
Abstract
Background:
There is an important gap in knowledge about the effectiveness of nonoperative treatment (exercise) for patients with traumatic primary and recurrent anterior shoulder dislocations (ASDs).
Purpose/Hypothesis:
The purpose of this study was to assess the efficacy and safety of physical therapist–supervised, shoulder instability neuromuscular exercise (SINEX) versus self-managed, home-based, standard care shoulder exercise (HOMEX) in patients with traumatic ASDs. The hypothesis was that SINEX would have a larger effect and fewer adverse events compared with HOMEX.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
A total of 56 participants with radiographically verified, trauma-initiated primary or recurrent ASDs and self-reported decreased shoulder function were randomized to 12 weeks of either SINEX or HOMEX. The SINEX program consisted of 7 exercises, individually progressing from basic (2 × 20 repetitions each day) to elite (2 × 10 repetitions, 3 times weekly). The HOMEX program included 5 shoulder exercises performed 3 times weekly (2 × 10 repetitions). The primary outcome was the Western Ontario Shoulder Instability Index (WOSI) score, ranging from 0 (best possible) to 2100. The between-group minimal clinically important difference at 12 weeks was 250 points. Secondary outcomes included WOSI subdomain scores, patient-reported ratings of kinesiophobia and pain, objective shoulder function, patient satisfaction, and number of adverse events.
Results:
The between-group mean difference in the WOSI total score at 12 weeks significantly favored SINEX over HOMEX (–228.1 [95% CI, –430.5 to –25.6]). SINEX was furthermore superior to HOMEX in most of the secondary outcomes (3/4 subdomains of the WOSI and pain level during the past 7 days as well as clinical signs of anterior shoulder instability). Also, although not statistically significant, less than half the proportion of the SINEX patients compared with the HOMEX patients (3/27 [11%] vs 6/24 [25%], respectively; P = .204) underwent or were referred for shoulder stabilizing surgery. Satisfaction with both exercise programs was high, and no serious adverse events were reported.
Conclusion:
Neuromuscular shoulder exercise (SINEX) was superior to standard care exercise (HOMEX) in patients with traumatic ASDs. Further long-term follow-ups on treatment effects are needed.
Registration:
NCT02371928 (ClinicalTrials.gov identifier).
A traumatic anterior shoulder dislocation (ASD) is a common athletic injury among young, active patients. 34 The annual incidence of primary traumatic ASDs is between 11.2 and 26.2 per 100,000 people. 30,32,52 Patients with primary traumatic ASDs are prone to recurrent ASDs because of lesions of the glenoid labrum, an important stabilizer of the shoulder. 31,42 This may lead to recurrent ASDs and symptoms for longer periods, 3 reduced participation in physical activity, and decreased shoulder-related quality of life. 16,37,44
Diverging strategies exist as to the optimum treatment for this group. For young, active male patients with primary traumatic ASDs, 2 systematic reviews have concluded that shoulder stabilizing surgery with postsurgical shoulder rehabilitation was superior to nonsurgical standard care treatment only in reducing the risk of recurrent ASDs. 19,34 These systematic reviews included 4 randomized controlled trials (RCTs) with rehabilitation of only primary traumatic ASDs, 5,22,27,50 and these studies had several limitations: limited description of the rehabilitation protocol and lack of short-term treatment effect measures. Moreover, the primary endpoint was objectively registered anterior shoulder redislocation, which usually does not occur until 12 to 24 months after a primary traumatic ASD. 40 Therefore, from RCTs, little is known about patients with primary and recurrent traumatic ASDs on short-term and subjective outcomes of shoulder symptoms and function. 25
Furthermore, in qualitative, cross-sectional, and cohort studies, it was reported that many patients (∼50%) with a primary traumatic ASD who had been treated nonsurgically did not experience recurrent ASDs, whereas shoulder function in general was poor. 21 Also, it was reported that some patients who were treated with surgery and rehabilitation reported poor shoulder function, a fear of reinjuries, and unstable shoulders for long periods. 16,44 This would tend to indicate that nonsurgical standard care treatment is only suboptimal and that initial surgery is not ideal for all patients with traumatic ASDs (primary or recurrent). In addition, as not all patients are candidates for surgery (surgeon’s or one's own decision), an efficient and evidence-based standardized physical therapy regimen for the nonsurgical management of traumatic ASDs is needed. Such a regimen has not yet been established, as also seen in treatment recommendations within this area, which are only weakly substantiated as described because of the absence of RCT studies that compare the effect of nonsurgical exercise programs. 25 Traditionally, nonsurgical standard care treatment for patients with traumatic ASDs consists of closed reduction followed by immobilization in a shoulder sling, and, if provided, some type of physical therapy (eg, shoulder range of movement exercises and low load strengthening of the rotator cuff muscles). 5,22,27 However, as a traumatic ASD often leads to loss of mechanical stability and deficits to the global neuromuscular and proprioceptive systems, in addition to weakness of the rotator cuff muscles, 9,10,20,29,43 a greater focus on neuromuscular exercises that enhance compensatory functional shoulder stability may seem relevant. While other studies on patients with traumatic knee instability (anterior cruciate ligament tears) have shown a large effect for progressive neuromuscular exercise programs, 11,17 such programs do not exist for patients with traumatic ASDs. 53 This is why it seems reasonable to also develop and evaluate treatment effects of such a program for patients with traumatic ASDs. 36
Therefore, the purpose of this RCT was to evaluate the efficacy and safety of a nonsurgical, supervised, progressive shoulder instability neuromuscular exercise (SINEX) program compared with a self-managed, home-based, standard care shoulder exercise program (HOMEX) in patients with traumatic ASDs. The hypothesis was that SINEX would (1) have a larger effect than HOMEX and (2) not induce more adverse events than HOMEX.
Methods
Trial Design
A multicenter, randomized, assessor-blinded, controlled clinical superiority trial was conducted using a parallel (1:1) group design. All patients gave written informed consent, and the study fulfilled the principles of the Declaration of Helsinki. 51 The study conformed to the CONSORT 2010 statement. 41 Details of the trial design and methods have been published elsewhere. 15 The statistical analysis plan is provided as supplementary material (see Appendix 1, available as supplemental material). Deviations to the study protocol 15 were as follows: Initially, patients had to have clinical signs of anterior shoulder instability with positive findings on a minimum of 2 of 3 clinical tests (apprehension, relocation, surprise). However, this criterion was removed from inclusion criteria because many of the patients reported poor shoulder function without having clinical signs of anterior shoulder instability. However, the clinical tests were retained as treatment effect measures. Furthermore, the objective measurement of prone-lying shoulder stability (using a Nintendo Wii Balance Board), originally included in the objective outcome test battery, 15 was withdrawn because of low concurrent validity compared with the gold standard (force platform). 14
Setting and Participants
Patients were recruited from 3 orthopaedic shoulder units in the Regions of Southern and Northern Denmark from March 2015 to March 2017, with the final deadline for enrollment set at March 31, 2017. 15 Eligible patients were men and women between the ages of 18 and 39 years with trauma-initiated, unidirectional anterior shoulder instability. 18 Inclusion criteria were radiographically verified acute primary or recurrent ASDs (using a radiograph that showed the actual dislocation, which is standard procedure before manual reduction in Denmark) and self-reported decreased ability to perform shoulder movements during daily activities in the previous 7 days. Patients were assessed for eligibility to participate in the RCT within 3 to 6 weeks after their current shoulder injury. This screening window was chosen to ensure that all patients had completed initial immobilization of the shoulder after reduction. Exclusion criteria were humeral head fractures and/or bony Bankart lesions requiring early surgery (evaluated by orthopaedic surgeons), prior surgery in the affected shoulder joint, more than 5 ASDs in the patient’s lifetime, suspected competing diagnoses (such as rheumatoid arthritis, cancer, neurological disorders, fibromyalgia, psychiatric diseases), sensory and motor deficits in the neck and shoulder, current pregnancy, inability to speak or write Danish, and/or inability to attend 12 weeks of supervised shoulder training.
Stratified Randomization and Blinding
Patients were randomly assigned to either SINEX or HOMEX with a 1:1 allocation per study site, stratified according to injury status: that is, a primary (first-time) or recurrent (second- to fifth-time) ASD. A computer-generated randomization sequence was produced using PROC PLAN (SAS Institute) to generate the schedules before any patient was enrolled, allocating patients in permuted blocks of 2, 4, or 6 to the SINEX or HOMEX program. At each trial site, these (stratified) lists were sequentially numbered in opaque, concealed envelopes. A total of 2 outcome assessors, blinded to treatment allocation, performed all measurements according to procedures described previously. 15
Interventions
As standard care treatment varies, the HOMEX program was developed to reflect the core similarity of standard care packages while still representing a realistic treatment option. The SINEX program was developed to accommodate shoulder mechanical loss and proprioceptive impairment subsequent to trauma-initiated primary or recurrent ASDs. 9,10,20,29,43
SINEX Program
A cornerstone of the neuromuscular exercises was movement quality through guided supervision from physical therapists. The neuromuscular exercises included strength, coordination, balance, and proprioception, which were integrated simultaneously into various body positions, enhancing compensatory functional shoulder stability. This is in contrast with the standard care program (HOMEX) that relied primarily on strength training to increase muscle mass. The SINEX group received 12 weeks of individually tailored, supervised sessions of progressive shoulder exercise in addition to functional kinetic chain exercise. The SINEX program included 7 exercises targeting the glenohumeral and scapular muscles. Each exercise has 7 progression levels (basic to elite), with exercises at the basic level performed every day (2 × 20 repetitions) and exercises at the elite level performed 3 times weekly (2 × 10 repetitions). Exercises followed general strength training principles, with basic and elite levels referring to low and high load exercises. All patients in the SINEX group had access to online exercise instructions and videos through the physical therapy website (digifys.com).
Supervised sessions were provided throughout the 12 weeks, lasting approximately 45 minutes each. Supervised sessions were offered twice a week for the first 2 weeks and then once a week for the remaining 10 weeks, summing up to a maximum of 14 sessions. The amount of supervised sessions needed was decided by physical therapists based on the movement control and capability of the individual patient. However, to satisfactorily complete the SINEX program, attendance of at least 7 (50%) supervised sessions (of 14 possible) was required in addition to completion of at least two-thirds (66%) of the planned home-based exercises (self-reported training diary). A full description of the SINEX program is provided as supplementary material (see Appendix 2, available as supplemental material).
HOMEX Program
The HOMEX group received 1 introductory supervised physical therapy session, including a leaflet with photographs and descriptions of exercises. Patients were instructed not to perform exercises that exceeded their pain limit and that provoked shoulder pain. The HOMEX program consisted of active exercises for the rotator cuff and scapular muscles using elastic bands and 1 exercise for mobility/coactivation of the scapular and core stability muscles. Patients had to perform the exercises for 12 weeks, 3 times weekly (2 × 10 repetitions). After 6 weeks, patients received a telephone call from a physical therapist to ascertain the appropriate progression of and compliance with the exercises. Compliance with the HOMEX program was reached, with a minimum of two-thirds (66%) of the planned home training completed (via self-reported training diary). Further details of the HOMEX program are provided as supplementary material (see Appendix 3, available as supplemental material).
Outcome Measures
The primary endpoint was the change in the total score of the patient-reported Western Ontario Shoulder Instability Index (WOSI) from baseline to the 12-week follow-up. The WOSI covers 21 items, each ranging from 0 to 100, with higher scores representing worse shoulder-related quality of life. 26 A reliable and validated Danish version of the WOSI was used. 12
Secondary patient-reported outcomes were the subdomain scores (physical symptoms, sport function, lifestyle, emotions) of the WOSI collected at baseline and weeks 4, 8, and 12. Further secondary patient-reported outcome measures included the Tampa Scale of Kinesiophobia, 35,47 the EuroQol 5-Dimensions questionnaire, 38 and the Patient-Specific Functional Scale 7 as well as pain intensity now, average pain intensity in the past 24 hours, and average pain intensity in the previous 7 days using the Numeric Pain Rating Scale (NPRS). 8 Objective secondary outcome measures included the Constant-Murley score (CMS), including the CMS subdomains of range of motion and isometric shoulder abduction strength (in kg) with the use of a dynamometer, 2 blindfolded shoulder joint reposition sense (JRS) testing within low ranges of shoulder flexion and abduction (0° to 60° ± 10°) with the use of a laser beam, 45 and clinical tests for anterior shoulder instability 13 as well as the Beighton score for the classification of generalized joint hypermobility. 4,24 Patients further reported their impression of recovery at week 12 using the global perceived effect (GPE) scale and responded to questions on exercise-related adverse events and other shoulder-related issues after participation.
Statistical Analysis
To reduce bias in the interpretation of the primary outcome, a blinded interpretation framework was used (see Appendix 4, available as supplemental material). 23 All analyses followed the intention-to-treat (ITT) principle; missing data were replaced using nonresponder imputation (ie, baseline observation carried forward technique) 33 because of the assumption that those who dropped out returned to their baseline WOSI score (ie, null imputation). 49
Simple descriptive statistics of either group means with standard deviations or within-group numbers and proportions were used. Change values were calculated, and results are presented as the estimated adjusted between-group mean difference of change values, besides adjusted risk differences, with 95% CIs and associated P values. Analysis of covariance (ANCOVA) was used to analyze the mean change and self-reported data of continuous outcomes, presented as estimates of least squares means with 95% CIs. The model included treatment group, study center, sex, and injury status (primary or recurrent ASD) as fixed effects, adjusting each patient’s dependent outcome for his or her baseline score, with baseline as a covariate. For the categorical outcomes (eg, clinical test findings, adverse events), logistic regression analysis was used, presenting probability estimates with 95% CIs using the same fixed effects and covariates as in the ANCOVA above. For the categorical outcomes on self-reported data and adverse events at week 12, data are presented as percentages, with differences between groups determined by a chi-square test or Fisher exact test.
For the longitudinal part of the trial (no imputation for missing data needed), a linear mixed model with repeated measures of the WOSI (weeks 4, 8, and 12) was performed to test the difference and trajectory over time between the 2 groups (interaction: group × time) with the same fixed effects and covariates as in the ANCOVA. For sensitivity and exploratory purposes, per-protocol analysis was performed, which included only the participants who had acceptable exercise compliance. 15
The study was powered to detect a difference of at least 250 points as the minimal clinically important difference (MCID) between SINEX and HOMEX for the primary outcome. 28 To achieve 90% power to show a clinically relevant between-group difference in favor of SINEX, with a 2-sided type I error rate of 5%, 36 patients per group were necessary.
All statistical analyses were performed with SPSS (Version 24.0; IBM). P values <.05 (2-sided) were considered statistically significant.
Patient Involvement
Patients with traumatic ASDs provided feedback about the neuromuscular exercises during the development and design of the SINEX program. After consenting to participate in the study, the patients were asked whether they wanted to receive a letter explaining the results of this trial. Accordingly, a letter in lay terms will be forwarded to those interested when the study findings are published.
Results
Participant Characteristics
A total of 130 patients were screened for eligibility. Of these, 56 patients fulfilled the eligibility criteria, comprising the ITT population (Figure 1), and were randomized to either the SINEX or the HOMEX group. A total of 51 of 56 (93%) completed the 12-week follow-up assessment (SINEX: n = 27; HOMEX: n = 24). At baseline, the groups were comparable in demographics and clinical characteristics (except for the WOSI lifestyle and NPRS within the past 24 hours in which the HOMEX group had poorer scores). The mean age was 25.8 ± 5.8 years and 26.2 ± 6.4 years for the HOMEX and SINEX groups, respectively, and a majority of the patients were male (49/56; 88%). Baseline characteristics are described in Tables 1 and 2.
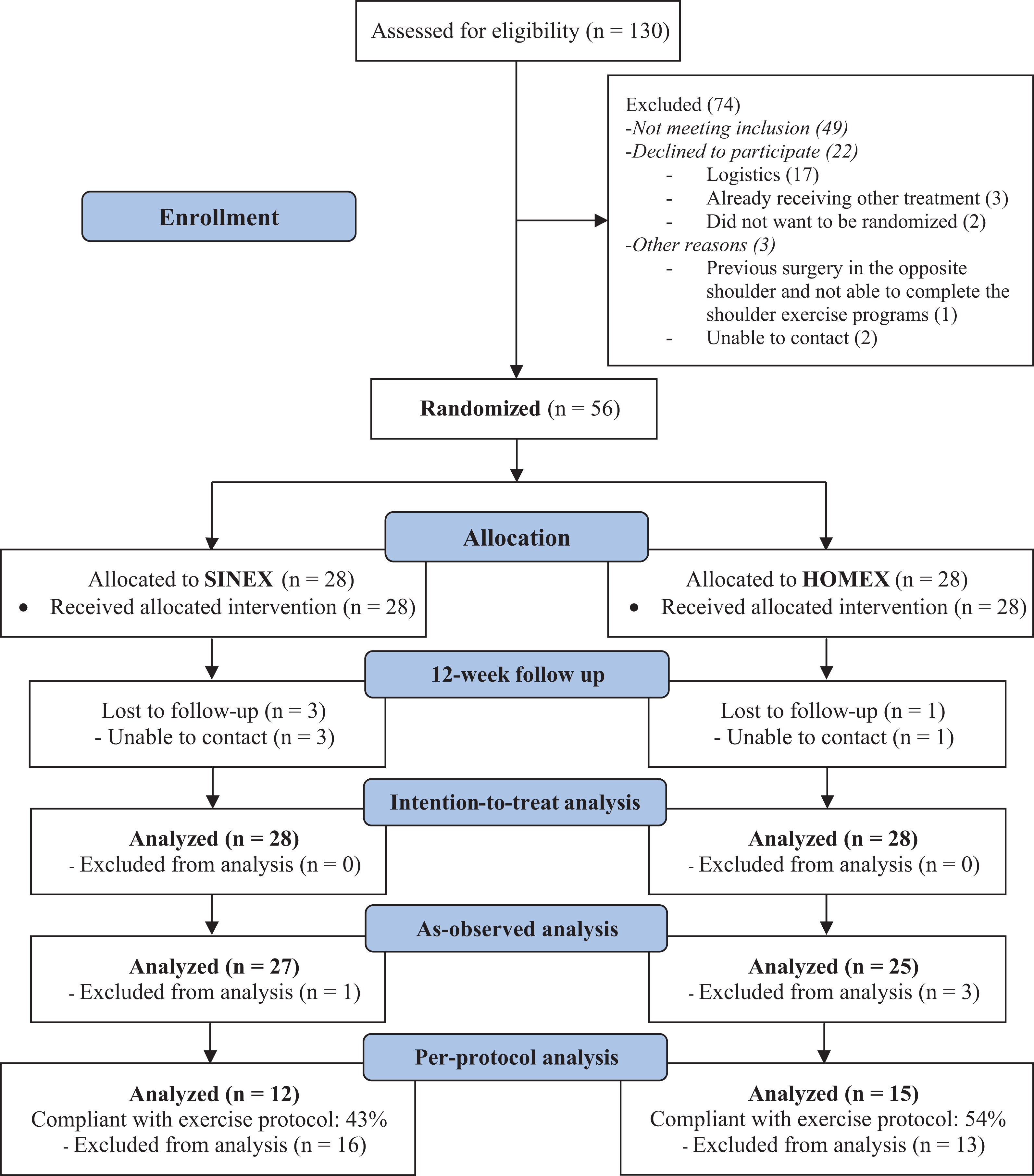
Flowchart of participants with traumatic anterior shoulder dislocations (ASDs) in the study. A total of 49 patients did not meet the inclusion criteria: 11 did not meet the age requirements (<18 years: n = 5; >39 years: n = 6), 11 had no radiographic verification of a shoulder dislocation, 17 reported not having any problems with shoulder movements during daily activities in the previous 7 days, 2 patients had a bony Bankart lesion or humeral head fracture, 1 patient had experienced more than 5 ASDs in his or her lifetime, 2 patients had suspected competing diagnoses (sclerosis: n = 1; unknown neurological disorder: n = 1), 1 patient was pregnant, 3 patients had no clinical signs of anterior shoulder instability, and 1 patient was not able to speak and write Danish. HOMEX, self-managed, home-based, standard care shoulder exercise program; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise.
Baseline Demographic Information a

a Data are reported as n (%) unless stated otherwise. HOMEX, self-managed, home-based, standard care shoulder exercise program; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise.
b During athletic activities (soccer, gymnastics, fun wrestling, motocross).
Baseline Outcome Measure Scores a
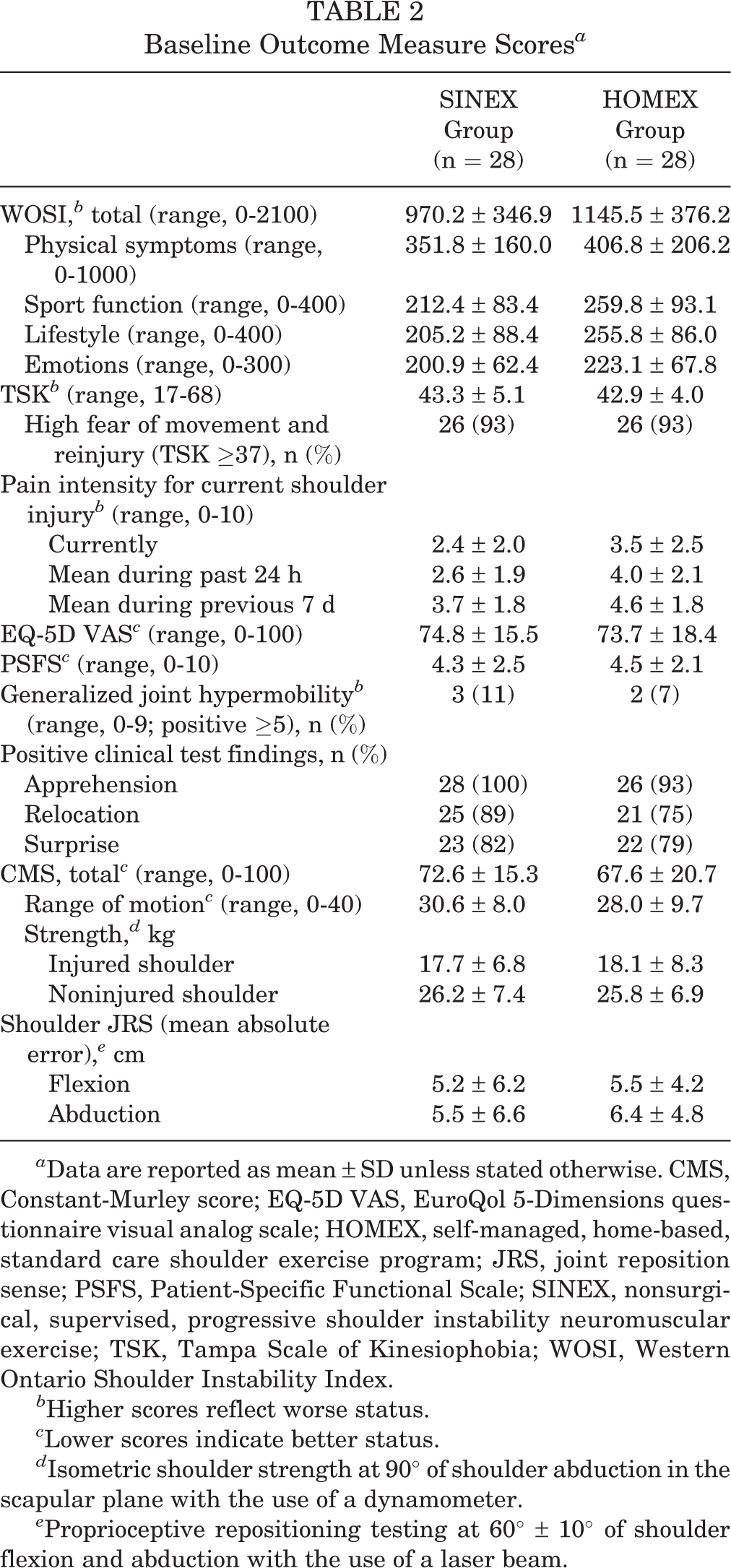
a Data are reported as mean ± SD unless stated otherwise. CMS, Constant-Murley score; EQ-5D VAS, EuroQol 5-Dimensions questionnaire visual analog scale; HOMEX, self-managed, home-based, standard care shoulder exercise program; JRS, joint reposition sense; PSFS, Patient-Specific Functional Scale; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise; TSK, Tampa Scale of Kinesiophobia; WOSI, Western Ontario Shoulder Instability Index.
b Higher scores reflect worse status.
c Lower scores indicate better status.
d Isometric shoulder strength at 90° of shoulder abduction in the scapular plane with the use of a dynamometer.
e Proprioceptive repositioning testing at 60° ± 10° of shoulder flexion and abduction with the use of a laser beam.
For those returning diaries after completing the home exercise (n = 18 patients in each group), the overall adherence was a mean of 71% for SINEX and 79% for HOMEX. However, compliance with SINEX (at least 7/14 supervised exercise sessions and at least 66% of the scheduled home-based training) corresponded to 12 of 28 (43%) patients attending a mean of 9 supervised sessions and 82% of the scheduled home-based training. Compliance with HOMEX (at least 66% of the scheduled home-based training) corresponded to 15 of 28 (54%) patients performing a mean of 87% of the home-based training. Therefore, the per-protocol population was composed of 12 and 15 patients for the SINEX and HOMEX groups, respectively.
Primary Outcome
The SINEX group had a significantly greater improvement on the WOSI total, although marginally below the cutoff for the MCID, compared with the HOMEX group in the change from baseline to the 12-week follow-up (between-group mean difference, –228.1 [95% CI, –430.5 to –25.6]; P = .028) (Table 3). The mean change in the WOSI total score was 655.3 (95% CI, 457.5 to 853.0) in the SINEX group and 427.2 (95% CI, 245.9 to 608.6) in the HOMEX group.
Changes in Outcome Measure Scores Between Baseline and Week 12 in Intention-to-Treat Population a
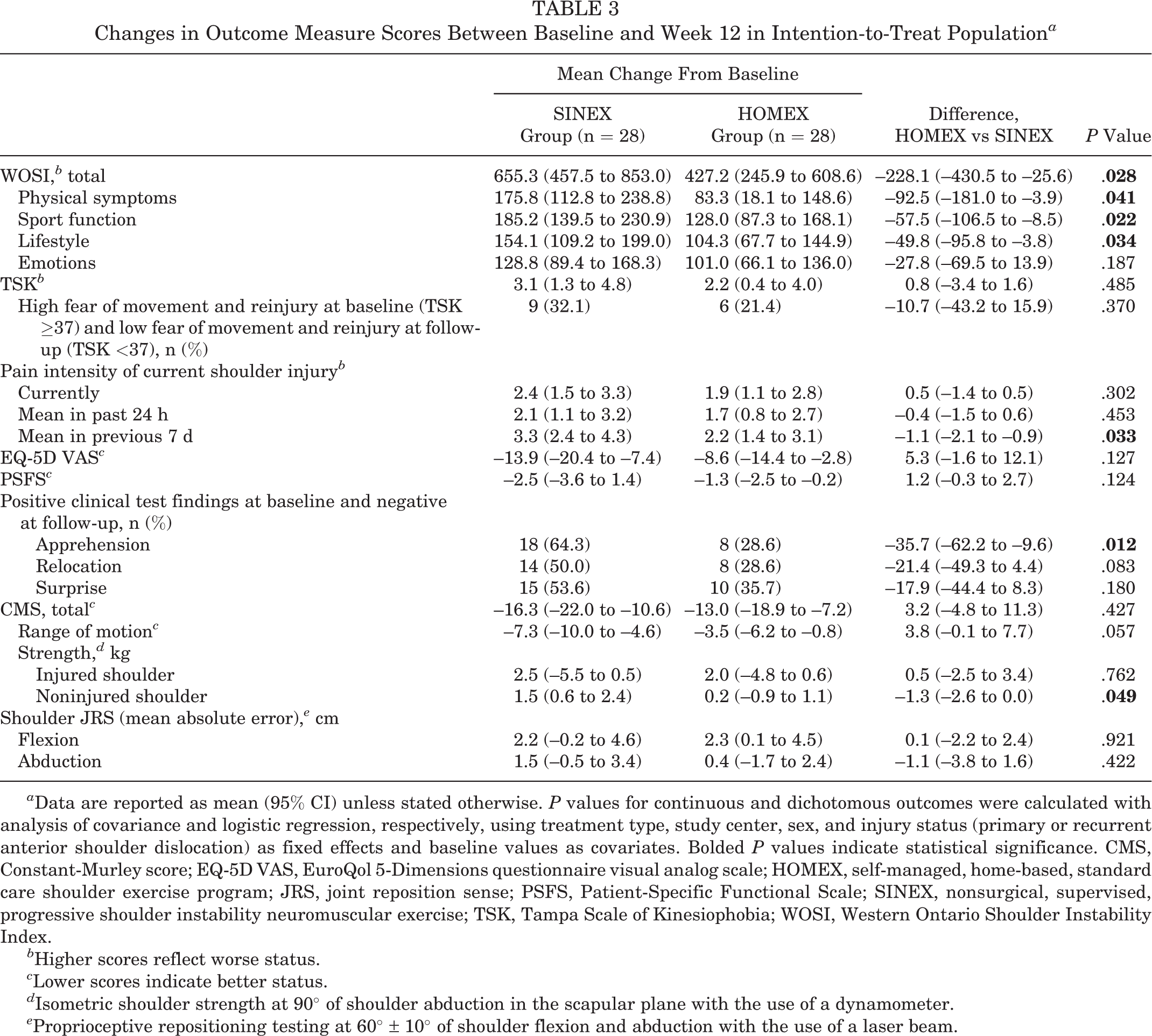
a Data are reported as mean (95% CI) unless stated otherwise. P values for continuous and dichotomous outcomes were calculated with analysis of covariance and logistic regression, respectively, using treatment type, study center, sex, and injury status (primary or recurrent anterior shoulder dislocation) as fixed effects and baseline values as covariates. Bolded P values indicate statistical significance. CMS, Constant-Murley score; EQ-5D VAS, EuroQol 5-Dimensions questionnaire visual analog scale; HOMEX, self-managed, home-based, standard care shoulder exercise program; JRS, joint reposition sense; PSFS, Patient-Specific Functional Scale; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise; TSK, Tampa Scale of Kinesiophobia; WOSI, Western Ontario Shoulder Instability Index.
b Higher scores reflect worse status.
c Lower scores indicate better status.
d Isometric shoulder strength at 90° of shoulder abduction in the scapular plane with the use of a dynamometer.
e Proprioceptive repositioning testing at 60° ± 10° of shoulder flexion and abduction with the use of a laser beam.
Secondary Outcomes
On 3 of 4 WOSI subdomains and in pain during the previous 7 days, significantly larger improvements were seen in favor of the SINEX group (Table 3). Further significant improvements in favor of SINEX were seen in clinical signs of anterior shoulder instability with the apprehension test and in CMS strength of the noninjured shoulder (Table 3). Also, less than half of the patients (33% and 46%, respectively) in the SINEX and HOMEX groups returned to preinjury levels of sport (Table 4). At the same time, the mean ratings of actual shoulder function and ability to perform sport/leisure activities on the GPE scale were rated “improved” to “much improved,” with a statistically significant difference in favor of the SINEX group compared with the HOMEX group (6.2 vs 5.5 [P = .012] and 5.8 vs 4.9 [P = .025], respectively) (Table 4).
Self-reported Data at 12-Week Follow-up a

a Data are reported as n (%) unless stated otherwise. Bolded P values indicate statistical significance. HOMEX, self-managed, home-based, standard care shoulder exercise program; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise.
Although not statistically significant, only half of the patients in the SINEX group (3/27; 11%) compared with the HOMEX group (6/24; 25%) underwent or were referred for shoulder stabilizing surgery (Table 4). In the multilevel analyses, there was no difference between groups over time for the WOSI total score and for each of the WOSI subdomain scores (baseline and weeks 4, 8, and 12), which was only shown for the WOSI total (Figure 2).

Western Ontario Shoulder Instability (WOSI) total score at baseline and weeks 4, 8, and 12 for the SINEX versus HOMEX groups among patients with traumatic anterior shoulder dislocations. The graphs illustrate the results from the intention-to-treat population. Data points represent least squares means. (A) Nonresponder imputation (SINEX, n = 28; HOMEX, n = 28). (B) As observed (SINEX, n = 28, 26, 18, and 27, respectively; HOMEX, n = 28, 25, 22, and 25, respectively). (C) Per-protocol analysis (SINEX, n = 12, 10, 10, and 12, respectively; HOMEX, n = 15, 14, 15, and 15, respectively). HOMEX, self-managed, home-based, standard care shoulder exercise program; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise.
Adverse Events
Few patients reported recurrent ASDs at the 12-week follow-up, with no significant difference between groups (Table 4). In addition, a large proportion (85% and 83%, respectively) in the SINEX and HOMEX groups reported “very little or not at all” on recurrent anterior shoulder instability or subluxations, with no significant difference between groups (Table 4). Short-lasting adverse events at 12 weeks were few, with no significant group differences (Table 5). The most common adverse events were exercise-induced shoulder pain, soreness, and muscle fatigue (SINEX: n = 10; HOMEX: n = 10).
Adverse Events From Baseline to Week 12 a

a Data are reported as n (%). Includes any specific and serious adverse events. P values were calculated with the Fisher exact test. HOMEX, self-managed, home-based, standard care shoulder exercise program; SINEX, nonsurgical, supervised, progressive shoulder instability neuromuscular exercise.
Sensitivity and Per-Protocol Analyses
Patients who did and did not complete the follow-up assessments (5 patients in total) did not differ on all baseline variables (data not presented), except for employment now in which those lost to follow-up had a lower rate of full-time employment and a higher rate of sick leave. The per-protocol analysis confirmed the ITT analysis, with further significant group differences in favor of SINEX (data not presented).
Discussion
Although the MCID was not reached, this multicenter RCT involving patients with traumatic ASDs showed the superior effects of supervised neuromuscular shoulder exercise versus standard care shoulder exercise after 12 weeks of nonsurgical treatment with regard to the primary outcome of patient-reported shoulder function and quality of life. Further superior effects of SINEX were seen in a number of key secondary outcomes, and although not statistically significant, less than half of the patients in the SINEX group (3/27) compared with the HOMEX group (6/24) underwent or were referred for shoulder stabilizing surgery at the 12-week follow-up. Satisfaction with both exercise programs was high, and no serious adverse events were reported.
We are not aware of any other RCTs investigating the effectiveness of a nonsurgical, physical therapist–supervised progressive exercise regimen in patients with traumatic ASDs. 25 Only 1 other study (noncontrolled cohort study) has evaluated the effect of a 12-week nonsurgical progressive shoulder rehabilitation program in patients with traumatic ASDs (primary dislocations only). 1 That study found that 15 of 20 (75%) patients had no clinical sign of anterior shoulder instability (negative apprehension test finding), 1 which is in line with the current results of 18 of 28 (64%) patients in the SINEX group. Regarding returning to preinjury levels of sport, 15 of 20 (75%) patients in the study by Aronen and Regan 1 returned to unrestricted athletic participation at the 12-week follow-up, which included the sport that caused their initial dislocation. This is in contrast with the current findings in which a smaller proportion of patients in both groups (SINEX, 9/27 [33%]; HOMEX, 11/24 [46%]) returned to their preinjury level of sport at the 12-week follow-up. One explanation for this discrepancy may be the difference in populations (occupational 1 vs general and not necessarily athletic population [no sport to return to] and first-time 1 vs first-time or recurrent ASD). Another reason may be the different definitions of return to sport (“being allowed to participate in unrestricted athletic participation” 1 and “returning to preinjury level of sport”). Nonetheless, the superior benefit of SINEX in the current study was further consistent with the results of the GPE scale in which the mean rating (7-point Likert scale; 7 = best) for capability to perform sport/leisure activities was higher in the SINEX group than in the HOMEX group (5.8 vs 4.9, respectively; P = .025) at the 12-week follow-up. This corresponds to “much improved” from only “improved.” Thereby, the current results seem to reflect the conclusion of Aronen and Regan, stating “that a progressive neuromuscular program substantially improves the likelihood of full return to activity.”
In agreement with the hypothesis, the SINEX program with supervised physical therapy guidance in neuromuscular shoulder exercises had a larger effect compared with the HOMEX program and was safe to perform. However, with the 95% CI of the primary outcome including the cutoff of 250 points for the WOSI, prespecified as a clinically relevant MCID, a true between-group difference in favor of SINEX cannot be ruled out. However, while previous studies have recommended changes ranging from 210 to 400 of 2100 (10%-19%) for the WOSI total score, 6,28,46 one might question the current MCID threshold, as it is at the lower end of the suggested changes (228.1). However, despite the fact that both groups were expected to improve, regardless of treatment allocation, a large between-group treatment effect (eg, MCID of 400/2100 [19%]) was not anticipated . Thus, the current MCID of at least 250 of 2100 (12%) points for the WOSI total was pragmatically chosen based on the existing literature and within the common rule of thumb of a minimum of 10% difference for interpreting MCIDs in patient-reported outcomes. 39 Furthermore, most of the secondary patient-reported outcome measures supported the primary finding in the current study but not the objective outcome measures of the CMS and JRS. The reason may be that the CMS is not specifically designed to evaluate shoulder instability 48 and that JRS testing, for reliability reasons, 45 was performed in low-range positions only (<60° of shoulder flexion/abduction), thus not able to capture the proprioceptive changes achieved during the SINEX program predominantly including overhead exercises.
Finally, it should be noted that the long-term effects regarding preventing recurrent ASDs, avoiding surgery, and returning to sport, among others, of the current treatments are unknown. In addition, it is unknown how much added cost attributed to physical therapy there is associated with administering SINEX, but a long-term follow-up at 1 and 2 years and cost-benefit analysis will be performed.
Limitations and Strengths
Although the sample size and adherence were relatively low, which increased the risk of type II errors, the current data showed a significant and nearly clinically relevant difference in favor of SINEX. To further support these findings, both the sensitivity and per-protocol analyses confirmed the current ITT analysis.
Another limitation is that the number of glenohumeral Hill-Sachs lesions and anterior bone loss in each group are unknown. However, the nature of the randomized design ensures that these characteristics were equally distributed between the 2 groups, thereby limiting any potential bias. Also, the decision to enroll patients with primary as well as recurrent ASDs may seem controversial, as they may have had different starting points for treatment. However, a recent cross-sectional analysis revealed that patients with primary and recurrent ASDs present with equally poor shoulder function and a high fear of reinjuries, thereby indicating equal indications for receiving treatment regardless of the number of previous dislocations. 16 Furthermore, although stratification may be seen as a limitation, the use of this technique ensured that the number of patients with primary and recurrent ASDs were equally distributed between the 2 groups, thereby limiting any potential bias.
In some countries, it may be that a home-based program is not the standard care for patients with traumatic ASDs, which is why the generalizability of the current findings may be limited. However, the current HOMEX program was designed to reflect the core similarity of standard care packages across most hospitals in Denmark. Because of the design, it was not possible to blind the patients and the treating physical therapists; yet, because all outcome assessments and analyses of the primary outcome were performed blinded and all WOSI scores showed a consistent pattern in favor of SINEX, this is not considered a major limitation.
It is also a limitation that we cannot conclude whether it is the neuromuscular aspect, the difference in supervision, or a combination of the two that makes up the current treatment effect. Finally, because of technical errors having wrongly allocated 2 patients in the analysis performed after the consensus agreement on blinded data interpretation (see Appendix 4, available as supplemental material), these data could not be used entirely as intended. However, the revised analysis further confirmed the findings in the blinded interpretation document, and the topics suggested as points for discussion in the consensus agreement could still be used.
One strength of this study is the detailed and published protocol including blinded analysis and interpretation of the primary outcome. Furthermore, this study developed and used a standardized, individualized, physical therapist–supervised neuromuscular shoulder exercise program targeting both primary and recurrent ASDs. This study therefore complies with recent recommendations for further research, pointing to the need for more studies to refine an ideal physical therapy regimen for nonsurgical management after primary and recurrent ASDs. 25
Another strength is that only 2 outcome examiners were used, which is why assessment variability was kept to a minimum for the objectively measured outcomes. Also, the rate of loss to follow-up was low and equal in both groups.
Finally, it is a strength that the control group (HOMEX) received a realistic and active treatment approach that is often used today and expected to induce a true treatment effect. Still, SINEX managed to improve patients more.
Conclusion
Ultimately, 12 weeks of neuromuscular shoulder exercise (SINEX) was superior to a standard care home exercise program (HOMEX) in improving patient-reported shoulder function in patients with traumatic ASDs, although the improvement did not reach the MCID. As SINEX showed the most benefit, this exercise program could potentially be the first-choice option in patients with traumatic ASDs who are not candidates for early shoulder stabilizing surgery. Further long-term treatment effects on patient-reported outcomes and shoulder redislocations as well as socioeconomic evaluations of SINEX are needed to explore the potential for nonsurgical rehabilitation of this complex patient group.
Supplemental Material
Supplemental Material, DS_10.1177_2325967119896102 - Neuromuscular Exercises Improve Shoulder Function More Than Standard Care Exercises in Patients With a Traumatic Anterior Shoulder Dislocation: A Randomized Controlled Trial
Supplemental Material, DS_10.1177_2325967119896102 for Neuromuscular Exercises Improve Shoulder Function More Than Standard Care Exercises in Patients With a Traumatic Anterior Shoulder Dislocation: A Randomized Controlled Trial by Henrik Rode Eshoj, Sten Rasmussen, Lars Henrik Frich, Inge Hvass, Robin Christensen, Eleanor Boyle, Steen Lund Jensen, Jens Søndergaard, Karen Søgaard and Birgit Juul-Kristensen in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank the staff involved in prescreening the patients at the Odense University Hospital, Aalborg University Hospital, and South-West Jutland Hospital; Annie Gam Petersen for the recruitment of study participants; Odense University Hospital, Aalborg University Hospital, and South-West Jutland Hospital for the use of their facilities for treatment and outcome assessments; Elizabeth Andreasen for help with outcome assessments and data collection; physical therapists Lotte Mejlvig Nielsen, Annelene Houen Larsen, Marianne Gregersen, Gitte Poulsen, Sarah Tofte Benzon, and Mette Nybo Bjerregaard for the instruction and treatment of study participants; Anne Marie Rosager for assisting with administrative tasks; Suzanne Capell for academic editing; and the study participants who made this trial possible.
Final revision submitted October 15, 2019; accepted October 25, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee for the Region of Southern Denmark (project No. S-20140093).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.