
Abstract
Purpose:
The aim of this study was to evaluate the results of patients with recurrent anterior shoulder dislocation, who had been treated with repair of the Bankart lesion without capsuler plication.
Material and method:
The study included 22 shoulders of 22 patients (16 males and 6 females) with a mean age of 28 years, who underwent Bankart repair between 2011 and 2014. Patients with bilateral shoulder instability, multiple instability, >25% glenoid bone loss, and those with a history of shoulder surgery were not included in the study. The average follow-up time was 21.2 months. Evaluation was made of the preoperative number of dislocations, postoperative recurrence, functional status, and daily activity performance of the patients. Shoulder range of motion was measured. The results were evaluated using the Rowe shoulder score and the Oxford shoulder instability score.
Results:
Recurrence was observed in only one patient who had a shoulder dislocation after trauma, thus giving a recurrence rate of 4.5%. Shoulder range of motion was full in all except that one patient. The mean Rowe shoulder score was 95.5 (excellent) and Oxford shoulder stability score was 44.6 (excellent).
Conclusion:
No recurrent shoulder dislocation was observed in patients who underwent Bankart repair surgery. Plication was not performed with the Bankart repair. Close to full range of motion was obtained in all patients. In conclusion, Bankart repair alone can be considered to be sufficient for the treatment of traumatic recurrent anterior shoulder instability.
Introduction
The glenohumeral joint has the most extensive range of movement of any joint in the body. It is one of the most active joints in the body and because of its role in the protective reflex of the body, it is often injured. Shoulder dislocations comprise approximately 50% of all joint dislocations and more than 90% of these dislocations are anterior. The stability of the shoulder joint depends on static and dynamic soft tissue structures such as the labrum, the glenohumeral ligaments, and the rotator cuff. 1
The most important factor affecting the treatment success in a patient with shoulder dislocation is recurrence of dislocation after treatment. It is thought that in surgical treatment, in addition to Bankart repair, which is one of the pathologies thought to cause dislocation, a more than necessary amount of capsular plication and capsular shift reduces the internal volume of the joint. 2,3 Surgical options to reduce the capsular volume include open capsular shift and plication, arthroscopically capsular plication, and thermal capsulorrhaphy. 2,4,5 The open anteroinferior capsular shift-plication involves incising, overlapping, and suturing the capsule to reduce redundancy. Arthroscopic techniques include the thermal capsulorrhaphy and the arthroscopic version of the open capsular shift-plication procedure. Thermal capsulorrhaphy termed thermal capsular shrinkage and was done with the use of a laser or with a monopolar radiofrequency. These procedures had high failure rates due to rebound ligament stretching. 4 Arthroscopic capsular shift procedures that use capsular plication have also been developed to mimic the gold-standard open procedure. Techniques vary, with the use of different suture or tack applications, plication and pleating variations, humeral- or glenoid-based shifts, direction of approach, and posterior pinch-tuck methods. 4 A synovial rasp is used to lightly abrade the synovium overlying the posterior and inferior capsule and along the capsular aspect of the glenoid labrum. Care is taken not to violate the integrity of the capsule with hooks and a special type of stiches. A 1-cm plication fold between the capsule and labrum was created. The sutures are tied to close the capsular fold together and reduce the capsular volume.
The aim of this study was to evaluate the results of patients with recurrent anterior glenohumeral dislocation, who had been treated for the main pathology of Bankart lesion without the application of capsular plication.
Material and method
Approval for the study was granted by the Clinical Research Ethics Committee; decision no 226, dated 23 September 2014.
The study included 22 patients who had arthroscopic Bankart repair for traumatic recurrent anterior shoulder dislocation applied by a single surgeon (CZE) in our clinic between 2011 and 2014. Exclusion criteria were bilateral shoulder instability, more than 25% glenoid bone loss, multidirectional instability, or previous surgery. The patients comprised 6 (27.2%) females and 16 (72.8%) males with a mean age of 28 years (range, 16–49 years). The mean age at first dislocation was 22.8 years (range, 15–40 years). Pathology was observed in the right shoulder in 16 (72.8%) cases and in the left shoulder in 6 cases (27.2%), and of these the involvement was on the dominant side in 16 cases (72.8%).
In all the cases, the shoulder dislocation was traumatic and the mechanism of trauma was most often activities such as a fall (13 patients), a collision while playing football (8 patients), or fighting (1 patient). The mean preoperative duration of the complaints was 67.6 months (range, 10–192 months). Between 1 and 10 previous dislocations were determined in 12 cases, between 11 and 20 in 1 and more than 20 in 9 cases. No patient had undergone surgery after the first dislocation. In the preoperative examinations, the apprehension test was positive in all cases. Preoperative evaluation of all cases was made with direct radiographs and magnetic resonance imaging. In all the patients, labral separation was determined. A Hills–Sachs lesion was determined in 19 cases and Humeral Avulsion Glenohumeral Ligament (HAGL) lesion in 1 case. Intervention for Hills–Sachs and HAGL lesions was not made in any case.
Surgery was applied with the patient in the beach chair position under general anaesthesia. Arthroscopy was applied using the standard portals. Regardless of the trauma etiology and number of dislocations, only capsulolabral repair was applied to all the patients and capsular plication was not made in any case. The same surgeon (CZE) performed all the operations with the same standard technique in acccordance with these principles. Before the repair, the glenoid neck was decortisized with reaming and shaving. The first suture hook was routinely placed over the glenoid just at the edge of the joint cartilage at the level of 5 o’clock. Then additional suture hooks were placed at the glenoid border in the positions of 4 o’clock, 3 o’clock, and sometimes 2 o’clock.
On postperative day 1, the arm sling was removed and pendular shoulder movements were started. The patient was instructed to repeat these movements daily as far as tolerated. At other times, the arm sling was worn for 2 weeks. After 2 weeks, passive shoulder exercises were started to obtain shoulder range of movement and it was permitted to use the arm for simple daily activities (e.g. eating and drinking). Strengthening exercises were not started until 2 months postoperatively. Sporting activities could recommence after 3 months but it was recommended to avoid contact sports and activites for 6 months.
With the shoulder in 90° abduction, the internal and external ranges of movement angles were measured. At the same time, anterior elevation and abduction range of movement angles were also measured. At the postoperative follow-up examinations, two shoulder evaluation systems were used. The subjective feeling of subluxation or documented full dislocation was evaluated as recurrence of instability.
Range-of-motion (ROM) measurements, satisfaction scores, return to previous level of activity, and rate of recurrence, Rowe score, and Oxford shoulder stability score were measured. Return to the previous activity level and rate of recurrence were evaluated. These results also were compared with the other results in the literature (Table 1).
Comparison of studies.
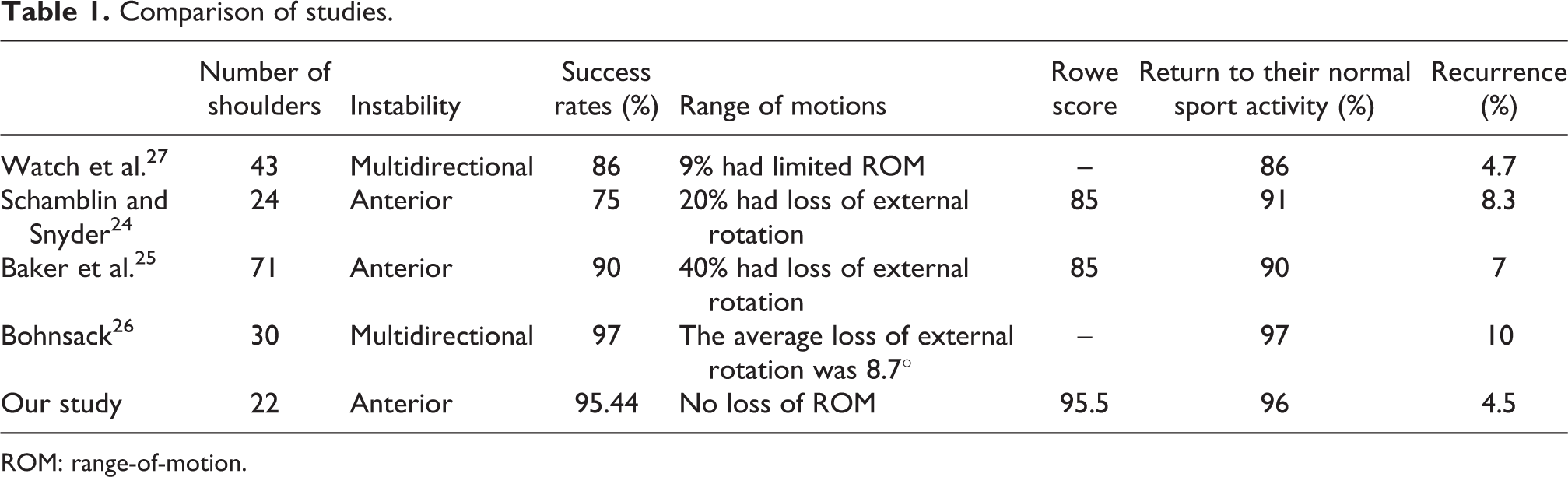
ROM: range-of-motion.
Results
The general data of the patients are shown in Table 2. The mean follow-up period was 30.3 months (range, 25–48 months). Postoperatively, dislocation occurred in only one patient as a result of trauma. The recurrence rate was determined as 4.5%, which was not significantly different from the other studies (Table 1). The mean time to return to work or school postoperatively was 35.5 days (range, 20–75 days).
The general data of the patients.

aDislocation developed following trauma and bone Bankart lesion developed.
On the Rowe shoulder instability scale, 21 (95.4%) patients were evaluated as excellent and 1 (4.6%) patient as poor. In 16 (72.7%) of 22 patients, no limitation of movement was determined, slight limitation in 5 (22.7%) patients, a moderate level in 1 (4.6%), and no significant limitation in any patient. The average Rowe score of our study was similar to other studies (Table 1).
According to the Oxford shoulder instability scale, the mean score of patients was 44.6 (range, 32–48). The results of 20 patients were evaluated as excellent and of 1 patient as good.
Of the 21 patients for whom final examination could be made, no limitation was determined in the external rotation, anterior elevation, or abduction movement of 21/22 patients when compared with the contralateral side. In one patient limitation was found of 15° in external rotation, 10° in abduction, and 20° in anterior elevation (Figure 1).

The patient with limitation in shoulder range of motion.
The mean number of suture hooks used in the patients was determined as 3 (range, 2–4).
Discussion
Arthroscopic Bankart repair has been modified by surgeons. Many methods have been applied in addition to the procedure for the labral damage, such as anterior and posterior capsular plication, closure of the rotator interval or thermal capsular shrinkage. 6 Bankart repair, also known as anatomic repair, is currently the treatment of choice according to various surveys of surgeons, with more than 90% of surgeon choosing the Bankart procedure as initial repair for recurrent instability. 6
It is well known that it is important for the static and dynamic stabilizing factors to work in balance for the stability of the glenohumeral joint. An imbalance in this relationship causes instability. Any defect in the proprioceptive structure in this area is also significant in glenohumeral instability. 7
Bankart lesion is accepted as a basic pathology in recurrent shoulder dislocations. The basis of the Bankart lesion was defined as “the separation of the capsule from the fibrocartilaginous glenoid ligaments.” As a result, the labrum is separated from the glenoid edge and there is a loss of tension in the inferior glenohumeral ligaments. Thus the anteroinferior glenohumeral ligaments attached to the labrum separate from the glenoid edge and functions are disrupted. 8 –12
In 1909, Thomas 13 reported that the lesion causing glenohumeral dislocation was a tear in the capsule. Controlled dislocations were formed in cadaver studies and the anteroinferior capsule was seen to be torn. The conclusion was reached that for a recurrent anterior dislocation of the shoulder, “a hernial sac is formed anterior to the capsule and therefore, the aim of the treatment should be the repair of this sac.” Surgery including a decrease in the capsule was reported to be sufficient.
The capsular mechanism was defined by Townley. 14 Loss of the anterior bumper effect of the capsule allows for abnormal anterior translation of the humerus head. 14 The anterior barrier effect of the labrum has been reported to be very small. Therefore, surgical repair of the Bankart lesion as described has been reported to be excellent. 14 It has long been a matter of unresolved debate as to how the lesion is the basis of instability or if there is perhaps a more important lesion in the basis of instability. A study conducted in 1992 made a great contribution to the understanding of the pathology of shoulder instability. 15 The inferior glenohumeral ligament was cut from three anatomic regions and tested for tension failure on a single axis. In the Bankart lesion (cut from the glenoid attachment point of the capsule), failure developed in 40% of the samples. In those cut from the center of the capsule, the failure rate was determined as 35% and in those taken from the humerus head attachment point, 25%.
In a study by Bigliani et al., 16 plastic deformation of the capsule was defined and it was reported that the failure had formed with a significant extending of the inferior glenohumeral ligament. Thus, arthroscopic evaluation of capsular tension is difficult. Surgical intervention is recommended for all related patho-anatomic problems. 7
Several new techniques have been defined related to the emergence of these problems. Laser capsulorraphy has been used to stretch the capsule, but there is a risk of necrosis. Radiofrequency temperature probes are used for capsular stretching. 7
There are also cadaver studies that have reported that capsule plication is an effective method in reducing the glenohumeral joint internal volume. 17 However, it is not fully known by how much the joint volume should be reduced to remove the instability in these patients with shoulder instability because of capsular laxity. It can therefore be assumed that because of the likelihood of healing characteristics being different in each patient, the tissue response to plication may not be able to be fully predicted. In addition, as advanced experience is required to achieve the appropriate tissue tension, the learning curve is extremely long and no objective measurements have been defined as yet. There is a need for more scientific research on this subject. In a study by Chiang et al., 18 posteroinferior capsular plication was applied and the rotator interval was closed in 45 patients and at the end of a 5-year follow-up period, significant restriction was determined in shoulder movement. The dislocation recurrence rate was found to be 6.6%. Recurrence and revision rates of the arthroscopic Bankart repair were found to be 6 and 4.7%, respectively, in a study. 19 In the past, recurrent instability was often the consequence of capsular redundancy because of ineffective hardware. With modern suture anchors, capsular plication could be done more effectively during the arthroscopic repair. The recurrence rate decreased from 4% to 17%. 5
There are also studies stating that there is restricted shoulder joint movement in patients who have undergone capsular plication. In a biometric study by Shafer et al. in 2008, 20 anterior plication was applied to patients and in the measurements made at 0° and at 60° abduction, a reduction in external rotation was determined. In the same study, in patients to whom only plication had been applied, an increase was determined in glenohumeral translation. In another biometric study by Alberta et al. in 2013, 17 a significant reduction in external rotation was determined after plication was applied to cadavers. Westerheide et al. 21 applied plication additional to labral repair in 71 cases and reported a recurrence rate of 7%. It was also determined that shoulder joint range of movement had decreased by 25% compared to the unaffected shoulder in 40% of patients.
Another important point is that in several studies, the shoulder joint range of movement has not been compared with the contralateral healthy shoulder but the results have been the comparison of pre and postoperative values. The pre and postoperative shoulder joint range of movement angles may be the same as the preoperative fear of dislocation restricts external rotation. Therefore, the comparison must be with the pre and postoperative values of the healthy shoulder as it is necessary to determine the extent of the restriction in the normal values. Lee et al. 22 applied capsular plication to 75 cases and it was concluded that in these patients with preoperative mean shoulder external rotation value of 78.1, at the 3rd and 6th months postoperatively there was a reduction in external rotation and only at the 24th month postoperatively was the preoperative level regained. If there is no problem in the other shoulder, there will be seen to be a loss of external rotation of mean 13.4%. In the current study, with the exception of one patient, the joint range of movement was measured as full in comparison with the healthy shoulder.
We searched the PubMed, the Cochrane Library, and Ovid/MEDLINE for articles published from 2000 through 2014 on surgical procedures to treat shoulder instability. Search terms were shoulder capsular plication, shoulder capsular shift, shoulder capsular shrinkage, thermal capsulorrhaphy, and shoulder instability. Cohort studies, multiple case reviews, and randomized controlled trials were included. Only studies that specifically investigated the outcomes of arthroscopic capsular shift through plication and thermal capsularrhaphy were eligible.
We compared studies based on outcome measures such as ROM measurements, satisfaction scores, return to previous level of activity, and rate of recurrence. Outcome measurements were also compared with Rowe score and Oxford shoulder stability score. Return to the previous activity level and rate of recurrence were the most common measurements to determine the success rates. These measurements were also compared with results of our study (Table 1). Kim et al. 23 applied capsular plication for the treatment of 24 shoulders with anterior glenohumeral instability. The average loss of external rotation was 20%. The average Rowe score improved from 30 to 85. All patients returned to their normal work and activities. However, only four of these (17%) returned to their work and activities with no limitations, and six (25%) returned with moderate limitations. 23
Westerheide et al. 21 treated 71 patients with Bankart repair and capsular plication for anterior instability. Sixty percent of these patients had full range of motion. Ninety percent of these patients returned to their previous level of sports, 40% continued to exhibit mild-moderate apprehension. The average final Rowe score was 85. 21 In two studies, 24,25 capsular plication was applied to patients that had multidirectional instability of the shoulder. The success rate was 86 and 97%.
An arthroscopic capsular shift with sutures alone does not appear to increase glenohumeral stability and also result in significant decreases in primary external rotation in abduction. 26
Postoperative recurrence of shoulder dislocation is evaluated as treatment failure. In previous studies, recurrence rates have been published ranging from 4% to 17%. In the current study, dislocation occurred in only one patient, the cause of which was a fall. The recurrence rate was determined as 4.5%, which was determined as a lower level than most of the reports in literature. In literature, there are some studies to treat the patients with a Bankart repair and capsular plications. The recurrence rate in the studies was between 4.7% and 10%. 21,23 –25
Previous studies have shown that the number of suture hooks used during the operation could affect the result. In a study by Watch et al., 27 it was suggested that the use of fewer than four suture hooks could have been one of the reasons for failure. In another study by Witney-Lagen et al., in 2014, 28 after a 4-year follow-up period of 114 patients, it was reported that stability had been achieved with the use of fewer than three suture anchors and that even one anchor may be sufficient. In the current study, a mean of three suture anchors was used. Data from the trails showed that patients operated using two anchors had a higher incidence of recurrence instability (35%) compared to patients operated using three or more anchors (20%). 5 In the patient in whom postoperative dislocation developed, four suture anchors were used.
A vital feature in assessing any operative intervension is patient satisfaction. The common tool used in the majority of the studies was the Rowe score, which look stability, function, and motion. 6
The limitations of the current study can be said to be that there was no comparison of the patients to whom plication was applied, the preoperative evaluation was insufficient, the number of patients evaluated was low, and the average follow-up period was short. More patients and a longer follow-up period are required to confirm our finding.
Generally, the recommended treatment in recurring traumatic anterior shoulder dislocations is the repair of the Bankart lesion, which is accepted as the primary pathology and in addition capsular shift and plication. However, it is difficult to decide on the degree of capsular plication during the operation and if excessive plication is applied, it will cause restriction in the joint range of movement.
From the results of this study, it can be considered that treatment directed at the lesion only will be sufficient in patients with anterior glenohumeral instability. It can also be thought that just as the application of additional procedures of capsular plication or closure of the rotator interval could cause a restriction in shoulder movements, there is no additional contribution to reduction in recurrence and this is shown by the results of this current study.
Conclusion
The results of this study determined that in patients with repair of the Bankart lesion as the main pathology, there was no recurrence of the dislocation. Therefore, Bankart repair without capsular plication may be determined to be sufficient in the prevention of dislocation recurrence.
In conclusion, it can be said that in patients with involuntary recurring traumatic anterior glenohumeral instability, the application of Bakart repair alone without plication could be sufficient.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.