
Abstract
Background:
Augmentation of Bankart repair with long head of the biceps tendon transfer has been previously described, although there is a paucity of literature describing its biomechanical effects.
Purpose/Hypothesis:
The purpose of this study was to assess the effect of augmenting Bankart repair with either the conjoint tendon or the long head of the biceps tendon, both with and without subcritical (13%) glenoid bone loss. We hypothesized that, in a cadaveric model, augmenting Bankart repair with the long head of the biceps tendon would restore a greater degree of stability compared with augmenting Bankart repair with the conjoint tendon.
Study Design:
Controlled laboratory study.
Methods:
A total of 12 cadaveric shoulders were tested on a 6-degrees-of-freedom robotic musculoskeletal simulator to measure the peak resistance force due to an anterior displacement of 1 cm. The rotator cuff muscles were loaded during testing to simulate physiological conditions. The following test conditions were used for each specimen: (1) intact shoulder, (2) Bankart lesion with 13% anterior bone loss, (3) 13% bone loss with Bankart repair (anchors placed at the 3-, 4-, and 5-o’clock positions), (4) 13% bone loss with both Bankart repair and transfer of the long head of the biceps tendon, and (5) 13% bone loss with Bankart repair and transfer of the conjoint tendon.
Results:
Labral repair with the addition of long head of the biceps tendon transfer had the greatest peak resistance force to anterior displacement among all groups (54.1 ± 5.5 N) and was significantly stronger than both standard Bankart repair by 16.3% (46.5 ± 7.6 N; P = .039) and the conjoint transfer procedure by 16.6% (46.4 ± 7.7 N; P = .008).
Conclusion:
Given the susceptibility of recurrent instability in shoulders with subcritical bone loss after isolated labral repair, it is important to consider augmenting Bankart repair in high-risk patients to avoid potential recurrence and the need for reoperations. Transferring the long head of the biceps tendon to the anterior glenoid represents one possible augmentation.
Clinical Relevance:
We present biomechanical data for a relatively novel technique for augmenting capsulolabral repair strength in an anterior instability model with subcritical bone loss. These data represent biomechanical justification for the utilization of this relatively novel technique.
Traumatic shoulder instability is one of the most common shoulder injuries among athletes. 6,7 Although Bankart repair is an effective method for addressing recurrent anterior shoulder instability, recent studies have demonstrated that failure to address glenoid bone loss is a common cause of recurrent instability after isolated Bankart repair. 4,10,13,17,25,26 In contrast to subcritical bone loss, multiple studies have defined critical bone loss of the anterior glenoid associated with recurrent anterior shoulder instability after Bankart repair, with percentages reported ranging from 15% to 30%. 9,11 Several open and arthroscopic operative techniques are utilized to reconstruct the glenoid with a variety of autograft and allograft sources. 1 –3,12 –14,16,20 –23,34 The Bristow-Latarjet procedure is being used with increasing frequency for addressing recurrent shoulder instability in the setting of glenoid bone loss. This surgical technique restores the congruity of the deficient glenoid by augmenting the anterior glenoid with the coracoid process. 32 The conjoint tendon, which remains attached to the transferred coracoid, creates a dynamic restraint to anterior translation of the humeral head with the arm in the abducted and externally rotated position. 32
Although the Bristow-Latarjet technique effectively addresses recurrent shoulder instability, this procedure is associated with a complication rate as high as 20%. 5 While cases of critical bone loss depend on restoring the architecture of the glenoid and warrant reconstruction with a bone graft, the necessity of osseous reconstruction of the glenoid in cases of subcritical bone loss is unclear. 10 Bankart repair augmented with long head of the biceps tendon transfer has been previously described, raising the question of whether isolated soft tissue transfer could effectively increase stability after Bankart repair in the setting of subcritical bone loss. 8 The advantageous feature of this tendon transfer was that it provided a functional sling effect. This study examines the effect of augmenting Bankart repair with either the conjoint tendon or the long head of the biceps tendon, both with and without subcritical (13%) glenoid bone loss. We hypothesized that augmenting Bankart repair with the long head of the biceps tendon would restore a greater degree of stability compared with augmenting Bankart repair with the conjoint tendon in a cadaveric model.
Methods
Preparation of Specimens
All specimens were purchased from a local medical donor bank. Before study initiation, an a priori power analysis was performed with a power level of 0.8 and planned effect size (f) of 0.5 for peak resistance force to anterior displacement. A total of 9 shoulders would be required for a significance level of .05. Therefore, 12 fresh-frozen cadaveric shoulders (6 men, 6 women) with a mean age of 53.9 years were utilized. Specimens older than 60 years were excluded to decrease the risk of an existing rotator cuff tear (all tested shoulders had intact rotator cuffs). Shoulders were excluded if they had moderate to severe shoulder osteoarthritis based on computed tomography (CT).
All skin and subcutaneous tissues were excised, and the shoulders were dissected down to the rotator cuff muscle bellies and tendons, the long head of the biceps brachii tendon, and the conjoint tendon. Care was taken not to destabilize the long head of the biceps tendon from its native groove. The osteotomized scapula and humerus were then potted in a 2-part urethane compound (Smooth-Cast 300Q; Smooth-On) utilizing custom fixtures. For testing, the glenoid surface was potted parallel to the horizontal plane, while the humerus was potted in 60° of abduction and neutral rotation. To maintain the dynamic stabilizers of the shoulder, dynamic loading of the rotator cuff was performed by placing 7.5-N deadweights on the supraspinatus, infraspinatus, teres minor, and subscapularis tendons. 11 Also, 10 N was applied to both the conjoint tendon and the long head of the biceps tendon by utilizing constant force springs. After mounting, pretest CT was performed to define a coordinate system (Figure 1). YG was defined as a vector from the most inferior point to the most superior point on the glenoid rim. XG was defined as a vector from posterior to anterior of the bony glenoid rim. ZG was calculated as a cross-product of the XG and YG axes. The midpoint of the superior and inferior points of the glenoid rim was determined to be the origin of the glenoid coordinate system. 18
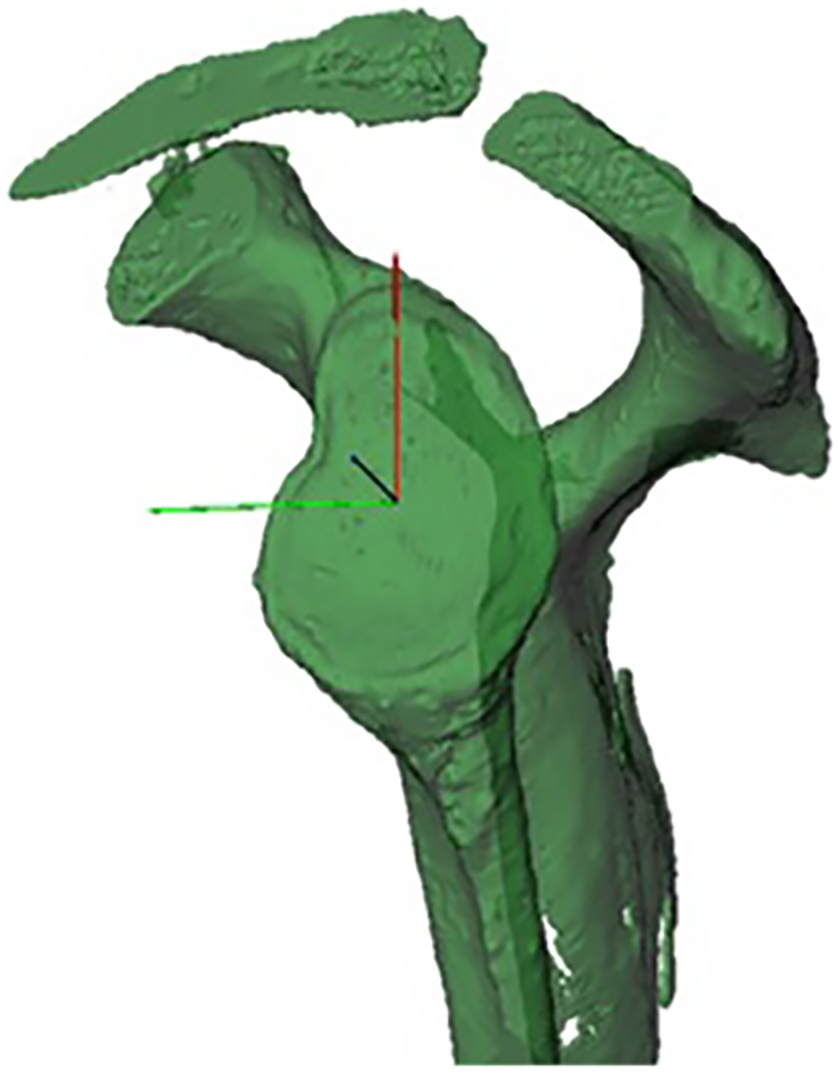
A 3-dimensional coordinate system is used to calibrate the robotic arm based on computerized tomography of each specimen. YG, vector from the most inferior point to the most superior point on the glenoid rim (red line); XG, vector from posterior to anterior of the bony glenoid rim (green line); ZG, cross-product of the XG and YG axes (black line).
Testing Apparatus
A 6-axis industrial robotic arm (KR 6 R700; KUKA) controlled by simVITRO LabVIEW software (Cleveland Clinic) was used for robotic force testing (Figure 2). This robot contains a multiaxis load cell (SI-580 N; ATI) for the measurement of forces in all 3 Cartesian directions. After mounting, the 3-dimensional relationships between the robot, load cell, and specimen were established using a 6-degrees-of-freedom digitizing probe (Optotrak; NDI). In addition to dynamically loading the rotator cuff, an additional 5-N compressive force was applied to the humerus during testing to centralize the humeral head on the glenoid surface. Starting from the centered position, the humeral head was displaced 1 cm in the anterior direction at a rate of 1.0 mm/s. The peak resistance force resulting from anterior displacement of the humeral head was recorded. There were 2 trials performed for each test condition, and the mean values were used for data analysis.

Robotic arm with a mounted specimen. Loading of the rotator cuff was performed using (A) deadweights (rotator cuff muscles) and (B) constant force springs (conjoint tendon and long head of the biceps tendon).
Test Conditions
The following test conditions were used for each specimen: (1) intact shoulder, (2) Bankart lesion with 13% anterior bone loss, (3) 13% bone loss with Bankart repair (anchors placed at the 3-, 4-, and 5-o’clock positions), (4) 13% bone loss with both Bankart repair and transfer of the long head of the biceps tendon, and (5) 13% bone loss with Bankart repair and transfer of the conjoint tendon. To access the labrum to create the Bankart lesion/bone loss, capsulotomy was performed from the 2- to 7-o’clock positions. Direct anterior bone loss was created by removing 13% of the anterior to posterior glenoid width (measured on individual CT scans). Both the long head of the biceps tendon and conjoint tendon transfer procedures were performed by splitting the subscapularis in line with the muscle fibers at the midportion of the tendon and anchoring the respective tendon (either the long head of the biceps tendon or conjoint tendon) 1 cm medial to the articular surface with a suture anchor using 6 alternating square knots (Figure 3). The respective tendons were anchored into the midportion of the anterior glenoid neck. Long head of the biceps tendon tenotomy was performed at its insertion onto the superior labral complex, while conjoint tendon tenotomy was performed at its insertion directly onto the coracoid. The capsular tissue and subscapularis tendon were then repaired over this. All tendon transfer and Bankart repair procedures were performed using Gryphon BR Suture Anchors (Mitek).

The long head of the biceps tendon (LHB) was transferred using a suture anchor placed 1 cm (green line orthogonal to the glenohumeral joint surface) medial to the glenoid surface and subsequently loaded during testing with a 10-N constant force spring. For clarity, the outline of the glenoid is marked in red, the humerus in white, and the coracoid in black.
Statistical Analysis
Ultimately, 1-way repeated-measures analysis of variance was used to determine the difference in mean peak force values among test conditions. Post hoc Dunnett analysis was performed to examine significant differences among individual groups. A P value of .05 was used to determine significance for all tests (SPSS Version 21.0; IBM).
Results
The mean peak resistance force in the intact shoulder group was 42.4 ± 4.3 N. Upon creating a Bankart lesion and 13% anterior bone loss, there was a statistically significant decrease in peak resistance force to anterior displacement (31.9 ± 5.8 N; P = .006). There was no statistically significant difference in peak resistance force between the Bankart repair group (46.5 ± 7.6 N) and the intact shoulder group (P = .99). Labral repair with the addition of long head of the biceps tendon transfer had the highest resistance to peak resistance force among all groups (54.1 ± 5.5 N) and was significantly greater than both standard Bankart repair by 16.3% (46.5 ± 7.6 N; P = .039) and the conjoint transfer procedure by 16.6% (46.4 ± 7.7 N; P = .008) (Figure 4). There was no significant difference in the mean peak resistance force between Bankart repair alone and Bankart repair with the addition of conjoint tendon transfer (P = .99).

Transferring the long head of the biceps tendon to the glenoid produces a greater resistance to translational force than Bankart repair alone and Bankart repair with transfer of the conjoint tendon. Arrows denote statistical significance (P < .05). LHB, long head of the biceps tendon.
Discussion
Our objective was to augment Bankart repair with either the long head of the biceps tendon or the conjoint tendon and determine which tendon transfer restores a greater degree of resistance to anterior displacement of the humeral head in the setting of subcritical bone loss of the anterior glenoid. Labral repair augmented with long head of the biceps tendon transfer produced significantly greater resistance to anterior displacement of the humeral head compared with the intact native labrum. Additionally, this transfer provided significantly greater resistance force compared with transfer of the conjoint tendon.
Recurrent anterior shoulder instability in the absence of a critical glenoid defect is most commonly addressed with isolated Bankart repair. 33 Instability recurrence rates range from 2% to 8%. Analysis of these recurrent cases of shoulder instability during revision surgery has demonstrated that failure to address anterior glenoid bone loss is a common cause of recurrent instability. 28 –31 While the Bristow-Latarjet procedure addresses critical glenoid bone loss in recurrent shoulders, there is no consensus regarding the optimal modality for addressing subcritical bone loss. 11 Several studies have defined subcritical glenoid bone loss and examined the impact of outcomes after isolated labral repair in patients with subcritical bone loss. 10,15,19 Shaha and colleagues 24 reported that 13.5% glenoid bone loss was associated with poor outcomes in patients who underwent isolated arthroscopic labral repair. They measured bone loss using magnetic resonance imaging with the perfect circle technique described by Harmsen and Huijsmans, 13 and patients were divided into quartiles based on the percentage of bone loss. They arbitrarily set the subcritical threshold cutoff at 13.5%. Patients with ≥13.5% bone loss were found to have worse functional outcomes and a greater degree of recurrence. Based on this threshold, Dickens and colleagues 10 conducted a case-control study to examine the effect of subcritical bone loss in collegiate football players after arthroscopic labral repair. In this series, 47 patients had <13.5% bone loss, and 3 patients had ≥13.5% bone loss. Additionally, Shin et al 27 performed a cadaveric study to determine the percentage of bone loss at which soft tissue repair alone fails to restore anterior-inferior glenohumeral translation. They created 10%, 15%, 20%, and 25% glenoid bone defects and found that glenohumeral translation could not be adequately restored once the bony defect exceeded 15%. 27
Complications after a Bristow-Latarjet procedure include recurrent instability, musculocutaneous nerve palsy, and persistent postoperative pain, ranging from 7.5% to 25%. The indications for performing this procedure are less clear in the setting of subcritical bone loss because the concept of surgically addressing subcritical bone loss is relatively novel and few studies have examined the role of glenoid reconstruction in this specific patient population. Furthermore, there is variability in the definition of what constitutes subcritical bone loss. Yang et al 34 recently published a study comparing remplissage versus the modified Latarjet procedure for Hill-Sachs lesions in patients with subcritical bones. They reported that both surgical options could provide satisfactory results in the general population. However, they reported that the modified Latarjet procedure resulted in improved outcomes in patients with previous instability surgery, collision and contact athletes, and patients with greater than 10% of glenoid bone loss. Additionally, they found that patients who underwent the Latarjet procedure had a higher complication rate.
DeFroda et al 8 reported a case of augmenting Bankart repair with the long head of the biceps tendon, raising the question of whether isolated soft tissue transfer could sufficiently augment shoulder stability in patients with subcritical glenoid loss. The unique feature of their tendon transfer was that in addition to reinforcing the static effect of Bankart repair, it produced a functional sling effect that is comparable with the effect produced by the Bristow-Latarjet procedure. In our study, we demonstrated that the augmentation of Bankart repair with the long head of the biceps tendon is more reliable than the augmentation of Bankart repair with the conjoint tendon and that this repair provides more resistance to anterior displacement of the humeral head than the intact labrum. Therefore, transfer of the long head of the biceps tendon may be indicated in the setting of subcritical bone loss in which further resistance to translation is desired. It should be noted that these supraphysiological resistance values may provide additional utility in the prevention of an “engaging” bony lesion, particularly in the setting of poor patient compliance in which adequate timing for labral healing is not permitted.
This study has several limitations. First, the osseous defect was created by osteotomizing the glenoid, which is an oversimplification of the pattern of glenoid bone loss that occurs in patients with recurrent shoulder instability. However, our methodology allowed us to reproducibly create a specific degree of bone loss in all of the cadaveric specimens included in the study. Second, because of the sequential nature of the study design, the long head of the biceps tendon was sacrificed before mechanical testing of transfer of the conjoint tendon. Therefore, the native anatomy was not used for testing of the conjoint tendon. Third, in vivo shoulder stability relies on a complex interplay between the static and dynamic shoulder stabilizers. Although our model attempted to reproduce the horizontal compression of the humeral head into the glenoid by individually loading the rotator cuff muscles, the long head of the biceps tendon and conjoint tendon, this does not account for the variability of muscle forces encountered during an in vivo instability event. Furthermore, our translation tests were performed with the humeral head in a neutral position, which may not be the position of the humeral head during dislocation. However, this testing methodology has been previously used in similar cadaveric testing, and its limitations have been discussed in prior publications. 27 Fourth, the bone and soft tissue quality of cadaveric shoulders may not represent the tissues found in younger patients who typically present with anterior shoulder instability.
Conclusion
Given the susceptibility of recurrent instability in shoulders with subcritical bone loss after isolated labral repair, it is important to consider augmenting Bankart repair in high-risk patients to avoid potential recurrence and the need for reoperations. Transferring the long head of the biceps tendon to the anterior glenoid represents one possible augmentation.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this project was provided in part by DePuy Synthes. Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award No. P30GM12273 (COBRE Bioengineering Core). S.L.B. has received educational support from Stryker. B.D.O. has received consulting fees from Conmed Linvatec, DuPuy Synthes, and the Musculoskeletal Transplant Foundation; has received research support from Histogenics, Medical Device Business Services, and Vericel; has received publishing royalties from Saunders/Mosby-Elsevier and Springer; and is a paid associate editor for The American Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.