
Abstract
Background:
The treatment of irreparable rotator cuff tears (IRCTs) is a significant challenge, and various treatment options have emerged. Superior capsular reconstruction (SCR) is a promising procedure for patients with IRCTs.
Purpose:
To investigate the clinical outcomes of SCR and compare allografts with autografts.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search for relevant articles was carried out using the PubMed, Cochrane Library, Embase, Scopus, and Google Scholar databases. We used medical subject heading (MeSH) terms and natural keywords (superior AND (capsule OR capsular) AND reconstruction). Also, we filtered for high-quality articles using the Methodological Index for Non-Randomized Studies (MINORS). We summarized the characteristic data and commonly used outcome measures of each included study and performed a descriptive analysis using an evidence-based tendency concept as proposed by Huisstede et al (2013).
Results:
A total of 10 articles (374 shoulders) with a mean follow-up of 27.2 months were selected and analyzed. There were 4 articles on SCR with an autograft, 4 on SCR with an allograft, and 2 on SCR with both an autograft and allograft. For autografts and allografts, respectively, the mean gain in forward elevation (FE) was 48.7° and 33.3°, the visual analog scale for pain score improved by 3.5 and 3.3, the American Shoulder and Elbow Surgeons (ASES) score increased by 47.3 and 31.9, and the acromiohumeral distance increased by 1.2 and 1.8 mm. In addition, the number of graft tears was 16 (10.0%) and 17 (12.9%), the number of other complications was 12 (7.5%) and 6 (3.9%), and the number of reoperations was 5 (3.1%) and 14 (8.2%) for autografts and allografts, respectively.
Conclusion:
Both autografts and allografts improved clinical outcomes. Although the graft tear rate appeared similar between the autograft and allograft groups, the autograft group had no cases of conversion to reverse total shoulder arthroplasty. In addition, we found 3 evidence-based tendencies: (1) a tendency for both autografts and allografts to have significantly improved FE and clinical scores, (2) a tendency that autografts improved internal rotation and allografts improved abduction, and (3) a weak tendency that autografts improved abduction and allografts improved internal and external rotation. Although it was not possible to compare the groups statistically, the differences in ASES scores might be clinically important and will need to be explored in future comparative studies.
The treatment of irreparable rotator cuff tears (IRCTs) has long been considered a challenge. Various treatments have been reported, including nonoperative treatment, debridement and biceps tenotomy, 2,39 tuberoplasty, 17 partial repair, 4 tendon transfer, 9,16 bridging patch graft suturing, 10,14,15,34 and reverse total shoulder arthroplasty (rTSA). 6,30 In elderly patients with IRCTs, rTSA has shown good results in the recovery of range of motion (ROM) and pain relief. However, rTSA has shown high rates of failure when performed on young patients and so is considered inappropriate for these patients. 36,37
Biomechanical analysis has found that the effect of the superior capsule on shoulder joint function is important. 28 Therefore, superior capsular reconstruction (SCR) using a fascia lata autograft was devised by Mihata et al 24 and was reported to have achieved good early results. However, because of concerns about donor site morbidity and the additional time and effort associated with autograft harvest, an SCR procedure using dermal allografts has been developed recently. 11 SCR using dermal allografts has been performed in many patients with IRCTs. 8,12,32,33 Although dermal allografts do not have any donor site morbidity and their use can shorten the operation time, there are concerns about low viability, graft rejection, infections, and high cost.
The purposes of this systematic review were to summarize the literature on the results of the SCR procedure using allografts or autografts, to compare the results according to the source of the graft through descriptive analysis, and to investigate the tendencies in SCR treatment by reviewing high-quality articles selected with a methodological assessment. We hypothesized that SCR with allografts would show a similar clinical outcome to SCR with autografts.
Methods
In preparation for this systematic review, we followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 29
Inclusion and Exclusion Criteria
We included all relevant articles and conference abstracts to incorporate as many research results as possible. The reasons for including a conference abstract in this study were as follows: (1) SCR is a procedure that has been popular since 2013; (2) a preliminary search was conducted before the start of the study, and only a small number of studies reported SCR results; and (3) our primary goal was to analyze the clinical outcomes of SCR comprehensively. Clinical studies or conference abstracts that included adult patients with IRCTs and reported the clinical outcomes of SCR were eligible for inclusion. Studies that did not separate SCR results from tendon transfer and bridging patch graft suturing cases, included SCR using a remnant biceps tendon as an autograft, and studies with ≤5 cases were excluded.
Search Strategy and Study Selection
We searched PubMed, Embase, and Cochrane Library to find relevant articles. To increase sensitivity, we used natural keywords as well as MeSH terms and Emtree: superior AND (capsule OR capsular) AND reconstruction. After eliminating duplicate articles, selection was performed using the previously established inclusion and exclusion criteria. A total of 2 independent reviewers selected the first candidates through the title and abstract and then selected the final articles through a full-text review. We also conducted citation tracking to find additional related articles using Scopus and Google Scholar databases. Any disagreement that occurred in the selection process was resolved through a group discussion or intervention by a third reviewer.
Data Extraction
After the assessment for study selection, 2 independent reviewers extracted the data from the selected articles. The collected data were as follows: level of evidence, number of patients and shoulders, sex, age, dominant side, surgical procedures, graft (thickness), rehabilitation program, follow-up, pain score, ROM, functional outcomes, reoperations, graft tears, and other complications. We considered a graft tear or failure as an important complication and examined these individual items separately from other complications. We included all cases of wound problems, infections, neurovascular symptoms, tears in other areas except grafts, and those in which the authors referred to “complications.” Each study differed in the measurement method of the results, and there were little key data such as standard deviations among the data presented, so meta-analysis or statistical analysis could not be performed. Therefore, descriptive analysis was carried out on data such as ROM, visual analog scale (VAS) for pain score, American Shoulder and Elbow Surgeons (ASES) shoulder score, complications, and reoperation rate to investigate the clinical results of SCR and the results of each graft sampling method.
Methodological Assessment
Levels of evidence were assessed according to the Oxford Centre for Evidence-Based Medicine (https://www.cebm.net/). The risk of bias for each study was assessed using the Methodological Index for Non-Randomized Studies (MINORS). The MINORS evaluation tool consists of 8 common items plus 4 additional items for research with the comparative group. Each item can have a score of 0, 1, or 2, with maximum scores of 16 points for a noncomparative study and 24 points for a comparative study. 29 A high total score means that the study is of high quality and has a low risk of bias. In this study, we decided to include articles that achieved more than 60% of the total possible MINORS score (15/24 points or 10/16 points).
Data Analysis
In our descriptive analysis, the primary outcome measures analyzed were ROM, complications, and reoperations. We also analyzed the change in outcome according to graft tears. An inherent drawback of this study was that strong evidence could not be derived, as only level 3 or 4 studies were included. Therefore, we decided to analyze articles using an evidence-based tendency concept as proposed by Huisstede et al, 13 in which having a “tendency” indicates that several high-quality studies on a specific topic have been found and that most studies have provided consistent findings. A “weak tendency” means that only 1 high-quality study has been found for a particular subject’s suggesting findings, and “conflicting tendency” means that there are conflicting opinions in several high-quality studies. If no high-quality research on a specific topic has been found, it is considered “no tendency.”
Results
Search Results
In the first step, 286 articles were retrieved from PubMed, 303 articles from Embase, and 6 articles from the Cochrane Library. After eliminating duplicates, 403 articles were screened by title and abstract. Regarding studies with cohort overlaps, a single article was chosen based on the following criteria: A published article rather than a conference abstract. An article published more recently. An article with a larger number of patients.
This led to the exclusion of 5 articles. 1,3,22 –24,31 Ultimately, 17 candidates were identified. After a full-text review of the 17 studies, 8 articles were included in the systematic review, and 1 additional article was found through citation tracking from the selected articles. Also, we carried out a search update to find new studies and found 1 new article. Figure 1 shows the flow diagram of the whole process and the reasons for exclusion. There were no randomized controlled trials (level 1) and no prospective comparative studies (level 2). Overall, 1 level 3 and 8 level 4 studies plus 1 conference abstract were included.

Flow diagram showing the selection of appropriate articles.
Summary of Outcomes of Each Article
Table 1 summarizes the characteristic data and outcomes of each study. Essentially, 4 articles 7,19,21,35 showed the results of autografts, 4 articles 8,12,32,33 showed the results of allografts, and 2 articles 18,40 showed the results of using both autografts and allografts. The distributions of age and follow-up are shown in Figures 2 and 3, respectively. Although age distributions were similar throughout the articles, the follow-up duration varied. Most of the articles used parallel 2 or 3 anchors to fix the medial side except for 3 studies: Rosales-Varo et al 35 used 1 metallic screw, Hirahara et al 12 used a partial articular supraspinatus tendon avulsion bridge–type configuration (2 by 1), and Pennington et al 32 used 3 push-in anchors. Most of the articles used a double-row configuration (2 by 2) to fix the lateral side except for 2 studies: Rosales-Varo et al 35 used 2 metallic screws, and Lee and Min 18 used 2 anchors (single-row configuration). All of the articles that reported margin convergence suturing performed posterior margin convergence suturing, whereas 5 of 8 articles also performed anterior margin convergence suturing. Postoperative rehabilitation varied by study. Outcomes were evaluated using various tests and measurement methods for each study, and the following were frequently used: ROM (9 articles), ASES score (8 articles), VAS for pain (7 articles), Constant-Murley score (5 articles), strength (5 articles), acromiohumeral distance (AHD; 8 articles), presence of a graft tear (9 articles), other complications (8 articles), and reoperations (10 articles). Table 2 shows the results of each article for commonly used measures.
Characteristic Data and Outcomes of Individual Studies a

a ABD, abduction; AHD, acromiohumeral distance; allo, allograft; A/S, arthroscopic; ASES, American Shoulder and Elbow Surgeons; auto, autograft; DASH, Disabilities of the Arm, Shoulder and Hand; ER, external rotation; FE, forward elevation; IR, internal rotation; JOA, Japanese Orthopaedic Association; lat, lateral; LDT, latissimus dorsi transfer; med, medial; NA, not available; PASTA, partial articular supraspinatus tendon avulsion; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; SCD, superior capsular distance; SF-12, Short Form–12 Health Survey; SPADI, Shoulder Pain and Disability Index; SST, Simple Shoulder Test; SSV, subjective shoulder value; TFL, tensor fasciae latae; UCLA, University of California, Los Angeles; VAS, visual analog scale.
b Conference abstract.
c Metallic screw with 4 strands.

Summary plots for age distribution.

Summary plots for follow-up duration.
Results of Superior Capsular Reconstruction a

a Data are reported as mean ± SD (range) unless otherwise indicated. ABD, abduction; AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FE, forward elevation; IR, internal rotation; NA, not available; VAS, visual analog scale.
b Statistically significant change (P < .05).
c There were 3 different methods used to measure IR.
d The highest level of the vertebral body that the patient’s thumb could reach.
e There were 5 points (lateral thigh = 0, buttock = 1, sacrum = 2, lumbar = 3, and T7 = 5).
f Spinal segment T1 was designated as 1, T12 as 12, L1 as 13, and L5 as 17.
Comparison Between Autografts and Dermal Allografts
Table 3 shows a comparison of clinical outcomes for autografts versus allografts, and Table 4 summarizes graft tears, other complications, and reoperations. For autografts and allografts, respectively, the mean gain in forward elevation (FE) was 48.7° and 33.3°, the VAS for pain score improved by 3.5 and 3.3, the ASES score increased by 47.3 and 31.9, and the AHD increased by 1.2 and 1.8 mm. Although statistical significance could not be analyzed, a somewhat large difference was observed between graft types.
Outcomes Between Autograft and Allograft Groups a
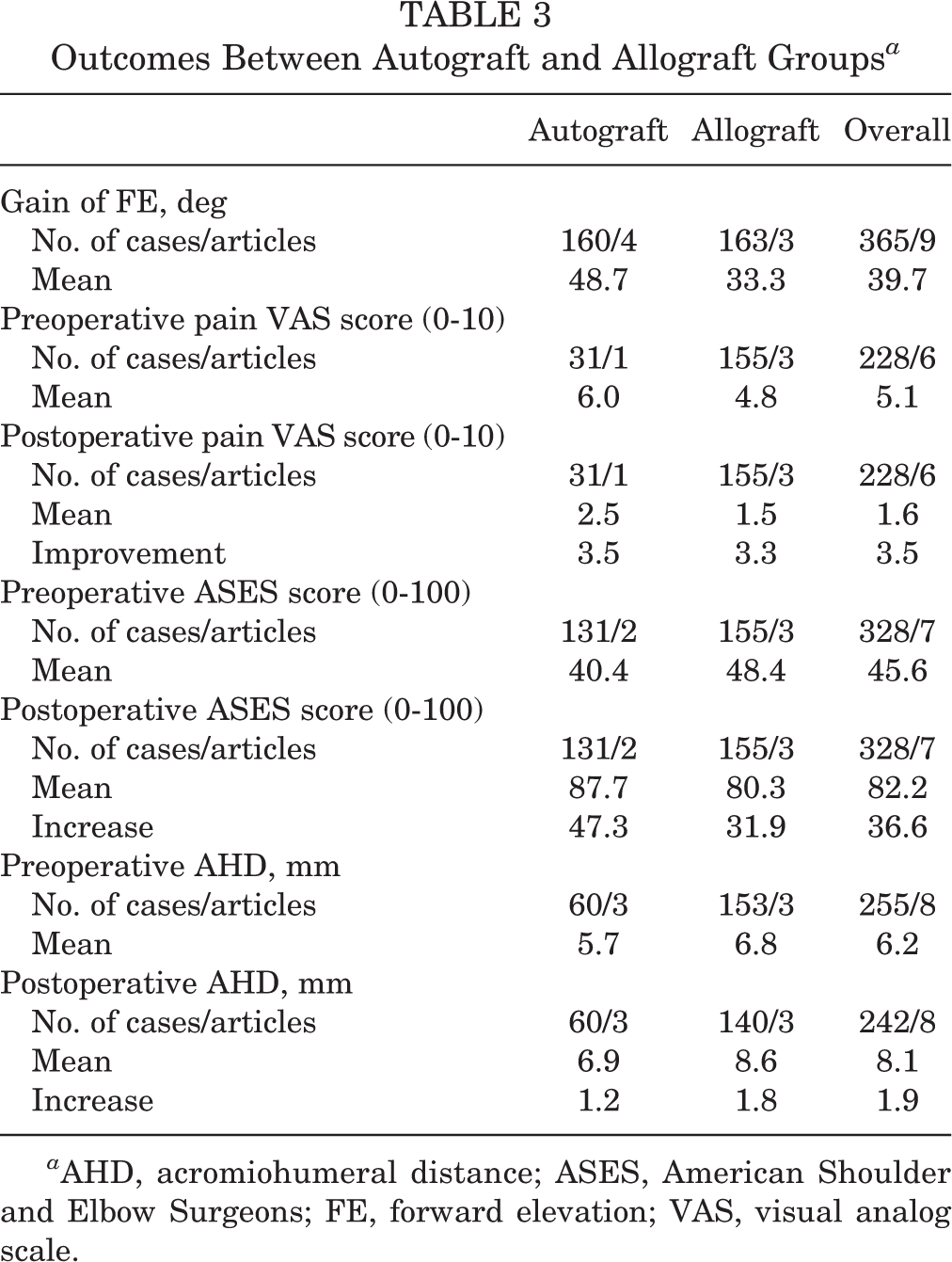
a AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Surgeons; FE, forward elevation; VAS, visual analog scale.
Complications and Reoperations Between Autograft and Allograft Groups a

a IST, infraspinatus; NR, not recorded; rTSA, reverse total shoulder arthroplasty; SCR, superior capsular reconstruction; SSC, subscapularis.
The number of graft tears was reported to be similar, with 16 cases (10.0%) and 17 cases (12.9%) for autografts and allografts, respectively. Complications other than graft tears occurred in 12 cases (7.5%) and 6 cases (3.9%) for autografts and allografts, respectively, and reoperations occurred in 5 cases (3.1%) and 14 cases (8.2%), respectively. Common reoperations were as follows: conversion to rTSA (10 cases from the allograft group), revision surgery of failed SCR (2 cases from the allograft group and 13 cases from the combined group), and debridement or lavage for postoperative infections (3 cases from the autograft group and 1 case from the allograft group). Other common complications are summarized in Table 4. There were 16 graft tears (10.0%) reported in the autograft group, but none were converted to rTSA. In the allograft group, graft tears were reported in 17 cases (12.9%), and conversion to rTSA was reported in 10 cases (7.6%).
Comparison Between Torn Graft and Intact Graft Groups
There were 2 studies 18,19 that analyzed the change in outcomes according to graft tears, as summarized in Table 5. Lim et al 19 showed no significant difference between the torn autograft and intact autograft groups in most of the outcomes except preoperative and postoperative AHD and preoperative VAS pain score. On the other hand, the study by Lee and Min 18 showed significant differences in results between the torn graft and intact graft groups in all measures except for internal rotation (IR) and external rotation (ER).
Comparison Between Torn Graft and Intact Graft Groups a

a Data are reported as mean ± SD unless otherwise indicated. AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FE, forward elevation; IR, internal rotation; NR, not recorded; VAS, visual analog scale.
b Statistically significant change (P < .05).
Evidence-Based Tendency
Each study was assessed for the risk of bias using the MINORS criteria. 38 The mean score of noncomparative studies was 11.2 ± 1.2. There were no comparative studies. The conference abstract was excluded from this methodological analysis because it was not possible to evaluate the risk of bias. Figure 4 shows the distribution of MINORS scores and the range considered as high-quality articles. All 9 studies except the conference abstract were considered as high-quality studies, exceeding 60% (≥10 points) of the total points, and their tendencies were analyzed. Both autografts and allografts significantly improved FE 7,8,19,21,32,33,35 and clinical outcomes, 7,8,12,19,21,32,33,35 as indicated by the VAS pain and ASES scores. Also, there was a tendency identified in 2 articles each that autografts increased IR 7,21 and allografts improved abduction (ABD). 32,33 Moreover, there were weak tendencies (1 study each) that autografts improved ABD 7 and allografts improved IR and ER 8 . There were conflicting tendencies about whether autografts improved ER and whether autografts or allografts increased the AHD.

Distribution of MINORS scores and the range considered as high-quality articles.
Discussion
We found 2 impressive results. First, although the graft tear rate seemed similar between the autograft and allograft groups, there was no conversion to rTSA in the autograft group. Most patients with graft tears underwent nonoperative treatment or revision surgery, with satisfactory clinical outcomes. We conducted an additional literature search to find reasons for this finding, but we could not find any evidence. As rTSA is also associated with other factors such as the preoperative Hamada classification, rotator cuff status, and age, further research is needed to figure out the cause of the finding and whether allografts independently increase the rate of conversion to rTSA.
The second finding was that there was a conflicting opinion about the clinical outcomes associated with graft tears. Lim et al 19 reported that 7 graft tears occurred in the medial row (with remnant tissue at the insertion site) and 2 graft tears occurred in the lateral row. On the other hand, Lee and Min 18 reported that 11 graft tears occurred at the humeral suture site and 2 graft tears occurred at the glenoid site. Most graft tears in the study by Lim et al 19 had remnant tissue at the insertion site, and the clinical outcomes were not related to the presence of graft tears, whereas the majority of graft tears in the study by Lee and Min 18 did not have remnant tissue, and the torn graft group showed worse outcomes than the intact graft group. This finding suggests that the presence of remnant tissue in the greater tuberosity (insertion site) may be a major factor in predicting clinical outcomes after graft tears. However, careful interpretation is necessary because the number of cases studied was small (31 shoulders for Lim et al, 36 shoulders for Lee and Min). Further studies are needed to classify the graft tear systematically and clarify the relationship between graft tears and clinical outcomes.
Hirahara et al 12 reported that a dermal allograft is advantageous for the acquisition of ROM because of its high elasticity compared with a tensor fasciae latae autograft. The result that allografts tended to improve FE, ABD, IR, and ER is consistent with the opinion of Hirahara et al. 12 However, autografts also tended to sufficiently improve FE, ABD, and IR. We assumed that the reason for this result was based on the findings of a biomechanical study by Mihata et al. 20 They reported that fascia lata allografts fully restored superior glenohumeral stability, whereas single-layered human dermal allografts partially restored superior glenohumeral stability. 20 Fascia lata and hamstring autografts with lower elasticity might act as a stable fulcrum of the glenohumeral joint, leading to improved ROM.
The essential surgical method of all studies included in this systematic analysis was SCR, but there were also a variety of additional procedures. There were differences in the treatment of the remnant biceps tendon (biceps tenotomy), suturing between the anterior or posterior rotator cuff and graft, acromioplasty, and graft fixation technique (single or double row). These factors may have affected the outcomes. The study by de Campos Azevedo et al 7 reported that SCR in combination with long head of the biceps tenotomy had a better outcome than SCR without tenotomy. On the other hand, they reported that anterior acromioplasty was not associated with the outcome, thus emphasizing the benefits of long head of the biceps tenotomy in SCR. According to a biomechanical study by Mihata et al, 26 acromioplasty has the potential to prevent graft friction and graft tears in SCR. Based on this finding, Lim et al 19 performed SCR and routine acromioplasty. They reported that an increased AHD and successful SCR were related to routine acromioplasty, which they recommended. 19
Another biomechanical study by Mihata et al 27 reported that posterior continuity of the graft and residual infraspinatus tendons via side-to-side suturing could restore superior stability of the shoulder but that anterior side-to-side suturing (anterior margin convergence) was not required. Lee and Min 18 suggested that it is important to restore posterior remnant tissue because there is a significant correlation between graft tears and discontinuity between the graft and posterior remnant tissue such as the infraspinatus tendon. The study by Hirahara et al 12 emphasized the importance of anterior side-to-side suturing as well as posterior side-to-side suturing to optimize graft tensioning. Considering that there are numerous fixation techniques alongside many additional procedures, appropriate procedures should be used depending on the patient’s condition.
A study of the thickness of fascia lata grafts by Mihata et al 25 reported that stability of a 8 mm–thick graft was superior compared with a 4 mm–thick graft. Most of the autograft studies 7,18,19,21 included in this review achieved a graft thickness of 5 to 8 mm and reported good results. Allograft studies, on the other hand, used various sizes of dermal allografts. The study by Hirahara et al 12 included 1 case using a 1.5 mm–thick graft and reported that a graft tear occurred in the case. The study by Yoon et al 40 included 1 case using a 2 mm–thick graft and reported that the AHD decreased and osteoarthritis progressed in that patient. Denard et al 8 used a 1-mm graft in 5 cases, a 2-mm graft in 2 cases, and a 3-mm graft in the rest. The 1 mm–thick graft showed a 40% success rate, while the 3 mm–thick graft showed better results. Based on this finding, Denard et al 8 proposed using 3 mm–thick allografts. Other studies 32,33 using only 3 mm–thick allografts also showed good results.
One of the most obvious disadvantages of autografts, donor site morbidity, is referred to in only 2 of the 4 articles. According to Mihata et al, 21 none of the patients complained of harvest site–related dysfunction, and only 1 patient complained of discomfort in the surrounding area. According to de Campos Azevedo et al, 7 16 of 22 patients felt discomfort at the donor site, but the surgical results compensated for such discomfort. Based on the available data, it is assumed that some patients may experience mild discomfort, but no serious complications occurred.
It is important to note that both the autograft and allograft groups had significantly better clinical outcomes compared with those before surgery. Descriptive analysis revealed that there were not only small differences but also large differences between the 2 groups. The statistical significance of differences between the 2 groups may be analyzed through a comparative study. If a subsequent comparative study yields no or little differences between the 2 groups, allografts, which have the advantage of no donor site morbidity, will be an attractive option for SCR graft selection. However, if there is a difference in outcomes between the 2 groups, it will be necessary to establish an appropriate indication for selecting an autograft versus an allograft, considering the cost-effectiveness, operation time, graft rejection and failure rate, and donor site morbidity.
To the best of our knowledge, this study is the first systematic review comparing outcomes after autograft and allograft use in SCR, and it has several limitations. First, we tried to conduct as comprehensive a search as possible, but we may have missed related articles. Also, because research on SCR is actively being carried out, the results may be different if further studies are added and analyzed. Second, the articles included in this study mainly reported early results, so it will be necessary to synthesize the results of long-term follow-up to be reported later. Third, SCR using a remnant biceps tendon as an autograft was recently reported but was not included in this systematic review. 5 In future comparative studies, this procedure should be considered. Fourth, operation time and cost-effectiveness are important factors to compare. In this review, none of the studies presented operation time or considered the cost of surgery. Fifth, we set somewhat arbitrary criteria because there were no clear criteria for high-quality studies. If these criteria had been more strict, none of the tendencies would have been identified. Finally, studies 8,32 in the allograft group did not fully assess the presence of retears. Therefore, retear rates of the allograft group might be underestimated. To obtain strong evidence on the comparison of results between autografts and allografts, level 1 and 2 studies should ultimately be conducted. Multicenter research may be necessary to obtain enough cases.
Conclusion
Both autografts and allografts improved clinical outcomes. Although the graft tear rate appeared similar between the autograft and allograft groups, the autograft group had no cases of conversion to rTSA. In addition, we found 3 evidence-based tendencies: (1) the tendency that both autografts and allografts significantly improved FE and clinical scores, (2) the tendency that autografts improved IR and allografts improved ABD, and (3) the weak tendency that autografts improved ABD and allografts improved IR and ER. Although it was not possible to compare the groups statistically, the differences in ASES scores might be clinically important and will need to be explored in future comparative studies.
Footnotes
Final revision submitted October 11, 2019; accepted November 19, 2019.
One or more of the authors declared the following potential conflict of interest or source of funding: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2018R1D1A1A02086025). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.