the internal review board and using a retrospective review of individual patient records, we identified collegiate baseball players who underwent UCLR by a single surgeon from 2009 to 2017. At the time of surgery, characteristic data were collected from each player including age at injury, current and prior level of play (ie, division of college baseball, class year), dominant throwing arm, and date of surgery. Postoperatively, all patients participated in the surgeon’s standard rehabilitation and subsequent throwing protocol before being cleared to return to competitive play. After patients completed the standard postoperative rehabilitation, information on whether players were able to return to play after surgery was documented. Publicly available team websites were used to retrospectively collect performance statistics for all seasons after a player’s return to competition. Collected demographic statistics included total collegiate games played, total collegiate games played after injury, and total seasons played. Performance statistics were collected for all seasons after a player’s return to competition.
Collected performance statistics were cross-referenced with team websites, press releases, and collegiate baseball statistical websites, including the www.thebaseballcube.com, to verify statistical data. Pitching statistics included appearances, games started, innings played per game, walks plus hits per inning pitched (WHIP), earned runs, cumulative earned run average (ERA), and per-season statistics such as games played, wins, losses, saves, complete games, innings played, hits, runs, earned runs, ERA, strikeouts, home run, shutouts, and walks. Remaining collegiate eligibility was determined based on the number of collegiate seasons played relative to 8 semesters of collegiate eligibility. 20 Information from patient records and data from relevant press releases or team websites were used to further confirm whether players had either completed eligibility, stopped playing before completing collegiate eligibility, or participated in additional redshirt years during their collegiate career. Players who did not return to play were contacted by email or telephone to both verify the end of their playing career and ascertain their reason for not returning to play.
Exclusion criteria from the final analysis included the following: (1) players actively recovering from surgery, (2) athletes participating in recreational or non-baseball-related sports, (3) players who were unable to be definitively identified via publicly available online information; (4) players lacking specific performance data or statistics, and (5) players undergoing revision procedures (Figure 1). Players actively recovering from surgery were those athletes within the cohort who were not yet cleared for competitive play by the operating surgeon. Postoperatively, all players progressed through a standard-of-care throwing regimen.

CONSORT (Consolidated Standards of Reporting Trials) diagram of analyzed players. UCL, ulnar collateral ligament.
A matched control group of healthy collegiate pitchers was assessed to provide baseline statistics and compensate for any changes in performance related to additional experience as a collegiate pitcher. The process for choosing control pitchers involved a systematic evaluation of UCL-reconstructed pitchers for characteristics such as arm dominance, level of experience at time of injury, year of injury, collegiate baseball team, current level of play, and number of collegiate games played before injury in a method described in prior studies. 5,11,15,19 Using these characteristics, we identified a control pitcher from the same team (level-of-play match) as the UCL-injured pitcher during the same year of return to play (time-era match). The control player was also assessed for average innings played per season of interest (workload and experience match). If these criteria were not met, the control selection process was repeated within the same year and team until an adequate match was found. Demographic and performance statistics for control pitchers were collected in the same manner as for their respective injured counterparts. Pitching statistics for the controls were obtained relative to the matched pitcher’s return-to-play years.
Statistical Analysis
Data on all injured players and controls were analyzed through use of descriptive statistics, including means, standard deviations, counts, and percentages. Continuous and categorical characteristic variables, categorical operative characteristics, and continuous performance variables were compared between cases and matched controls. Continuous variables were assessed for normality through use of the Shapiro-Wilk test. Continuous characteristic data were found to have a normal distribution, and Student t tests were used for comparisons between cases and controls. Categorical variables such as position, class year, level of collegiate play, operative technique, and graft type were compared through use of the chi-square test. Player performance data were deemed nonparametric according to the Shapiro-Wilk test, and thus, Mann-Whitney U tests were used to compare injured players versus a matched cohort. Statistical significance was determined using a P value less than .05; however, because multiple statistical comparisons were performed, a Bonferroni correction was applied to the analyses of performance measures between cases and matched controls. All statistical analyses were performed with STATA software (StataCorp).
Results
A total of 58 collegiate baseball players who underwent UCLR were identified and included in the study. The studied cohort had a mean ± SD age of 19.95 ± 1.19 years and consisted of 84.5% pitchers and 82.8% right-handed throwers. Within the studied cohort, 43.1% of players competed at the Division I level, 31.0% at the Division II level, and 15.5% at the Division III level. Demographic and operative characteristics of all studied players are provided in Table 1. Of the players studied, 84.5% (n = 49) were able to return to competitive collegiate gameplay at a mean ± SD of 16.98 ± 6.16 months after UCLR and were able to play a mean ± SD 1.60 ± 0.84 seasons postoperatively. More than half (83.7%) of the players who returned to play were underclassman at the time of injury, with freshmen composing 63.3% of the cohort. A statistically significant difference was found related to class year, as no senior baseball players were able to return to play postoperatively (P = .020).
Characteristic Data of All Collegiate Baseball Players After UCLR a

aData are expressed as mean ± SD or n (%). UCLR, ulnar collateral ligament reconstruction.
Overall, 79.6% of all players studied either completed their collegiate eligibility or remained on active rosters. Specifically, 20.4% (n = 10) of all players did not complete their remaining collegiate eligibility, whereas 42.9% (n = 21) were still actively playing and 36.7% (n =18) ultimately completed their eligibility. Of the 21 players who completed their collegiate eligibility, 2 (4.1%) were able to play professionally after recovering from surgery. No reoperations were noted across players studied. All players continued to play their preoperative position, with the exception of 1 athlete who switched from pitching to a fielding position. Among UCLR players and controls, we found no statistically significant differences in age (19.88 ± 1.18 vs 20.35 ± 1.20, respectively; P = .274) or preoperative games played (14.67 ± 22.8 vs 17.67 ± 22.0, respectively; P = .718). Among players who did not return to play, 1 player stopped playing because of a coaching decision, 1 player retired because of ongoing postoperative pain, 1 player retired because of an unrelated biceps tendinitis injury sustained during the rehabilitation process, 1 player cited “psychological concerns” postoperatively, 2 players stopped playing to focus on academics, and 1 player graduated despite potentially having the option for a medical redshirt. The remaining 2 players could not be reached despite several attempts to contact them. Overall, 44.4% (n = 4) of players who did not return to play cited reasons unrelated to physical injury.
A subgroup analysis of only pitchers (n = 42) found a trend toward younger players returning to play postoperatively (age of those who returned, 19.81 ± 1.18 years; age of those who did not return, 20.3 ± 1.32 years; P = .256) at a mean of 16.98 ± 6.16 months. This finding was not statistically significant; however, our analysis found significant differences in the number of senior athletes who were able to return to play postoperatively, as no seniors returned to play after surgery (P = .008). Postoperatively, 81.0% of collegiate pitchers either completed their collegiate eligibility or remained on active rosters. Among pitchers, 19.0% (n = 8) retired before finishing their eligibility, whereas in the control group, 4.7% (n = 2) retired before finishing their collegiate eligibility (Table 2).
Characteristic Data of Collegiate Baseball Pitchers After UCLR a

a Data are expressed as mean ± SD or n (%). UCLR, ulnar collateral ligament reconstruction.
b One pitcher transitioned to a fielding position postoperatively and was excluded from subgroup analysis.
Compared with level-of-play, time-era, and workload-matched controls (n = 42), analyses of player performance statistics in collegiate pitchers found no statistically significant differences in postoperative appearances, games started, innings played per game, WHIP, earned runs, cumulative ERA, and season-related statistics such as games played, wins, losses, saves, complete games, innings played, hits, runs, earned runs, ERA, strikeouts, home run, shutouts, and walks. Complete comparisons of postoperative pitching performance statistics can be found in Table 3.
Postoperative Performance Statistics After UCLR in Collegiate Pitchers Compared With Matched Controls a
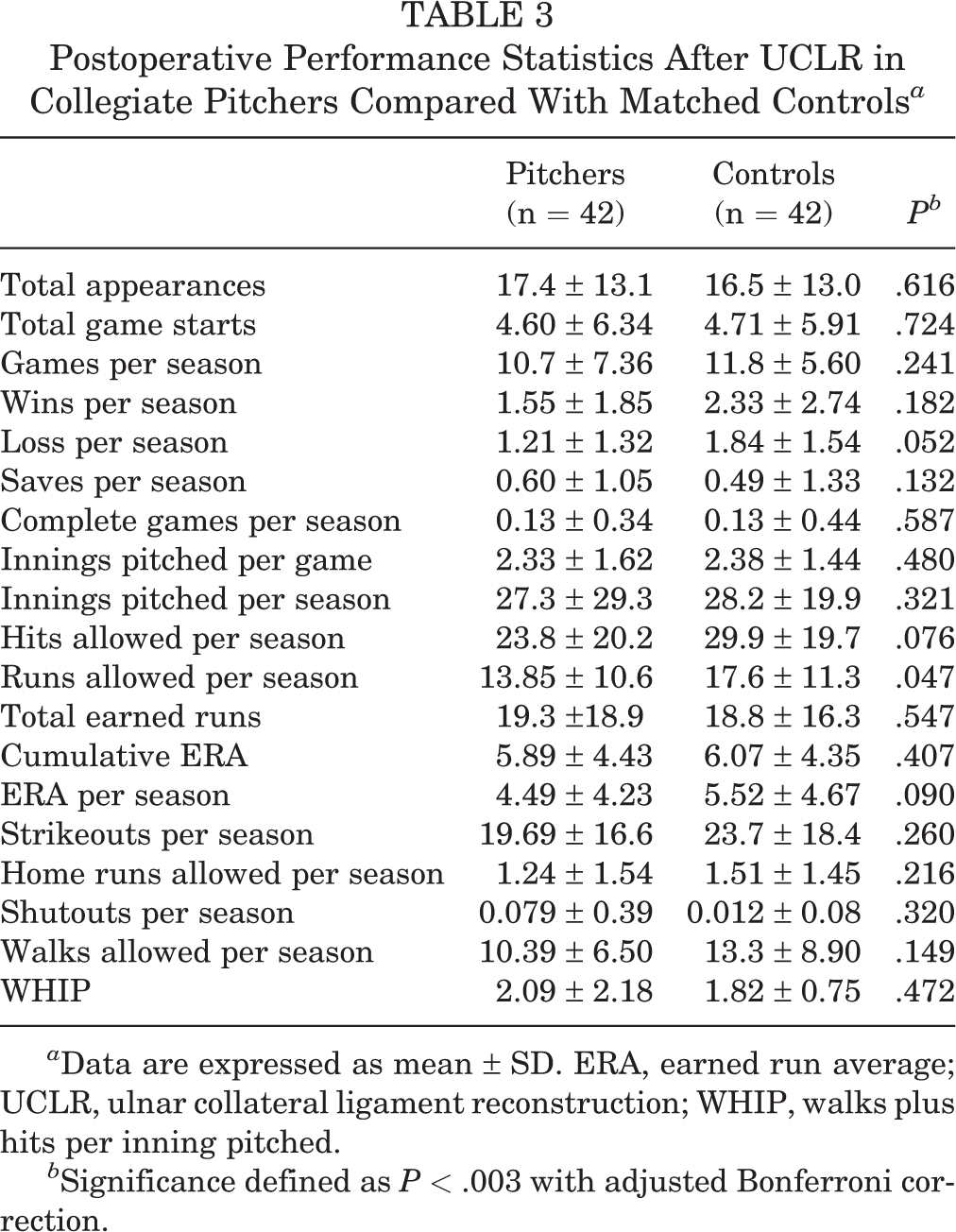
a Data are expressed as mean ± SD. ERA, earned run average; UCLR, ulnar collateral ligament reconstruction; WHIP, walks plus hits per inning pitched.
b Significance defined as P < .003 with adjusted Bonferroni correction.
Discussion
Prior studies have determined return to play as well as postoperative player performance after UCLR; however, these investigations have focused on professional baseball with less attention given to college athletes. 5,11,15,17 Our study evaluated return to play and career longevity, in the context of remaining collegiate eligibility, and characterized performance among collegiate pitchers after UCLR. Ultimately, 84.5% of all players were able to return to play at the collegiate level and compete for an average of 1.60 seasons postoperatively, with pitchers playing for a slightly longer period of 1.69 seasons after surgery. In terms of career longevity, 79.6% of all players and 81.0% of pitchers either completed their collegiate eligibility or remained on active college rosters after surgery. Underclassmen composed the majority (83.7% of all players vs 83.3% of pitchers) of players who were able to return to competition after UCLR, highlighting a link between class year and the likelihood for return to sport. Furthermore, no reoperations or revisions were performed across the study population. Compared with more recent literature analyzing UCLR outcomes across more heterogeneous populations of collegiate sports, our study solely examined college baseball players and found similar rates of return to play. 2,4 We also found no statistically significant differences in postoperative pitching statistics upon return to play relative to matched controls. As previously mentioned, the majority of current literature on UCLR has been dedicated to return to play in professional athletes. 4,11,16 Our study differs in that it provides additional information on both the performance and career longevity of a population that is becoming directly subject to the increasing prevalence of UCL injuries in overhead athletes. 6,10,14
Rothermich et al 23 found underclassmen and pitchers to be at a high risk of UCL injury; freshman accounted for 37.3% of players undergoing surgery, whereas only 8.2% were seniors. To an extent, our findings are consistent with the results reported by Rothermich et al in terms of timing of injury, as our cohort was also predominantly composed of freshmen athletes. Most players in the studied cohort experienced injury within the first 2 years of entering college yet were able to sufficiently recover in enough time to compete and still maintain or complete their eligibility. It can be argued that the cause of UCL injury early in a player’s college career is likely multifactorial. As adolescents transition from high school to college baseball, the acute increase in the intensity of the collegiate game only adds to the prior repetitive stresses and potential long-term effects that have been inflicted onto the thrower’s elbow since early adolescence. 13
Younger players have more potential years of play and therefore appear more incentivized to undergo corrective surgery. However, older players who become injured may simply retire given the long recovery that awaits. Our investigation does not enable us to make claims about the preinjury pitching volume or antecedent elbow symptoms of every athlete studied; however, prior studies have investigated the association between elbow pain and patient-related factors such as weightlifting during the season, gameplay outside of league play, in-game arm fatigue, and pitch counts upward of 600 pitches per season in youth pitchers. 13 Further, adjustments in training regimens and playing volume during the transition from high school to collegiate sports may be a contributing factor leading to UCL injury. Collegiate coaches and trainers must be mindful of the throwing mechanics of incoming college baseball players and must quickly optimize these factors to mitigate preventable injuries early on.
In MLB pitchers, data on athletic performance after UCL have varied pertaining to postoperative ERA and WHIP, with many studies citing equivalent postoperative outcomes. 5,7,11,15 More recently, a systematic review by Coughlin et al 2 pooling in-game statistical data found an overall decline in pitching performance in MLB players postoperatively; however, comparable trends in the pitching statistics at the collegiate level remain largely unknown. We found no statistically significant differences in pitching performance statistics of players who underwent UCLR compared with a matched control group of collegiate baseball players, and thus our study provides data supporting the efficacy of UCLR in helping players remain competitive postoperatively at the collegiate level. 7,12
College sports are subject to a variety of external factors not seen at the professional level; collegiate injuries are assessed and managed not only relative to seasonal timing but also in reference to their effect on player development, scholarship retainment, and eligibility constraints. Within the study cohort, 36.7% of all baseball players and, specifically, 38.1% of pitchers who returned to competition completed their collegiate eligibility. At the time of study, an additional 42.9% in each group were still playing on active college rosters. Our investigation provides some explanation as to why individual athletes within our cohort did not return to play; 44.4% of players who did not return said that they retired for reasons other than a physical injury. After UCLR, more than a year of rehabilitation is typically needed before attempting a return to competition. Although the connection between pain and depression in competitive collegiate athletes has been well established and cannot be overlooked, we have yet to fully understand the psychological factors that arise as players rehabilitate after UCLR. 26 Both injury and the rehabilitation process can have a profound effect on an athlete, especially when framed in the context of an amateur athlete’s career prospects, his or her ability to maintain a scholarship, and the finite time pressures inherent to college sport. For example, for older players with limited remaining eligibility, awareness of such a prolonged recovery period could negatively affect their interest in continuing to play and ultimately lead them toward early retirement or nonoperative management. This point may serve as a rationale for why younger athletes returned to play at a higher rate than older athletes; the younger athletes had relatively short playing careers before injury and may have had different motivations and fewer deterrents, leading them to continue competing at the collegiate level. Further study on these external influences and psychological factors in college sports would be helpful in understanding how they can potentially affect college athletes and their playing careers. Additionally, improved knowledge on how to manage such factors in the postoperative and rehabilitative period would help team physicians, trainers, and therapists in gauging the appropriate timing for return to play and prevent premature attempts that could induce further psychological harm through poor athletic performance.
Limitations
This study had several limitations. Similar to prior investigations using a similar study design, 5,11,15 this is a retrospective study that used public, web-based information to collect data. As a result, some of the data are limited by potentially inaccurate reporting and conflicting information. Although controls were matched according to time-era, workload, and level of play, the nature of publicly available data limited our ability to also match according to age because a large number of collegiate team websites lacked basic information such as date of birth. As such, more detailed matching using pitch counts or starter or relief status as a proxy of playing volume was not feasible. Additionally, inherent to collegiate athletics, the finite length of eligibility restricts long-term analyses of performance and career longevity. As such, the effect of UCLR on a player’s career can be viewed only in the context of the collegiate game. Another potential limitation secondary to the collegiate population is the relative skew of the data toward underclassmen. A reliable assessment of baseline performance was limited, as most younger players lacked significant preinjury data either because of minimal playing time preoperatively or because of inconsistent documentation of statistical data at the high school level.
Because our data rely on the accuracy of public reports, verification of the true timeline of competitive play cannot be obtained, and return-to-play data are inherently limited by the quality of individual team websites and available press releases. This limitation is not specific to affected players but also applies to those selected as controls. To address this limitation, we cross-referenced player data between several websites to ensure accuracy. This data collection method has been previously used in several valuable studies showing good reliability with results. 5,11,15,19 Further, it is possible that reinjuries occurred after a player was cleared to return to play and were ultimately treated nonoperatively. Even though these players did not undergo operative intervention, these reinjuries could still have a negative effect on the overall rate of return to play across the cohort. Last, given the low sample size, the study is susceptible to the possibility of type II error. However, the sample size is comparable with samples in prior studies on pitching performance after UCLR in MLB. 8,17,18
Despite these limitations, our investigation has several strengths: It provides homogeneity because it analyzes a single surgeon’s series of UCLRs, it is one of few studies to explicitly investigate return to play in collegiate baseball players in the context of remaining eligibility, and it remains one of the first studies to analyze postoperative performance data compared with a matched cohort of control players within this age group.
Conclusion
UCL injuries in college athletes present challenges not often seen at the professional level, such as scholarship retainment, player development, and seasonal and career-related pressures. Our study demonstrated that collegiate baseball players returned to play at a rate comparable with prior literature on professional pitchers and were often able to complete their collegiate playing eligibility postoperatively. Compared with controls, UCLR pitchers showed no significant differences in pitching performance postoperatively. Further study is needed to determine the exact reasons why college players retire despite having endured extensive surgical and postoperative rehabilitation processes related to UCLR.
Footnotes
Final revision submitted December 4, 2019; accepted December 23, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.P.T. has received grant support from Arthrex (via OrthoCarolina Research Institute) and educational support from Smith & Nephew and Peerless Surgical. C.S.A. has received research support from Major League Baseball and Stryker; royalties, consulting fees, and speaking fees from Arthrex; hospitality payments from Arthrex and DePuy; and royalties from Lead Player; and he has stock or stock options in At Peak. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Columbia University Institutional Review Board (protocol No. IRB-AAAR7012).