
Abstract
Background:
As the indications for reverse total shoulder arthroplasty (RTSA) have continued to expand, the average age of patients undergoing RTSA has decreased.
Purpose/Hypothesis:
The purpose of this study was to report the minimum 2-year outcomes after RTSA and to evaluate the impact of surgical variables on outcomes. We hypothesized that younger patients, patients with larger glenosphere, and patients with irreparable subscapularis tendons would experience worse subjective patient-reported outcome scores (PROS) and that younger patients and those with a reparable subscapularis would demonstrate a higher rate of return to recreational sports activities.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent RTSA by a single surgeon between November 2005 and September 2014 were considered for this study. Patient characteristics, surgical details, PROS, and rates of return to recreational sports activity were prospectively collected and retrospectively reviewed. We assessed correlations between PROS and both patient age and subscapularis reparability. PROS collected included the American Shoulder and Elbow Surgeons (ASES) score, Short Form 12 (SF-12), Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score, Single Assessment Numeric Evaluation (SANE), and postoperative patient satisfaction.
Results:
A total of 110 patients with an average age of 68.0 years (range, 45-87 years) were included. Minimum 2-year follow-up was obtained in 94 patients (85.4%), with a mean follow-up of 3.6 years (range, 2.0-9.3 years). The subscapularis was reparable in 58 patients (57.4%). All PROS significantly improved from pre- to postoperatively (P < .001). The median patient postoperative satisfaction was 9 out of 10 (range, 1-10). Increasing patient age was correlated with significant improvements in QuickDASH and ASES scores. Postoperatively, 76.1% (67/88) of patients were able to return to recreational sports activity. However, of those who did return, 68.2% indicated that they had to modify their activity in some way. Glenosphere size was not significantly associated with PROS or the rate of return to recreational sports activity, but patients with reparable subscapularis tendons demonstrated higher PROS and return to activity rates.
Conclusion:
Patients who had a reparable subscapularis tendon showed a significantly higher rate of return to recreational sports activity than patients who had a irreparable subscapularis tendon. Older age was correlated with greater improvement in several, although not all, patient-reported outcome measures. Glenosphere size was not significantly associated with higher PROS or rate of return to recreational sports activity.
Keywords
Since the introduction of reverse total shoulder arthroplasty (RTSA) in 2003 to the US market for patients with severe cuff tear arthropathy, the use of these prostheses has continued to increase. 4,9,11,19 This has resulted from predominantly positive reported outcomes coupled with expanding indications. 18 Indications for RTSA now include rotator cuff tear arthropathy, irreparable rotator cuff tears without arthrosis, irreparable or complex proximal humerus fractures, failed hemiarthroplasty, and revision of failed total shoulder arthroplasty, all of which are occurring in an increasingly younger patient cohort. 5,15 As a result, reverse prostheses accounted for nearly half of all total shoulder arthroplasties performed in 2011. 19
With increased use and an expanding demographic, there is increasing interest in measuring functional outcomes after RTSA. A number of studies have linked patient satisfaction after shoulder arthroplasty with the ability to resume sport and other recreational sports activities. 5,24 However, patients’ desires to return to recreational sports activities after shoulder arthroplasty do not always align with surgeons’ recommendations. This is in part attributable to the lack of clarity regarding the role of age on postoperative outcomes. 9,10,15 Data on return to recreational sports activity after RTSA could potentially be more valuable in a younger, more active cohort, under 65 years of age, which has been largely unexplored. Other surgical factors that may affect subjective outcomes and return to sporting activity are glenosphere size and subscapularis reparability. 2,3,8,16,22
The purpose of this study was to report the minimum 2-year outcomes after RTSA and to evaluate the impact of age, glenosphere size, and subscapularis reparability on outcomes, including the rate of return to recreational sports activity. We hypothesized that younger patients, those with larger glenosphere, and those with irreparable subscapularis tendons would experience worse subjective postoperative outcome scores and that younger patients and those with a reparable subscapularis would demonstrate a higher rate of return to recreational sports.
Methods
Study Population
This was an institutional review board–approved, evidence level 3 retrospective study using prospectively collected data from a single surgeon series (P.J.M.). Patients were included in this study if they (1) underwent implantation of primary RTSA and (2) were at least 2 years out from surgery. Patients were excluded if they refused to participate, died during the follow-up period, or required glenoid structural allograft reconstruction. Surgical data collected included patient age, size of glenosphere implanted, and subscapularis reparability. Preoperatively and at a minimum of 2 years postoperatively, patients completed evaluations using a questionnaire that included several patient-reported outcome scores (PROS): the American Shoulder and Elbow Surgeons (ASES) score, Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score, Single Assessment Numeric Evaluation (SANE), Short Form 12 Physical Component Summary (SF-12 PCS), and postoperative satisfaction (10-point scale, where 1 = highly unsatisfied and 10 = highly satisfied). Additional questions assessed patients’ participation in recreational sports activity, both preoperatively and postoperatively. Patients were asked to evaluate their functional ability to perform usual sports as “unable,” “very difficult,” “somewhat difficult,” or “normal.” For analysis, the data were dichotomized: “normal” and “somewhat difficult” were defined as return to recreational sports activity. We also evaluated clinical failure, defined as revision RTSA, and complication rates. Postoperative PROS were compared between glenosphere size (38 vs 42 mm), subscapularis reparability, and patient age.
Surgical Technique
All patients underwent the same surgical treatment by the senior surgeon (P.J.M.). For all patients, a Grammont-style RTSA was used. All operations were performed with the patient in the beach-chair position under general anesthesia combined with an interscalene nerve block. Following a standard deltopectoral approach, a biceps tenodesis was performed, if biceps tendon was present, proximal to the pectoralis major tendon, and the subscapularis tendon was peeled from its insertion on the lesser tuberosity. If necessary, a capsular contracture release was performed. The humeral head was then exposed, and an osteotomy was performed with an oscillating saw while protecting any residual rotator cuff. Subsequently, the glenoid was exposed, and osteophytes were removed along with the remainder of the biceps tendon and degenerative glenoid labrum. A guide pin was placed into the center of the glenoid and subsequently reamed. The baseplate was then placed and secured with locking and cortical screws, followed by insertion of the glenosphere. The goal was to have the glenosphere translated inferiorly with 2 mm of inferior overhang and also tilted approximately 10° inferiorly in the coronal plane. After the glenoid was completed, the humerus was reamed and broached. The optimal stem size was selected and placed through use of a cementless technique with an appropriately sized polyethylene liner. For all patients, the neck-shaft angle was 155°. Version was set so that the humeral head was concentrically reduced on the glenosphere when the forearm was in neutral rotation. After range of motion and stability were assessed, the shoulder was copiously lavaged, and the subscapularis was repaired in patients where adequate tissue remained. When the subscapularis was of poor quality, it was resected. Finally, the deltopectoral interval was closed in a layered fashion.
Postoperative Rehabilitation
Postoperative rehabilitation permitted immediate passive range of motion. In cases where the subscapularis tendon was repaired, external rotation was limited to 30° for the first 3 weeks. After that point, full active and active-assisted range of motion was permitted. After physician clearance, patients were not given restrictions on types of recreational or sporting activity.
Statistical Analysis
All statistical analyses were performed with SPSS version 11.0 (SPSS). Statistical power was considered with respect to detectable effect sizes between subgroups given a fixed sample size. Assuming 2-tailed comparison of group means and an alpha level of .05, a sample of 115 subjects is sufficient to detect an effect size of d = 0.53 for a 1:1 subgroup allocation ratio or d = 0.61 for a 3:1 subgroup allocation ratio with 80% statistical power. In this dataset, continuous variables were nonnormally distributed. The pre- and postoperative PROS of the entire study population were compared by use of a Wilcoxon signed-rank test. A Mann-Whitney U test for continuous variables was used to assess the differences in PROS between ages ≥65 versus <65 years, glenosphere size 38 versus 42 mm, and subscapularis reparability. Correlations between 2 continuous scales were assessed with Pearson correlation for normally distributed variables (age, postoperative SF-12 PCS, and QuickDASH scores); a Spearman rho analysis was used for postoperative ASES, SANE, and satisfaction scores for monotonic association. The level of significance was set at P < .05.
Results
Between November 2005 and September 2014, the senior surgeon performed RTSA on 119 patients (Figure 1). Of these, 4 patients refused to participate in the study, 4 patients died before final follow-up, and 1 patient required a structural glenoid allograft reconstruction, thereby leaving an initial population of 110 patients. A further 16 patients were lost to follow-up; thus, a minimum 2-year follow-up was obtained in 94 patients (85.4%), with a mean follow-up of 3.6 years (range, 2.0-9.3 years) and an average age of 68.0 years (range, 45-87 years) at the time of index surgery. Of the 68 patients with preoperative magnetic resonance imaging (MRI) scans available for review, 58 had irreparable supraspinatus tendons, and 66 of the 68 (97%) had infraspinatus tendon tears as well. The teres minor was intact in all patients. Hamada grades were calculated for all patients who had not undergone a prior ipsilateral shoulder arthroplasty; they were grade 1 in 20 patients, grade 2 in 3 patients, grade 4a in 4 patients, grade 5d in 5 patients, and grade 6 in 6 patients. Hamada grade was significantly negatively correlated with preoperative external rotation (rho = –0.373; P < .001).
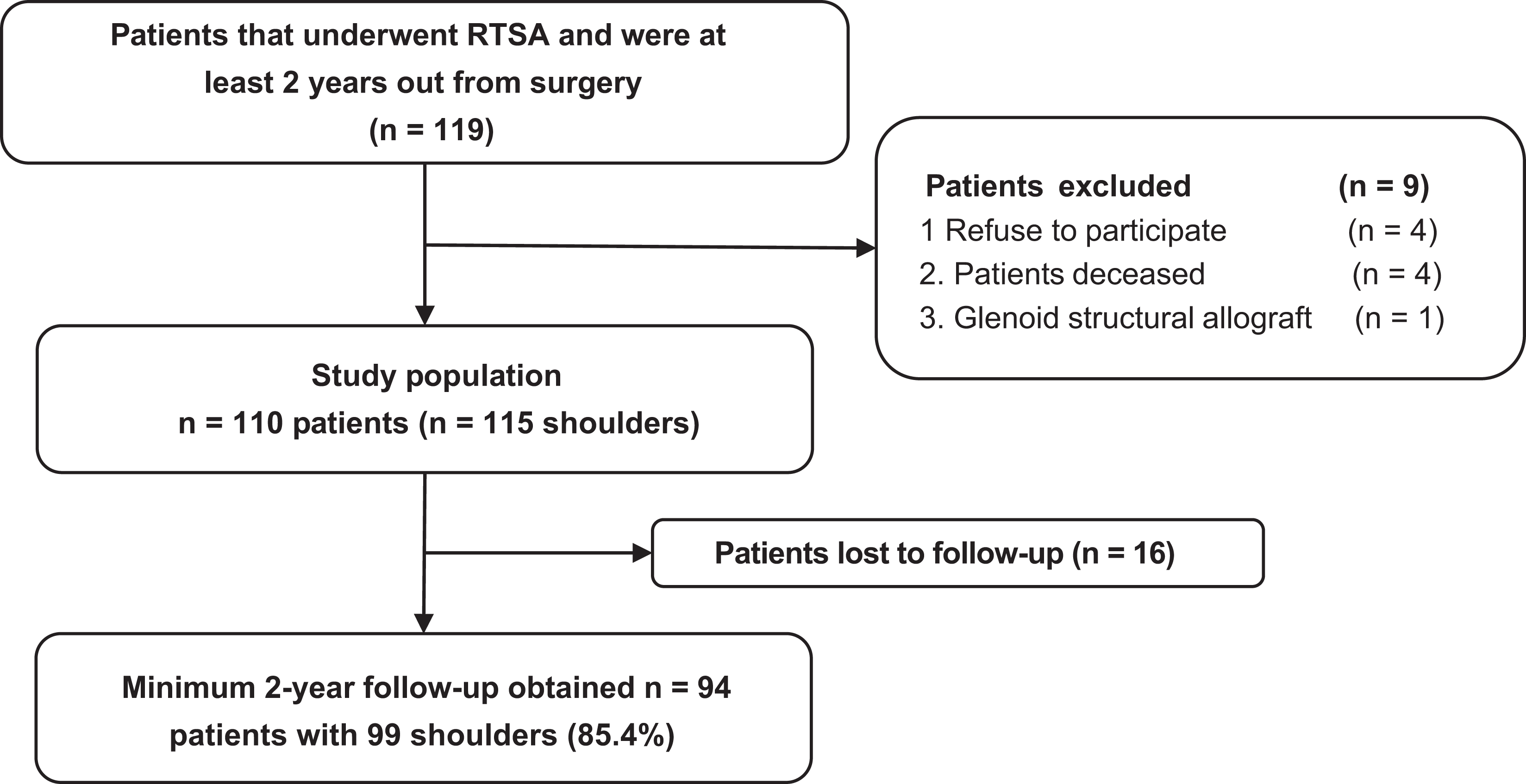
Flowchart illustrating the patient population for this study after application of inclusion and exclusion criteria and allowing for patients lost to follow-up. RTSA, reverse total shoulder arthroplasty.
Glenosphere size was selected intraoperatively based on patients’ body and glenoid size. The most commonly implanted glenosphere size was 38 mm (range, 36-42 mm). A total of 58 (50.0%) of the subscapularis tendons were reparable (Table 1). No significant association was found between age (P = .279) or sex (P = .537) and subscapularis reparability. A total of 7 patients (7.4%) of the 94 patients with a minimum 2-year follow-up ultimately required revision RTSA and were considered clinical failures. A further 2 patients (2.1%) experienced postoperative complications but did not progress to revision RTSA. The first patient experienced an acromial stress fracture and underwent open reduction and internal fixation surgery, and the second patient experienced postoperative shoulder pain necessitating arthroscopic debridement, distal clavicle excision, and suprascapular nerve release.
Subscapularis Tendon Reparability by Underlying Shoulder Diagnosis a

a Values are numbers of shoulders. State of the subscapularis was not determined in 14 shoulders.
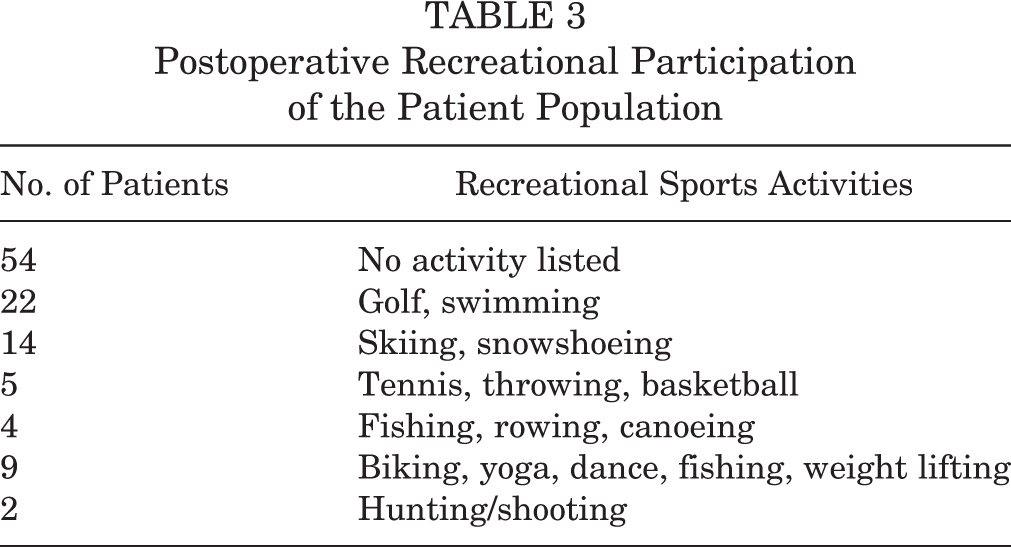
All outcome scores significantly improved from pre- to postoperatively (P < .001) (Table 2). Median patient postoperative satisfaction was 9 out of 10 (range, 1-10). Postoperatively, 35.9% of patients described return to recreational sports activity as “normal,” 38% as “somewhat difficult,” 9.8% as “very difficult,” and 16.3% as “unable” (Figure 2). The recreational sports activities in which patients participated are listed in Table 3, with the most common sport being golf.
Preoperative Versus Postoperative Patient-Reported Outcome Scores for the Study Population a

a Continuous data are presented as median (range). ASES, American Shoulder and Elbow Surgeons score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand score; SANE, Single Assessment Numeric Evaluation; SF-12 PCS, Short Form 12 Physical Component Summary; VAS, visual analog scale.
b Statistically significant difference between groups.

Graphical representation of the pre- and postoperative ability of patients to participate in recreational sports activity.
Postoperative Recreational Participation of the Patient Population
When postoperative PROS were compared by age as a continuous variable, QuickDASH (r = –.308; P = .002) was significantly negatively correlated, and ASES (rho = .280; P = .006) was positively correlated with increasing age. SF-12 PCS, SANE, and patient satisfaction were not significantly correlated with patient age. The size of the glenosphere had no significant association with postoperative PROS or the rate of return to recreational sports activity. Specifically, no difference in PROS was seen when glenosphere size 38 mm was compared with 42 mm (Table 4). Meanwhile, PROS and the rate of return to recreational sports activity were significantly higher (P = .006) in patients whose subscapularis was repaired after RTSA compared with those whose subscapularis was not repaired (Table 5).
Postoperative Patient-Reported Outcomes in Patients With Glenosphere Size 38 mm Compared With 42 mm a
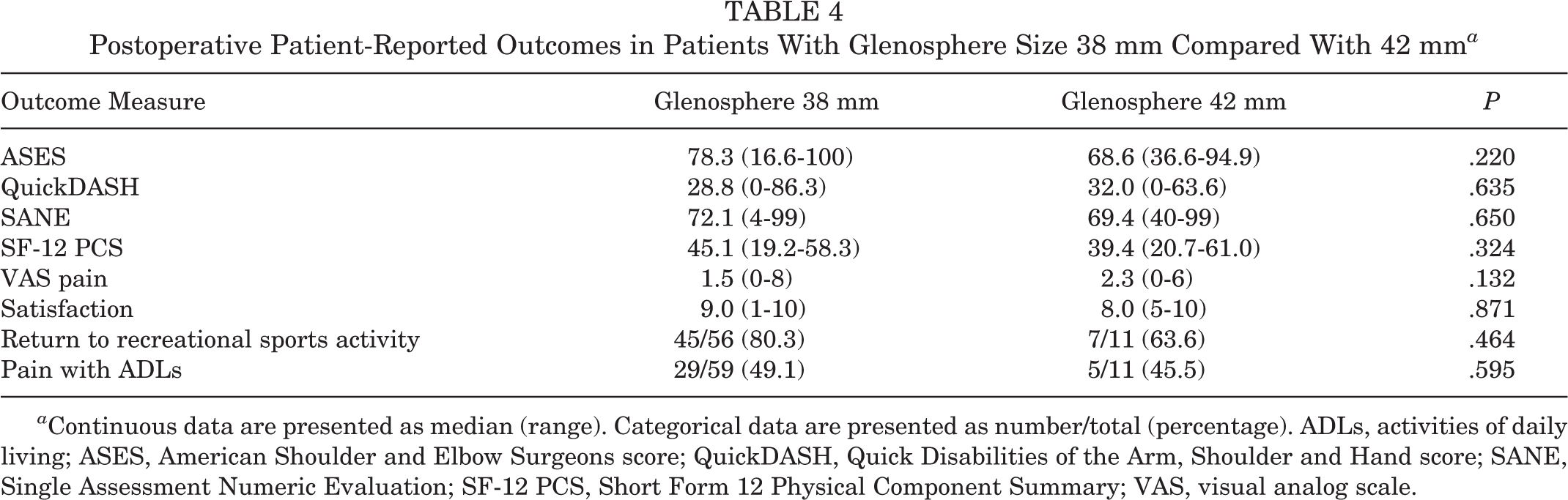
a Continuous data are presented as median (range). Categorical data are presented as number/total (percentage). ADLs, activities of daily living; ASES, American Shoulder and Elbow Surgeons score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand score; SANE, Single Assessment Numeric Evaluation; SF-12 PCS, Short Form 12 Physical Component Summary; VAS, visual analog scale.
Postoperative Patient-Reported Outcomes in Patients With Reparable Versus Irreparable Subscapularis a

a Continuous data are presented as median (range). Categorical data are presented as number/total (percentage). ADLs, activities of daily living; ASES, American Shoulder and Elbow Surgeons score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand score; SANE, Single Assessment Numeric Evaluation; SF-12 PCS, Short Form 12 Physical Component Summary; VAS, visual analog scale.
b Statistically significant difference between groups.
Active range of motion significantly improved in all measured planes from pre- to postoperatively (Table 6). In addition, both forward elevation and external rotation strength significantly increased after RTSA (Table 7).
Pre- and Postoperative Range of Motion a

a Values are expressed in degrees as mean ± SD.
b Statistically significant difference between groups.
Pre- and Postoperative Strength Testing a

a Strength testing was scored on a scale of 0-5, where 5 = normal. Values are expressed as median (25th-75th percentiles).
b Statistically significant difference between groups.
Discussion
The most important finding of this study is that patients with a reparable subscapularis demonstrated higher postoperative PROS after RTSA than patients with an irreparable subscapularis. Moreover, improvements in both ASES and QuickDASH scores were significantly correlated with increasing age. In addition, our results suggest that glenosphere size, independent of age, did not significantly affect outcomes.
It has previously been reported that younger age may be a risk factor for poorer outcomes after RTSA. 3 Ek et al 3 reported their results after RTSA in 35 patients younger than 65 years, noting an increase in the relative Constant score from 34% to 74% and a high complication rate of 37.5%. Additionally, they reported an improvement in subjective shoulder value from 23% to 66%. Although the heterogeneity of outcome metrics limits comparisons, the QuickDASH and ASES scores in the current study improved with increasing age.
Garcia et al 6 investigated rates of return to sport after RTSA in 76 patients who were active in a sport preoperatively. The average follow-up was 31.6 months and the average patient age was 74.8 years. The improvement in ASES scores was similar to that in our study (34.30 preoperative to 81.45 postoperative), and 85% of patients returned to 1 or more sporting activities at an average of 5.3 months after surgery. Age above 70 years was a significant predictor of decreased return to activities, which differs from the results of our study. The 85% rate of return to sport was higher than those previously published by Edwards et al 2 (75%) and Simovitch et al 21 (60%). The Edwards study included only 4 patients, whereas the Simovitch study included 67 patients who participated in a sport preoperatively. In the Simovitch study, of the patients who resumed sports postoperatively, 30% indicated that they were able to perform their activities at a higher level, and 65% reported no change in performance. The 3 most popular sports in their series were golf, swimming, and water aerobics.
More recently, Liu et al 14 compared return-to-sport rates after RTSA (102 patients) and hemiarthroplasty (71 patients). The investigators found that patients returned to sport at a significantly higher rate after RTSA as compared with hemiarthroplasty (85.9% vs 66.7%, respectively). In addition, the RTSA patients were more likely to be satisfied with their ability to play sports. Of note, no sports-related complications occurred. The authors identified female sex, age younger than 70 years, surgery on the dominant extremity, and a preoperative diagnosis of arthritis with rotator cuff dysfunction to predict a higher likelihood of return to sports. Bulhoff et al 1 analyzed return to activity levels after RTSA based on patients’ preoperative activity levels. At a mean follow-up of 4.8 years, 93% of patients who participated in sports preoperatively were able to return to sport postoperatively. 1 The most commonly reported low-demand sporting activities were stationary bike and treadmill use, and the most popular medium-demand sports were fishing, dancing, and swimming. 13 Despite no clear consensus in the literature regarding the acceptable activity level after RTSA, the available data demonstrate that most patients are able to return to low-impact sports.
According to a finite element model, increasing the glenosphere diameter improves the joint contact area and does not affect maximum contact stress. 12 The clinical relevance of increasing glenosphere diameter to maximize contact area is conflicting. Mollon et al 16 demonstrated that patients with 42-mm glenospheres had greater improvements in active forward elevation and external rotation compared with patients who had 38-mm glenospheres, whereas Müller et al 17 showed a clinically moderate but significant increase in external rotation strength at midterm follow-up by increasing the glenosphere diameter. In contrast, another study reported that larger glenospheres (42 mm) significantly reduced the development of scapular notching compared with smaller glenospheres (38 mm) without a significant influence in the Constant score. 22 This is in line with our results showing (with the numbers available) no significant differences in PROS or return to recreational sports activity rates based on glenosphere size. However, a 2017 biomechanical study showed that larger glenospheres underwent significantly greater polyethylene volume loss and volumetric wear rates, whereas smaller glenospheres underwent greater polyethylene surface deviations. The authors cautioned that the enhanced stability provided by larger glenospheres must be weighed against the potential for increased polyethylene wear. 8 Studies with longer follow-up will be needed to elucidate the influence of glenosphere size on functional outcomes.
Currently, there is controversy regarding whether the subscapularis should be repaired during RTSA, and the clinical question remains whether a reparable subscapularis tendon should be repaired when a Grammont-style prosthesis is used. 7,20,23 Giles et al 7 demonstrated in a cadaveric model that rotator cuff repair with glenosphere lateralization can produce an antagonistic effect that increases deltoid tension along with joint loading. Our findings indicate that patients with reparable subscapularis tendons demonstrated superior PROS, including rates of return to recreational sports activity, compared with those patients who had an irreparable subscapularis tendon. Our study findings are confirmed by Friedman et al, 5 who showed significantly higher postoperative scores for patients after subscapularis tendon repair without any significant difference in the complication or scapular notching rates between cohorts. Further studies will be vital to understand the indications for subscapularis repair during reverse shoulder arthroplasty.
Limitations
Although this study demonstrates interesting, clinically useful findings, it is not without limitations. This study is comprised of a single surgeon’s experience at a referral practice center with highly motivated and active patients. Therefore, the results may not be generalizable to other surgical practices or patient populations. The patients in this study were not randomized. However, to reduce the risk of reporting bias, the data were collected prospectively and analyzed retrospectively. We cannot rule out that the lack of statistically significant differences in the comparisons between factors and outcome scores may be because of type II β error. Within the scope of this study, we could not identify a statistically significant association between glenosphere size and PROS or rates of return to recreational sports activity. Still, we are reporting results from a large patient cohort in an increasingly used surgical procedure, and we believe that our results are valuable for other surgeons.
Conclusion
Patients who had a subscapularis tendon that could be repaired showed a significantly higher rate of return to recreational sports activity than patients whose subscapularis tendon was irreparable. Older age was correlated with greater improvement in several, although not all, patient-reported outcome measures. Glenosphere size was not significantly associated with higher PROS or rates of return to recreational sports activity.
Footnotes
One or more of the authors declared the following potential conflict of interest or source of funding: This research was supported by the Steadman Philippon Research Institute, which is a 501(c)(3) nonprofit institution supported financially by private donations and corporate support from the following entities: Arthrex, DJO, MLB, Ossur, Siemens, Smith & Nephew, and XTRE. J.A.G. has received grant support from DJO and educational support from Arthrex and Smith & Nephew. S.F. has received grant support from Arthrex and DJO and educational support from Arthrex and Smith & Nephew. S.M. has received grant support from Arthrex and DJO and educational support from Arthrex and Smith & Nephew. P.J.M. has received consulting fees from Arthrex and Merz Pharmaceuticals GmbH and speaking fees from Arthrex; receives royalties from Arthrex and MedBridge; and owns stock in VuMedi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Vail Valley Medical Center Institutional Review Board (protocol No. 2002-03).