
Abstract
Background:
Meniscal allograft transplant requires precise matching of the size of the allograft with the dimensions of the recipient knee. Estimation of contralateral meniscal size on magnetic resonance imaging (MRI) has been considered the ideal method to measure menisci before transplant. We questioned whether a contralateral intact meniscus with meniscal injury in the opposite compartment could be used as a reference to determine allograft size. Our question was derived from knowledge of meniscal injury influencing structures of the opposite compartment of the knee, including the meniscus.
Purpose:
To compare meniscal dimensions between intact meniscus with meniscal injury in the opposite compartment and normal meniscus with a normal opposite compartment.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This observational, cross-sectional study was performed between 2016 and 2017. The control group consisted of 200 knees with normal medial and lateral menisci. The medial intact group consisted of 150 cases of medial intact meniscus with injured lateral meniscus, and the lateral intact group consisted of 150 cases of lateral intact meniscus with injured medial meniscus. All patients were male. Mean age, height, and weight did not differ among groups. We investigated meniscal dimensions on MRI, including anteroposterior and mediolateral lengths, distance between the anterior and posterior horns (AHPH distance), and widths and heights of the anterior and posterior horns and midbody.
Results:
Most medial meniscal dimensions were similar between the control and medial intact groups, but the AHPH distance was smaller in the medial intact group (P < .001). Likewise, most lateral meniscal dimensions were similar between the control and lateral intact groups, but the AHPH distance was smaller in the lateral intact group (P < .001).
Conclusion:
Most dimensions of the intact meniscus with meniscal injury in the opposite compartment were similar to those of the normal meniscus with normal opposite compartment. Measuring the dimensions of the contralateral intact meniscus with meniscal injury in the opposite compartment on MRI can be an appropriate method to determine meniscal allograft size.
Keywords
Meniscal allograft transplant (MAT) has become a common treatment for patients with inadequate posttraumatic or postsurgical meniscus. 4 Success of the procedure depends on accurate measurements to precisely match the dimensions of the donor and recipient menisci. 8,14,16 Numerous measurement techniques to determine meniscal size have been introduced based on plain radiographs, 3-dimensional (3D) computed tomography, anthropometric data, and magnetic resonance imaging (MRI). 7,8 Among these techniques, measuring the dimensions of the in vivo contralateral meniscus on MRI is generally considered to be the most accurate and reliable method. 8
At our institution, measurement of the contralateral meniscus on MRI has been used for meniscal sizing before MAT. Occasionally, we have observed a contralateral intact meniscus with an injured meniscus in the opposite tibiofemoral compartment on MRI. In this situation, we have wondered whether the dimensions of the contralateral intact meniscus with meniscal injury in the opposite compartment provide an appropriate reference for meniscal allograft sizing.
Previous studies have reported that meniscal injury in one compartment can change the biomechanics of the opposite compartment of the knee. Posterior root tear of the medial meniscus can change the overall knee kinematics, including tibial external rotation and lateral translation. 1 Several finite element analyses and cadaveric studies 1,2,10 have shown that an abnormal injured meniscal state, including lateral meniscus posterior root tear or medial meniscus longitudinal tear, can influence contact pressure or shear stress on the structure of the opposite compartment of the knee. Accordingly, it is possible that the dimensions of the intact meniscus with meniscal injury in the opposite compartment differ from those of the normal meniscus with a normal opposite compartment, even if there is no injury. To our knowledge, no previous studies have addressed this issue.
In the present study, we compared meniscal dimensions between intact meniscus with meniscal injury in the opposite compartment and normal meniscus with a normal opposite compartment. We hypothesized that meniscal injury might affect the dimensions of the intact meniscus in the opposite compartment of the knee.
Methods
Patients
This observational, cross-sectional study was conducted at our hospital between 2016 and 2017. During this period, 4161 MRI scans of the knee were performed. Inclusion criteria were male patients between the ages of 20 and 45 years. Exclusion criteria were skeletal immaturity, history of knee surgery, ligament injury, discoid meniscus, and tibiofemoral joint arthritis. To evaluate normal meniscal dimensions, we identified subjects who underwent knee MRI with normal medial and lateral meniscus (control group). MRI examination was performed on these patients for various reasons: nonspecific knee pain without an apparent cause, simple contusion, symptomatic plica, patellofemoral pain syndrome, and patellar chondromalacia. None of the patients had any pathologic signal intensity suggesting meniscal degeneration or tear in either meniscus. A total of 200 knees were included in the control group.
We also reviewed the MRI findings of patients with intact menisci with meniscal injury in the opposite compartment. In the present study, meniscal injury was defined as a meniscus with a root tear or severe longitudinal (bucket-handle) tear; these lesions have clear effects on the function of the meniscus and may affect the structures of the opposite tibiofemoral compartment. 1,2,10 An intact meniscus had no pathologic findings on MRI. There were 150 cases of medial intact meniscus with injured lateral meniscus (medial intact group) and 150 cases of lateral intact meniscus with injured medial meniscus (lateral intact group).
This study was approved by an institutional review board. Informed consent was obtained from all patients before commencing the study.
MRI Measurement
MRIs were performed using a 3.0-T system (Achieva; Philips) with a specific 8-channel SENSE-Knee coil. Images were obtained with the knee in a neutral position. Proton density (PD)–weighted fat-suppression axial, T2-weighted spin-echo sagittal, PD-weighted spin-echo sagittal, and PD-weighted fat-suppression coronal MRI scans were obtained routinely in all knee examinations at our hospital. An additional PD or T2 fat-suppression axial sequence (repletion time/echo time, 4500/20 ms; field of view, 160 × 160 mm; matrix size, 320 × 309 pixels; section thickness, 3 mm; intersection gap, 0 mm) was also obtained. This axial image was directed to the femorotibial joint space to achieve the best image of the long axis of the meniscus in the longitudinal plane, parallel to the tibial plateau; the axial image encompassed nearly all of the meniscal root insertion and the borders of the anterior and posterior horns and the midbody of the medial and lateral meniscus.
Measurements were performed with these images by use of a picture archiving and communication system (PACS; Infinitt Healthcare) after digital transfer. Measurements were performed on a 61-cm (24-inch) monitor (SyncMaster 2494HMN; Samsung) in portrait mode using PACS software. The software was capable of detecting a minimum difference of 0.1 mm in length. 9
On the additional axial image, we evaluated anteroposterior (AP) length, mediolateral (ML) length, and distance between the anterior and posterior horns (AHPH distance) (Figure 1). The AP length was defined as the distance between the most anterior point of the anterior horn and the most posterior point of the posterior horn. 8,12 To determine the ML length, a reference line was drawn to connect the most central point of the anterior and posterior horn insertion points; ML length was defined as the distance from the reference line to the most outer margin. 8,12 The AHPH distance was defined as the distance between the center points of root insertion of the anterior and posterior horns. 17
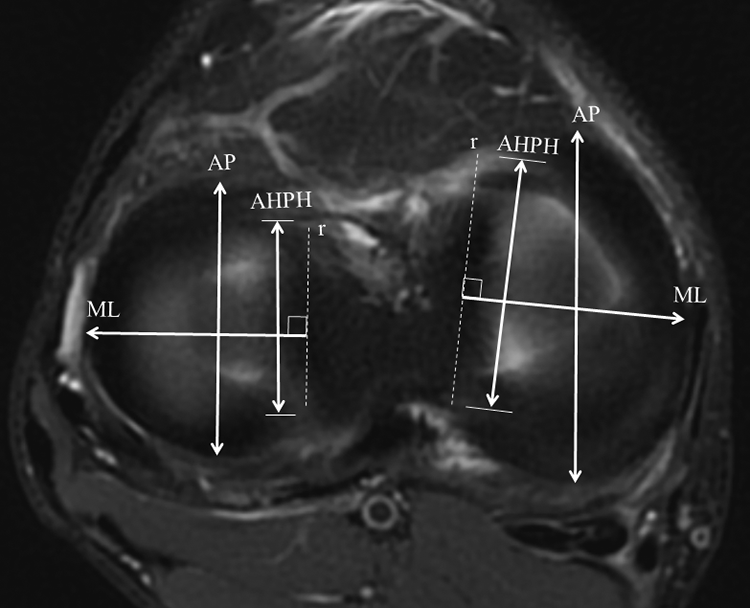
Measurement of anteroposterior and mediolateral lengths and the distance between the anterior and posterior horns (AHPH distance) in normal medial and lateral menisci. Anteroposterior (AP) length was defined as the distance between the most anterior point of the anterior horn and the most posterior point of the posterior horn. Mediolateral (ML) length was defined as the distance from the reference line (r) to the most outer margin. The reference line (r) was drawn to connect the most central point of the anterior and posterior horn insertions. The distance between the anterior and posterior horns was defined as the distance between the center points of root insertion of the anterior and posterior horns.
The respective widths and heights of the anterior and posterior horns of each meniscus were evaluated on sagittal MRI scans and were measured at the most anterior and posterior points of the meniscus (Figure 2). 3,6,12 The width and height of the midbody of each meniscus were evaluated on coronal MRI scans; those of the medial and lateral meniscus were measured at the most medial and lateral points on the meniscus, respectively (Figure 3). 3,6,12

Measurement of respective widths and heights of the anterior and posterior horns in (A) normal medial meniscus and (B) lateral meniscus. The widths and heights of the anterior and posterior horns of the meniscus were evaluated on sagittal MRI and were measured at the most anterior and posterior points of the meniscus, respectively. AH, height of anterior horn; AW, width of anterior horn; PH, height of posterior horn; PW, width of posterior horn.

Measurement of width and height of the midbody in normal medial and lateral menisci. The width and height of the midbody were evaluated on coronal MRI; those of the medial and lateral meniscus were measured at the most medial and lateral points on the meniscus, respectively. MH, height of midbody; MW, width of midbody.
To minimize observation bias, 2 independent investigators (H.S.L., C.H.P.) performed all measurements and repeated them after an interval of 2 weeks. The intra- and interobserver reliabilities for all measurements were assessed with the intraclass correlation coefficient, the values of which were all greater than 0.8 (Table 1). The mean values of the measurements, which were repeatedly performed by a single investigator who had more clinical experience than the other, were used in the analyses.
Intraclass Correlation Coefficient Values for Intra- and Interobserver Reliabilities a

a The control group contained knees with normal medial and lateral menisci; the medial intact group contained knees with intact medial meniscus with injured lateral meniscus; the lateral intact group contained knees with intact lateral meniscus with injured medial meniscus. AHPH distance, distance between the anterior and posterior horns; Intra, intraobserver reliabilities; Inter, interobserver reliabilities.
Statistical Analysis
Demographics including age, height, and weight were compared among control, medial intact, and lateral intact groups (analysis of variance). The dimensions of the medial meniscus were compared between the control and medial intact groups (independent t test). The dimensions of the lateral meniscus were compared between the control and lateral intact groups (independent t test). Statistical analyses were performed with SPSS Version 18.0 (SPSS Inc), and a P < .05 was considered statistically significant.
Power analyses using significance at an alpha of 0.05 were performed to determine whether the sample had sufficient power to detect significant differences. A power greater than 80% was considered sufficient, and all of the significantly different variables met this criterion.
Results
Patient demographics are presented in Table 2. Variables known to affect meniscal dimensions, including age, weight, and height, did not differ among the 3 groups. 3,15,16
Patient Demographics a
a Data are expressed as mean ± standard deviation. The control group contained knees with normal medial and lateral meniscus; the medial intact group contained knees with intact medial meniscus with injured lateral meniscus; the lateral intact group contained knees with intact lateral meniscus with injured medial meniscus.
Most medial meniscal dimensions were similar between the control and medial intact groups; however, the AHPH distance was significantly smaller in the medial intact group (P < .001) (Table 3). Likewise, most lateral meniscal dimensions between the control and lateral intact groups were similar, but the AHPH distance was significantly smaller in the lateral intact group (P < .001) (Table 3).
Meniscal Dimensions a

a Data are expressed in millimeters as mean ± standard deviation. The control group contained knees with normal medial and lateral meniscus; the medial intact group contained knees with intact medial meniscus with injured lateral meniscus; the lateral intact group contained knees with intact lateral meniscus with injured medial meniscus. Boldface P values indicate statistically significant differences between groups (P < .05). AHPH distance, distance between the anterior and posterior horns.
Discussion
The most important finding of this study was that most meniscal dimensions were similar between the control and intact meniscus groups, although the AHPH distance differed significantly between groups.
It has been reported that meniscal injury in 1 compartment can change the biomechanics of the opposite compartment. In a cadaveric study, Allaire et al 1 reported a significant increase in external rotation and lateral tibial translation (2.98 and 0.84 mm, respectively) in association with posterior root tear compared with a normal knee without injury. A finite element analysis by Li et al 10 revealed that a longitudinal tear of the medial meniscus increases compression and shear stress of the intact lateral meniscus. Bao et al 2 showed that a complete posterior lateral meniscal root tear increases peak contact pressure of the opposite medial compartment. Thus, we hypothesized that the dimensions of an intact meniscus, with meniscal injury in the opposite compartment, would differ from those of a normal meniscus with a normal opposite compartment. However, the results differed from our expectations: Most meniscal dimensions were similar between the control and intact medial or lateral meniscus groups.
In particular, clinically relevant dimensions of the meniscus did not differ between the control and intact groups. For example, no significant differences were found in AP and ML lengths between groups. The AP and ML lengths are clinically important parameters; most physicians base the prediction of meniscal size on the AP and ML lengths before allograft transplant. 8,12,14 Furthermore, no difference was found in meniscal height, which influences the contact pressure of the articular surface. 12 Change in environment due to meniscal injury in the opposite compartment may not be large enough to cause serious changes in clinically relevant dimensions of the intact meniscus. The presence of a joint capsule could also contribute to dimensional similarity because the capsule maintains the boundary of the meniscus and prevents changes in boundary shape. 11
Only the AHPH distance differed significantly between the control and intact groups. As previously described, meniscal injury can increase pressure and stress on the structures in the opposite compartment of the knee. 2,10 We expected a greater AHPH distance in the intact groups because the meniscal interhorn distance increases significantly under loads compared with under no load. 11 However, the distances were smaller in the intact groups compared with the control group. Although we cannot explain the exact mechanism behind this finding, we assume that the smaller AHPH distance in the intact groups resulted from a reduction in the weightbearing function of the knee with meniscal injury due to pain; the meniscal dimensions might be adapted to the reduced weightbearing state, which decreased the load on the meniscus and thus the AHPH distance. 13 A more sophisticated biomechanical study will be required to determine the exact mechanism for this finding.
MAT requires precise matching of the size of the allograft with the dimensions of the recipient knee to restore meniscal function. It has been reported that size discrepancies of less than 10% are tolerated after transplant. 8,12 A number of previous studies have tried to establish an accurate method to measure the size of the allograft meniscus. Until now, estimation of contralateral meniscal size on MRI has been considered the ideal method to measure menisci before transplant. 8,14 We questioned whether a contralateral meniscus with meniscal injury in the opposite compartment (such as a meniscal root tear or bucket-handle tear) could be used as a reference to determine the meniscal allograft size, because meniscal injury may influence the structures, including the meniscus, of the opposite compartment of the knee. Our results indicate that measurement of the contralateral meniscus with an injured meniscus in the opposite compartment can be used as an appropriate method to determine allograft size without major clinical problems. However, there may be minor differences in meniscal dimensions in an “imperfect” situation. It will be expected that more precise determination of allograft size and shape considering these small differences may lead to better clinical outcomes after MAT.
The present study has several limitations. First, we could not directly compare the dimensions of the normal meniscus with normal opposite compartment versus those of intact contralateral meniscus with meniscal injury in the opposite meniscus in paired knees within the same person. The number of samples satisfying this condition would have been too small to conduct the study. However, no significant differences were found in factors influencing meniscal size, such as sex, height, and weight, between the control and intact groups. In addition, it has been reported that meniscal dimensions are asymmetrical even between paired knees in the same patient. 5 Second, the measurements on MRI scans could have been inaccurate due to the MRI protocol, the measurement technique itself, or both. However, our MRI protocol and measurement techniques have been validated in previous studies. 8,12 In addition, the orthopaedic surgeons who measured the meniscal dimensions had more than 10 years of clinical experience with knee surgery, and the intra- and interobserver reliabilities of the measurements were satisfactory. Third, we limited our study of meniscal injury to just 2 conditions: root tear and bucket-handle tear. We might have obtained different results if we had considered other types of injury, such as horizontal or radial tear. Fourth, all of the patients enrolled in the present study were Asian males. The characteristics of our study groups should be taken into consideration when extrapolating our findings to females or other populations. Fifth, although our sample size was adequate, a larger sample would have increased the likelihood of finding significant differences. Future studies with larger populations will be necessary to confirm our findings.
Conclusion
Most dimensions of the intact meniscus with meniscal injury in the opposite compartment were similar to those of normal meniscus with a normal opposite compartment. Measurement of a contralateral meniscus with meniscal injury in the opposite compartment on MRI can be considered an appropriate method to determine allograft size before MAT. A more sophisticated biomechanical study will be required to determine the exact mechanism of differences in the AHPH distance.
Footnotes
Final revision submitted October 10, 2019; accepted November 19, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Institutional Review Board of Kyung Hee University Hospital (KHUH 2019-06-015-003).