
Abstract
Background:
The anatomy and function of the quadriceps muscle play a role in patellofemoral stability. Few studies have evaluated anatomic differences in the vastus medialis between patients with and without patellar instability.
Purpose:
To compare the anatomy of the vastus medialis using magnetic resonance imaging in patients with patellar instability to a control group.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A group of patients with patellar instability were sex-matched with a control group with anterior cruciate ligament tears, meniscal injuries, or sprains; patients younger than 15 years were excluded. The anatomy of the vastus medialis was examined by the distance between the distal origin of the vastus medialis in the femur and the medial femoral condyle, the distance from the proximal pole of the patella to the most distal insertion of the muscle and its ratio to the length of the articular surface of the patella, and a qualitative description of the insertion position of the muscle fibers (directly in the patella or the medial retinaculum).
Results:
Both groups comprised 78 knees (48 female; 61.5%). The mean age in the control and patellar instability groups was 30.2 ± 7.8 years and 25.6 ± 7.5 years, respectively (P = .001). The distance from the vastus origin to the condyle was 27.52 ± 3.49 mm and 26.59 ± 3.43 mm, respectively (P = .041); the distance from the proximal pole of the patella to the most distal muscle insertion was 17.59 ± 5.54 mm and 15.02 ± 4.18 mm, respectively (P < .001); and the ratio of this distance to the joint surface was 0.586 ± 0.180 and 0.481 ± 0.130, respectively (P < .001). In 75.6% of knees in the patellar instability group, the insertion of the vastus was into the medial retinaculum and not into the patella compared with 52.6% in the control group (P = .003; odds ratio, 2.8).
Conclusion:
The distal insertion of the vastus medialis differed in knees with patellar instability, with a more proximal insertion and less patellar coverage relative to controls, and was more frequently found in the retinaculum instead of directly in the patella.
The stability of the patellofemoral joint depends on both bone and soft tissue structures. The shape of the patella and femoral trochlea, femoral torsion, coronal alignment, and patellar height are the main bony factors responsible for good joint functioning. The main stabilizing soft tissue structures include the quadriceps muscle, medial patellofemoral ligament (MPFL), medial patellotibial ligament, medial patellomeniscal ligament, and medial and lateral retinacula. 6,12,15 Of these structures, the MPFL is considered the most important, and its rupture is cited as an essential injury for lateral dislocation of the patella. 5,6,10
The anatomy and function of the quadriceps muscle play a role in the alignment of the extensor apparatus, and an increased lateral quadriceps vector is a risk factor for patellofemoral pain or patellofemoral instability. 13,14,32 Accordingly, because the anatomic location of the vastus medialis favors restriction to patellar lateralization, this muscle is considered an important dynamic stabilizer of the patella. Its patellar insertion was described to be in the central region of the patella, with the muscle fibers inserting at a 50° angle to the longitudinal patellar alignment. 26 This more distal part of the vastus medialis has received special attention for inserting directly into the patella and merging with the MPFL; it is named the vastus medialis obliquus (VMO), as it has a more tilted anatomy and its own innervation. 8,9,21,23,29
The functional importance of the vastus medialis has been investigated in cadaveric specimens and also in vivo. VMO weakness causes increased patellar lateralization during knee extension 31 and correlates with patellofemoral pain 24 ; changes in its volume occur more frequently in patients with patellofemoral pain syndrome, 19 and decreased and delayed activation of the vastus medialis correlates with increased lateral tilt of the patella in patients with poor alignment of the extensor mechanism. 27,28
The hypothesis that anatomic and/or functional changes in the vastus medialis contribute to patellofemoral disease is worthy of investigation. However, few studies have evaluated anatomic differences in this muscle between patients with patellar instability and controls. 20,22 Knowledge of anatomic variations in different clinical situations is fundamental to define therapeutic strategies for the patellofemoral joint.
The aim of the present study was to compare the anatomy of the vastus medialis using magnetic resonance imaging (MRI) in patients with and without patellar instability. The hypotheses were that the insertion of the vastus medialis in the patellar instability group would be more proximal and more frequently inserted into the retinaculum rather than directly into the patella. In addition, the most distal origin of the vastus in the femur would be more proximal in this group. The hypotheses were based on the theoretical assumptions that in patients with patellar instability, the vastus medialis would be less efficient, end more proximally, lack direct contact with the patella, and be less oblique and more vertical, which would decrease the dynamic medial stabilizing force on the patella.
Methods
This study was approved by the hospital’s ethics committee. Inclusion criteria for MRI scans were the following: diagnosis of patellar instability by one of the senior authors (R.G.G. or B.B.H.), based on history, physical examination findings, and imaging (with at least 1 episode of dislocation) (patellar instability group), or an anterior cruciate ligament injury or medial collateral ligament injury or meniscal injury or sprain without anatomic abnormalities (control group); and skeletal maturity (age 15-50 years). Exclusion criteria were MRI scans with signs of an acute injury that could interfere with patellar or vastus analysis (eg, joint effusion affecting patellar position, severe medial retinaculum edema, or inability to visualize distal vastus insertion) and with degenerative changes (eg, osteoarthritis).
A database was created with 105 MRI scans of patients with documented patellar instability and 109 scans of control patients (with diagnoses of traumatic anterior cruciate ligament or medial collateral ligament injury, meniscal injury, or sprain without injuries) from 2013 to 2018 based on diagnostic data obtained from medical records. Scans of patients with anterior patellofemoral pain without instability were not included because the anatomic risk factors of anterior knee pain overlap with those of patellar instability. None of the scans included in the control group showed concomitant patellar instability. The scans were included according to convenience and availability in our database.
The MRI protocol at our institution consisted of good-quality scans (≥1.5 T) with slices <5 mm in thickness, for which data were available for analysis in HOROS software (open source; allowing measurements as small as 0.01 mm). As the epidemiological profile of the injuries was different, sex matching was performed by statistical analysis software (SPSS v 22; IBM), which excluded 58 scans for which an adequate control could not be found. After growth plate closure, the anatomy does not change significantly until degenerative changes start to occur. Therefore, we decided to only include skeletally mature (15 years and older) patients without osteoarthritis instead of matching patients by age. Thus, 78 examinations were included in the patellar instability group and 78 examinations were included in the control group.
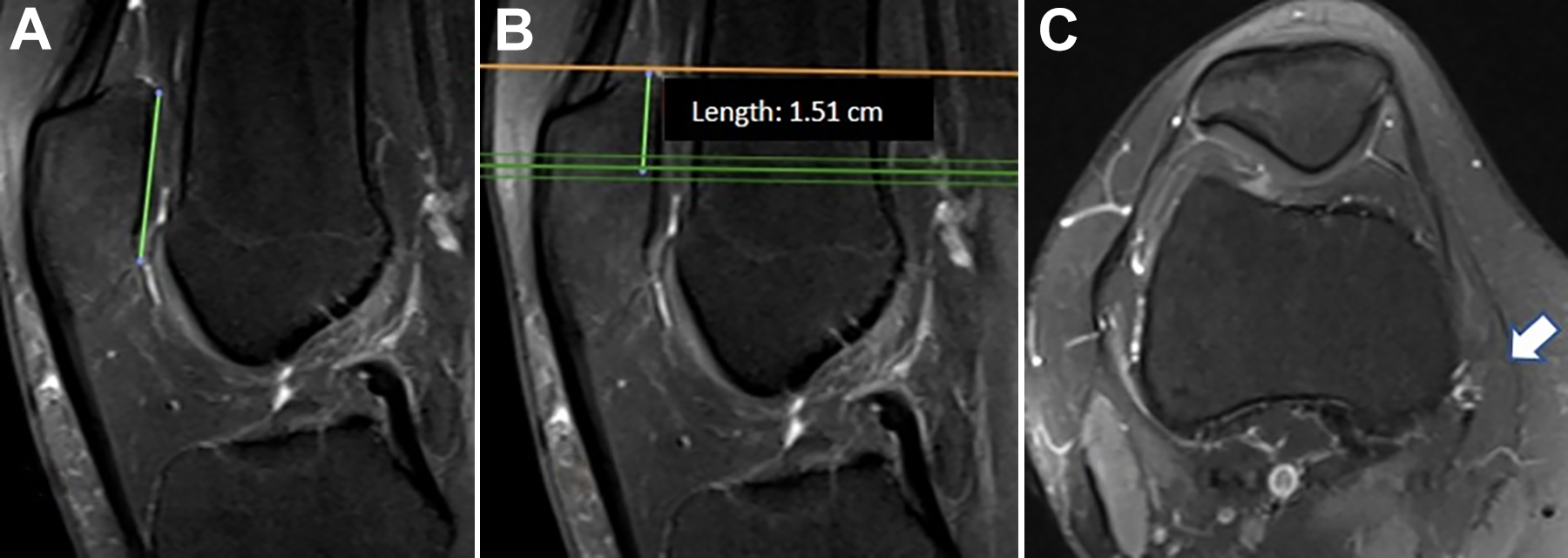
The anatomy of the vastus medialis was studied using the following measurements: Distance from the proximal pole of the patella to the most distal insertion of the muscle fibers of the vastus medialis (linear measurement in the sagittal view using the axial view to visualize the last slice containing muscle fibers from the vastus) (Figure 1). Ratio between (B) the distance on the most distal axial slice (C) with vastus muscle fibers indicated by the arrow to the proximal pole of the patella in relation to (A) the patellar articular surface in a right knee. Vastus/patellar insertion ratio, consisting of the ratio of distance 1 above to the length of the patellar articular surface (measured in the sagittal view with the largest proximal-distal distance of the patellar cartilage) (Figure 1). Qualitative description of the vastus insertion topography, whether directly into the patella (bone) or into the retinaculum (retinacular) evaluated in the axial view: if in the MRI axial images below the patellar upper pole, the vastus muscle fibers reached the patella directly or ended more medially in the retinaculum (Figure 2). Qualitative classification of the vastus insertion (white arrows) directly (A, B) into the patella or (C, D) into the ligament/retinaculum. Distance from the most distal origin of the vastus medialis in the femoral diaphysis to the medial femoral condyle (linear measurement in the sagittal view from the concavity-to-convexity transition of the posterior cartilage of the medial femoral condyle to the most distal point of origin of the vastus medialis in the femoral diaphysis) (Figure 3). This vastus origin–condyle distance intends to represent the direction of the vastus medialis muscle fibers, known to be more oblique in the VMO portion. Longer distances would mean more vertical fibers, which have a smaller medial vector. Vastus origin–condyle distance on a sagittal image from the most distal vastus medialis origin at the femur to the proximal end of the medial condyle cartilage in a right knee.


Statistical Analysis
A paired t test or the Wilcoxon test was used to analyze continuous variables according to their distribution, and the chi-square test was used to analyze categorical variables. Interobserver analysis was performed using the intraclass correlation coefficient (ICC) and kappa statistic for the categorical variables obtained from measurements made by 2 senior authors (R.G.G. and P.R.L.T.) in 30 patients of the series. Intraobserver analysis was not performed because of our experience with the anatomic landmarks used and previous publications with excellent intraobserver results. 13,14 An alpha of 5% was considered significant.
Results
A total of 156 matched scans were included: 78 in the control group and 78 in the patellar instability group. Table 1 shows the age and sex distribution.
Age and Sex Distribution

Both groups had 48 female knees (61.5%). The control group had a mean age of 30.2 ± 7.8 years, and the patellar instability group had a mean age of 25.6 ± 7.5 years (P = .001). In the control and patellar instability groups, respectively, the distance from the proximal pole of the patella to the most distal insertion of the muscle fibers of the vastus medialis was 17.59 ± 5.54 mm and 15.02 ± 4.18 mm (P < .001), and the ratio of this distance to the joint surface was 0.586 ± 0.180 and 0.481 ± 0.130 (P < .001). In 75.6% of the knees in the patellar instability group, the insertion of the vastus was in the retinaculum and not in the patella, compared with 52.6% in the control group (P = .003; odds ratio, 2.8). Finally, the vastus origin–condyle distance was 27.52 ± 3.49 mm in the control group and 26.59 ± 3.43 mm in the patellar instability group (P = .041).
Table 2 shows the results and comparisons between the measurements performed and the interobserver analysis. All measurements had an ICC considered good or excellent except the vastus origin–condyle distance, which was considered fair.
Comparison of Measurements a

a Data are shown as mean ± SD (95% CI) unless otherwise indicated. ICC, intraclass correlation coefficient.
b Odds ratio = 2.8.
Discussion
This study showed a clear anatomic difference in the vastus medialis muscle between patients with and without patellar instability. The quadriceps muscle had a more proximal patellar attachment in patients with instability: on average, 48% of the length of its articular surface (proximal half of the patella) compared with 58% of this length in the control group (distal half of the patella). In addition, the distal attachment of the vastus medialis into the ligamentous/retinacular component rather than directly into the patella, and therefore more medial, was significantly more frequent in knees with instability (75.6% vs 52.6%, respectively). These findings confirm that there is indeed a vastus medialis morphological difference in patients with patellar instability.
Few studies have evaluated anatomic differences of the vastus medialis between patients with patellar instability and controls. In 1992, Koskinen and Kujala 20 published a study with a small sample size of 20 low-quality MRI scans and found that the vastus medialis inserted higher in patients with patellar instability than controls, without affecting the patellar position values. In 2008, Lin et al 22 studied 112 patients with patellofemoral pain syndrome and reported that the cross-sectional area of the vastus medialis was a predictor of poor patellar alignment (tilt and shift). This finding does not confirm muscular dysplasia, only that greater muscle tropism influences patellar positioning. In 2014, Balcarek et al 1 studied 30 patients with acute patellar dislocation, 30 patients with recurrent instability, and 22 controls, comparing the cross-sectional area of the vastus medialis, angulation of its muscle fibers, and craniocaudal extent of the muscle in relation to the patella, and found no difference between groups. However, they measured only the linear distance of the craniocaudal extent of the muscle and not its ratio with the patellar length, as in our study.
The nonlinear or ratio measurements used in this study have not been previously described; they were developed to avoid biases related to patient anthropometry and muscle tropism. Although a significant difference in age was observed between the study groups, this difference has no clinical relevance, considering that only skeletally mature and nonarthritic patients were included. The location of the vastus insertion (whether in the patella or the retinaculum), as well as the ratio between the medial patellar coverage by the muscle and the patellar articular surface, is not influenced by the height or muscular tropism of the patient because these variables do not modify the position of the vastus in relation to the patella. Thus, we believe that the differences found should be valued, even without controlling for height, weight, and muscle strength, and that the ratio between the muscle and patella should be more valued than the linear measurement of the muscle, although this was also significantly different between groups. Although the absolute differences were small (∼2 mm), they are not within the measurement error because the software allows 0.01 mm of precision. The only linear variable analyzed, the vastus origin–condyle distance, was developed as a method to assess the obliquity of the vastus fibers, as larger distances would reflect a more proximal origin of the vastus medialis in the femur and a more vertical vector (as opposed to a more medial vector with higher obliquity). The result of this measurement was not relevant because, although significantly different, its magnitude was very small and its interobserver correlation was the lowest, reflecting the difficulty in obtaining it; in addition, the noncontrolled size of the patient sample may have influenced the measurement.
The vastus insertion site, whether directly into the patella or the retinaculum, was significantly different between groups (P = .003), with an odds ratio of 2.8 for the patellar instability group if the insertion was in the retinaculum/ligament. These data are clinically relevant because a more lateral (in the patella) distal insertion of the vastus results in a greater medialization vector of the muscle during its contraction.
Protocols for isolated VMO activation have been used to treat pain and patellofemoral instability, despite conflicting evidence regarding their efficacy. As an example, Hyong and Kang 17 showed that it is possible to favor activation of the vastus medialis in relation to the vastus lateralis using unstable surfaces for squats. Therefore, it is necessary to improve understanding of the relationship between the vastus medialis and patellar instability because this muscle can be a specific target of therapies. This issue is further complicated by the existence of studies questioning the importance of the vastus medialis, such as that of Peeler et al, 30 who found no anatomic basis in cadaveric specimens for the vastus medialis to function as a stabilizer of the medial patella. Although our study does not address function, patients with a greater vastus/patellar insertion ratio and with muscle fibers directly touching the patella may have a better medialization vector of the extensor mechanism and may respond better to rehabilitation and muscle strengthening programs. This requires further investigation.
In the treatment of patellar instability, advancement of the vastus medialis was widely used before the recognition of risk factors for patellar instability and the introduction of ligament reconstruction, especially of the MPFL. 2–4,7,11,16,18,34,35 When performed with exaggerated lateralization and distalization and combined with lateral retinacular release, as described by Insall et al, 18 the procedure provides patellar stabilization but may lead to increased joint pressure, tightening of the MPFL, and early degeneration. 3,18,25,33,35,36 Reconstruction of the MPFL and correction of risk factors have a high success rate in patellar stabilization and a lower risk of developing arthrosis; thus, transfer of the insertion of the vastus medialis was practically abandoned. However, recognition of the insertion abnormality of the vastus medialis in patients with patellar instability in the present study suggests that this is part of the pathophysiology of the disease. Thus, during surgical treatment, the insertion of the vastus medialis should not be neglected and inadvertently damaged. Additionally, in cases where it is necessary to remove the vastus medialis for reconstruction of the MPFL, the muscle should be adequately repaired at the end of the procedure. Another point for future consideration is normalization of the insertion of the vastus medialis through its distalization to below half the chondral surface of the patella and its advancement to the bony edge of the patella, as suggested by the present study. Again, normalization differs from the excessive lateralization described by Insall et al, 18 thus avoiding an excessively increased load on the patellofemoral joint and preventing increased arthrosis of the patellofemoral joint.
Limitations
One of the limitations of the present study was not assessing the impact of the vastus medialis measurements on patellar positioning. We consider this study an initial step in anatomic understanding of this structure, and therefore, we did not measure or control for all variables that affect patellar positioning, such as patellar height and trochlear dysplasia. Thus, we cannot attribute clinical relevance to the difference found, and this analysis is pending for future studies. Another limitation is that MRI was performed after dislocation of the patella; therefore, we cannot determine whether the change in the vastus medialis is the cause or consequence of the dislocation. However, as this is a case-control study, this limitation could not be avoided. Finally, the MRI-based parameters utilized in the study, although very easy to achieve and with good to excellent ICCs, have not been validated before, the patient sample size was not controlled, and no intraobserver analysis was performed.
Conclusion
Compared with that in controls, the distal insertion of the vastus medialis differed significantly in patients with patellar instability, with a more proximal insertion, less patellar articular surface coverage, and more frequent insertion of the muscle fibers into the retinaculum instead of directly into the patella.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (CAEE: 78967517.0.0000.0068).