
Abstract
Background:
Achilles tendinopathy is a frequent sports injury, and extracorporeal shock wave therapy (ESWT) has been proposed as a treatment.
Purpose:
To compare outcomes between ESWT and other nonsurgical intervention (including sham shock wave therapy) in Achilles tendinopathy patients.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
We included 5 randomized controlled trials and 3 case-control studies published between 2005 and 2018. We analyzed pain scores and other outcomes that were reported in more than 3 of the 8 studies.
Results:
ESWT was associated with significantly better scores than comparison therapy on the visual analog scale for pain (P < .01), American Orthopaedic Foot & Ankle Society scale (P = .01), Likert scale for satisfaction (P = .03), Roles and Maudsley scale (P < .01), Victorian Institute of Sports Assessment–Achilles questionnaire (P < .01), and numerical rating scale (P = .02). The 2 patient groups did not differ significantly in tenderness (P = .34) or pain threshold (P = .24). Subgroup analysis showed that ESWT led to better VAS pain scores than comparison treatments at both low-energy level (0.06-0.11 mJ/mm2) and medium-energy level (0.12-0.25 mJ/mm2) and at both shorter (<6 months) and longer (≥6 months) follow-up.
Conclusion:
ESWT improves pain and functional outcomes in patients with Achilles tendinopathy. Further research is needed to determine the optimal energy level.
Achilles tendinopathy is a frequent sports injury, especially in track and field athletes, accounting for 5% to 18% of all injuries in runners. 1 It most likely occurs when there is a sudden increase in the amount or intensity of leg activities. Because Achilles tendinopathy involves lesions in the Achilles tendon, enthesis organ, and surrounding peritendinous structures, patients experience pain to touch or during movement. Some patients may have trouble walking or running. 4
Extracorporeal shock wave therapy (ESWT), proposed as a nonsurgical alternative treatment for Achilles tendinopathy, has been widely used for several orthopaedic conditions, such as lateral epicondylitis and calcific rotator cuff tendinosis. 8,14 Based on the results of outcome measures to assess pain and function, one systematic review suggested that among patients with midportion Achilles tendinopathy, ESWT was comparable with eccentric training and superior to a wait-and-see approach at 4 months. 2 That review could not determine whether efficacy persisted beyond 12 months because of the small sample size. A systematic review based on only randomized controlled trials (RCTs) concluded that ESWT can improve pain and functional outcomes in Achilles tendinopathy patients for a minimum of 3 months. 1 This literature therefore provides evidence that ESWT should be considered before surgery when traditional treatments fail.
However, one of the problems with interpreting this evidence is the heterogeneity in instruments used to assess pain and functional outcomes after ESWT. These instruments include the American Orthopaedic Foot & Ankle Society score (AOFAS), visual analog scale (VAS) for pain, Victorian Institute of Sports Assessment–Achilles questionnaire (VISA-A), numerical rating scale (NRS), and the Roles and Maudsley scale. 2,7 A second problem is that many previous studies were relatively small and not based on a randomized controlled design. A third problem is that the effects of different ESWT energy levels on different types of Achilles tendinopathy have yet to be systematically reviewed.
The present meta-analysis addresses these questions and includes some RCTs and noncontrolled comparative studies published since the latest systematic reviews on ESWT.
Methods
Literature Search Strategy
MEDLINE (Ovid), EMBASE (Ovid), PubMed, and the Cochrane library (Central) were searched for relevant studies from 2005 to 2018. We used a combination of keywords and subject headings, including extracorporeal shockwave therapy (extracorporeal shockwave therapies, shockwave therapies, extracorporeal, shockwave therapy, extracorporeal, therapy, extracorporeal shockwave, shock wave therapy, shock wave therapies, therapy, shock wave, extracorporeal shock wave therapy, extracorporeal high-intensity focused ultrasound therapy, extracorporeal high intensity focused ultrasound therapy, HIFU therapy, HIFU therapies, therapy, HIFU, high-intensity focused ultrasound therapy, high intensity focused ultrasound therapy) and Achilles tendon (tendon, Achilles, calcaneal tendon, calcaneal tendons, tendon, calcaneal, tendons, calcaneal, tendo calcaneus). References in previous systematic reviews were searched for potentially relevant studies. The World Health Organization International Clinical Trials Registry Platform (http://apps.who.int/trialsearch/) and Clinical Trials Registry (http://clinicaltrials.gov) were searched for ongoing or completed but unpublished trials.
Study Selection
To be included in our review and meta-analysis, studies had to (1) have a controlled design, randomized or not; (2) involve patients with Achilles tendinopathy of any age treated with ESWT or, as the control arm, traditional nonsurgical treatments or sham ESWT; (3) evaluate pain and functional outcomes using any accepted instrument; and (4) be written in English. Studies were excluded if they involved animals or cadavers, were reviews or case reports, or did not report treatment or clinical outcomes.
Data Extraction
Two of the authors (Y.F., Z.F.) independently extracted publication information, study design, study population, interventions, and outcome measures from each included study. When 2 studies were found using the same group of participants, both studies were included only when different outcome measures were used. When studies involved the same group of participants and the same outcome measures, only the study with the longest follow-up was included.
Assessment of Study Quality
The quality of each article was assessed independently by 2 authors (Y.F., Z.F.) using the Cochrane risk of bias assessment tool in the case of RCTs or the Newcastle-Ottawa Scale in the case of nonrandomized comparative studies.
Meta-analysis
Data on pain and functional outcomes were meta-analyzed if they were reported in more than 3 of the included studies. These measures included AOFAS, Likert scale for satisfaction, Roles and Maudsley score, NRS, tenderness, VAS for pain, and VISA-A. VAS scores were also meta-analyzed for short- or long-term follow-up. In all meta-analyses, a random-effects model was used.
Test for Heterogeneity
Heterogeneity was tested with respect to the types of Achilles tendinopathy (insertional vs noninsertional), design of the study (randomized controlled vs non–randomized controlled), type of shock wave therapy device (electromagnetic vs radial vs multiple), frequency of the intervention (number of shock wave impulses, number of applications, and application intervals), outcomes, and duration of follow-up (<6 vs ≥6 months). A subgroup analysis was also performed based on energy level used in ESWT (low, 0.06-0.11 mJ/mm2; medium, 0.12-0.25 mJ/mm2; or high, 0.26-0.39 mJ/mm2). 3
Sensitivity Analysis
Sensitivity analysis was performed by repeating meta-analyses after removing each study one at a time.
Statistical Analysis
Data in the meta-analysis were expressed as mean differences (MDs) and 95% CIs. Heterogeneity was assessed using the I2 statistic: 25% was considered low; 50%, moderate; and 75%, high. Forest plots were used to show the outcome, pooled estimate of effect, and overall summary effect of each study. Differences were considered significant when the P value was less than .05. Statistical analyses were performed using RevMan 5.3 (Cochrane Collaboration).
Results
A total of 766 related studies were identified: 465 studies in PubMed, 112 studies in EMBASE, and 189 studies in MEDLINE (Figure 1). Duplicates (n = 299) were removed. After we reviewed titles, abstracts, and full text of the remaining 467 studies, 8 were included; these involved 442 cases of midportion Achilles tendinopathy, of which half received ESWT and the other half received a comparison treatment, including sham ESWT (2 studies), eccentric loading (4 studies), traditional nonoperative measures (2 studies), or wait-and-see (1 study) (Table 1).

Flow diagram showing literature selection.
Summary of Included Studies a

a Dashes indicate not reported. AOFAS, American Orthopaedic Foot & Ankle Society; ESWT, extracorporeal shock wave therapy; fSWT, focused shock wave therapy; NRS, Numerical Rating Scale; NSAID, nonsteroidal anti-inflammatory drug; RCT, randomized controlled trial; RM, Roles and Maudsley scale; rSWT, radial shock wave therapy; VAS, visual analog scale; VISA-A, Victorian Institute of Sports Assessment–Achilles questionnaire.
Meta-analysis
In measures where lower scores indicate more favorable outcomes (VAS pain, Roles and Maudsley, NRS, and Likert scores), ESWT was associated with lower VAS scores than comparison treatment (MD, –2.14; 95% CI, –2.73 to –1.56; P < .001; I2 = 88%) (Figure 2) 10,12,15,16 as well as with lower Roles and Maudsley score (MD, –2.80; 95% CI, –3.30 to –2.30; P < .001; I2 = 69%) (Figure 3) based only on 2 studies. 5,6 ESWT was also associated with lower NRS score (MD, –0.58; 95% CI, –1.07 to –0.08; P = .02; I2 = 69%) (Figure 4) 10 –12 and lower Likert scale score (MD, −0.46; 95% CI –0.87 to –0.05; P = .03; I2 = 55%) (Figure 5). 10 –12

Forest plot of visual analog scale scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of Roles and Maudsley scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of numerical rating scale scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of Likert scale scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.
In measures where higher scores indicate more favorable outcomes, ESWT was associated with higher VISA-A score than comparison treatment (MD, 1.53; 95% CI, 0.69 to 2.37; P = .0003; I2 = 92%) (Figure 6) 10 –12,16 and with higher AOFAS score (MD, 1.35; 95% CI, 0.28 to 2.41; P = .01; I2 = 93%) (Figure 7). 9,15,16 The 2 groups did not differ significantly in tenderness score (MD, –0.25; 95% CI, –0.77 to 0.27; P = .34; I2 = 61%) (Figure 8) 11,13 or pain threshold (MD, 0.45; 95% CI, –0.30 to 1.20; P = .24; I2 = 81%) (Figure 9). 10,12

Forest plot of Victorian Institute of Sports Assessment–Achilles questionnaire in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of American Orthopaedic Foot and Ankle Society scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of tenderness scores in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.

Forest plot of pain threshold in patients who received extracorporeal shock wave therapy (SWT) or comparison treatment. IV, inverse variance methods.
Among patients who received ESWT, VAS pain scores were not significantly different for follow-up shorter or longer than 6 months (MD, 0.01; 95% CI, –0.66 to 0.67; P = .99; I2 = 80%) (Figure 10). 5,6,16

Forest plot of visual analog scale scores after short- or long-term follow-up in patients who received extracorporeal shock wave therapy. IV, inverse variance methods.
A total of 3 RCTs reported that all patients who underwent ESWT experienced transient reddening of the skin. 10 –12 Further, 2 other studies reported individual complications, the incidence of which was similar between ESWT and comparison treatment (MD, 9.67; 95% CI, 1.19 to 78.93; P = .03; I2 = 0%) (Figure 11). 5,6 This lack of difference may be a reflection of the small samples in the 2 studies.

Forest plot of complications after short- or long-term follow-up in patients who received extracorporeal shock wave therapy (ESWT). M-H, Mantel-Haenszel.
Sensitivity Analysis
Removing the 2007 study by Rompe et al 12 reduced heterogeneity in pain threshold, NRS score, Likert scale score, and tenderness score. Removing the study by Vahdatpour et al 15 reduced heterogeneity in VAS score. Removing the study by Wei et al 16 reduced heterogeneity in AOFAS score. Removing the other studies did not alter heterogeneity in any of the outcomes.
Subgroup Analyses
Because of substantial heterogeneity in pain and functional outcomes, we performed subgroup analyses based on type of Achilles tendinopathy, study design, length of follow-up, and energy level of ESWT. VAS heterogeneity depended on the type of Achilles tendinopathy (insertional: 95% CI, –2.66 to –2.10; I2 = 0%; noninsertional: 95% CI, –3.79 to –2.90; I2 = 7%), energy of ESWT (medium: 95% CI, –2.76 to –1.27; I2 = 91%; low: 95% CI, –2.94 to −2.07; I2 = 0%), and study design (RCT: 95% CI, –0.90 to −0.04; I2 = 0%; case-control: 95% CI, –3.05 to –2.35; I2 = 54%). However, VAS score did not differ significantly between short- or long-term follow-up (<6 vs ≥6 months; P = .26) (Table 2).
Subgroup Analysis Based on VAS Score a

a AT, Achilles tendinopathy; IV, inverse variance methods; RCT, randomized controlled trial; VAS, visual analog scale.
Heterogeneity in VISA-A and AOFAS scores depended on length of follow-up, type of Achilles tendinopathy, ESWT energy level, and study design (P < .05) (Tables 3 and 4). In all subgroups, heterogeneity remained high for these outcomes.
Subgroup Analysis Based on AOFAS Score a

a AOFAS, American Orthopaedic Foot and Ankle Society; IV, inverse variance methods; RCT, randomized controlled trial.
Subgroup Analysis Based on VISA-A Score a
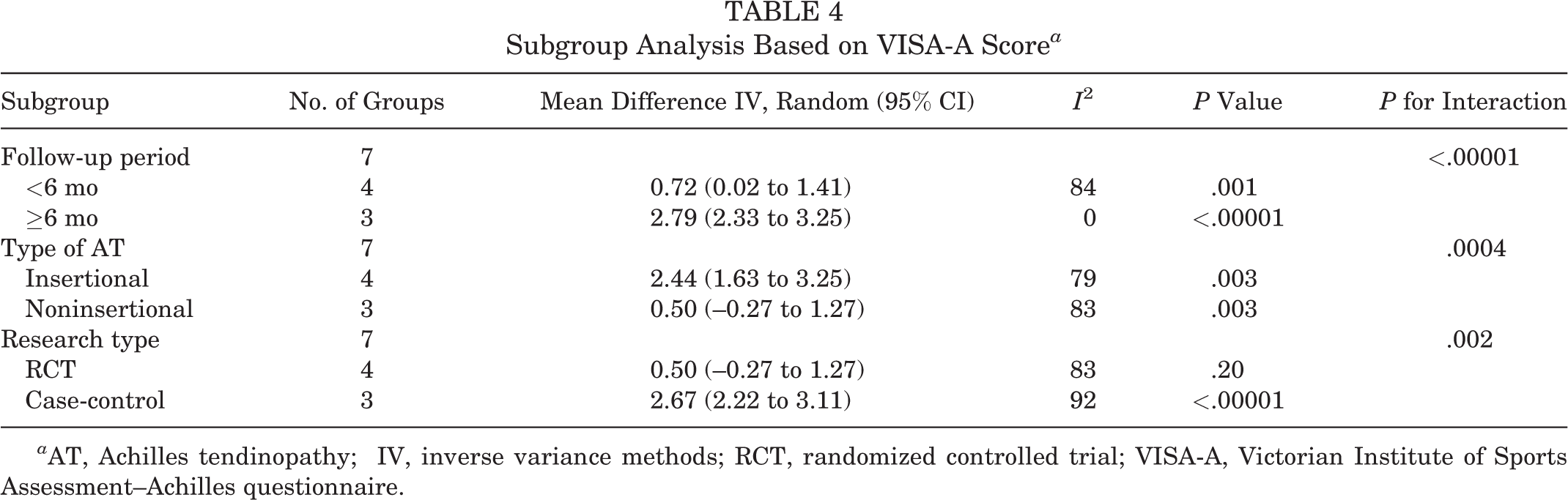
a AT, Achilles tendinopathy; IV, inverse variance methods; RCT, randomized controlled trial; VISA-A, Victorian Institute of Sports Assessment–Achilles questionnaire.
Quality Assessment
We found that 4 of the 5 RCTs had low risk of selection bias, except the study by Vahdatpour et al, 15 which had unclear selection bias. The studies by Rompe et al 10 –12 had high risk of performance bias. In addition, 2 of the studies by Rompe et al 10,11 had high risk of detection bias. All studies provided detailed data on demographics, pain, and functional outcomes. Rasmussen et al, 9 Rompe et al, 10 and Vahdatpour et al 15 did not provide sufficient information for assessing reporting bias. No study assessed possible contradictory factors (Figures 12 and 13).

Graphic assessment of risk of bias.

Summary of risk of bias.
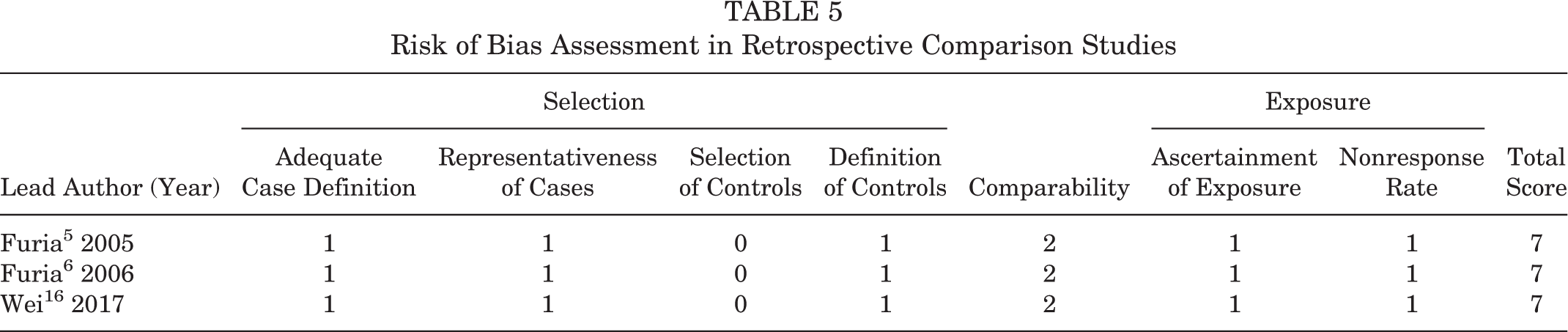
All 3 case-control studies 5,6,16 scored 5 or higher on the Newcastle-Ottawa Scale, indicating low risk of bias (Table 5).
Risk of Bias Assessment in Retrospective Comparison Studies
Discussion
The principal finding of this study was that patients who received ESWT for Achilles tendinopathy had significantly better pain and functional outcomes than patients who received other treatments, including sham ESWT, eccentric training, and other traditional treatments. This finding is consistent with those of previous systematic reviews on the effectiveness of ESWT on Achilles tendinopathies and on other orthopaedic diseases, including tennis elbow, patellar tendinopathies, and chronic proximal plantar fasciitis. 7 To the best of our knowledge, this is the first meta-analysis to conduct extensive subgroup analyses on the effects of ESWT on Achilles tendinopathies.
Our subgroup analyses showed that ESWT led to better VAS pain scores than other traditional nonoperative procedures against insertional and midportion Achilles tendinopathy. Our results are largely consistent with a smaller systematic review in which the authors found that ESWT was superior to eccentric training against insertional Achilles tendinopathy, comparable with eccentric training against midportion tendinopathy, and superior to the wait-and-see approach against midportion tendinopathy. 7
We found that ESWT led to better VAS pain scores than comparison treatments at both shorter (<6 months) and longer (≥6 months) follow-up. This confirms and extends previous analyses which concluded that ESWT can lead to better clinical outcomes than other nonsurgical treatments for follow-up of at least 3 months 1 and up to 12 months. 2 However, the persistence of therapeutic effects from ESWT may depend on the type of Achilles tendinopathy (insertional or noninsertional) and the energy level, which should be investigated in future studies.
Indeed, some studies have already demonstrated how the energy level in ESWT can affect outcomes: In 1 study, low-energy ESWT had short-term analgesic effects but aggravated symptoms in the long term. 13 We found that medium-energy ESWT (0.12-0.25 mJ/mm2) was comparable with low-energy ESWT (0.06-0.11 mJ/mm2) in improving pain VAS scores. Further work is needed to determine whether the energy levels differ in adverse effects. We noted that only 3 studies in our review used high-energy ESWT, probably because of the high risk of tissue damage.
This study has limitations. First, heterogeneity was high, which may make the results less reliable. Second, the small sample sizes in many studies may also make the results less reliable, especially in our subgroup analyses of follow-up duration and energy level. Indeed, small sample size prevented us from performing subgroup analysis based on treatment duration, which ranged from 4 to 12 weeks.
Conclusion
ESWT can lead to lower pain and better functional outcomes for patients with Achilles tendinopathy than other nonsurgical treatments.
Footnotes
Final revision submitted October 22, 2019; accepted October 23, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by National Natural Science Foundation of China (81972123, 31741046); Fundamental Research Funds for the Central Universities (2015SCU04A40); the Innovative Spark Project of Sichuan University (2018SCUH0034); 1·3·5 Project for Disciplines of Excellence–Clinical Research Incubation Project, West China Hospital, Sichuan University (2019HXFH039); and Research Project for Sichuan Provincial Health and Family Planning Commission (18ZD017). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.