
Abstract
Background:
Incidence rates of pediatric anterior cruciate ligament (ACL) injuries and ACL reconstruction (ACLR) are increasing. In adult patients with ACLR, limb-level loading profiles are less dynamic compared with uninjured controls (ie, lesser peaks and minimal offloading during midstance) early post-ACLR, and less dynamic profiles are associated with deleterious knee tissue changes. However, joint-level loading magnitudes during gait in the pediatric ACLR population are unknown.
Purpose/Hypothesis:
The purpose of this study was to compare medial and lateral tibiofemoral joint contact force profiles between pediatric patients with ACLR and pediatric matched controls. It was hypothesized that pediatric patients with ACLR would demonstrate less dynamic medial and lateral joint contact force profiles compared with matched uninjured pediatric controls.
Study Design:
Cross-sectional study; Level of evidence, 2.
Methods:
Pediatric patients 6 to 24 months post-ACLR (n = 25) and matched pediatric controls (n = 25; Tanner stage category, sex, Tegner activity score ±3) underwent a gait biomechanical assessment at a single time point, where ground-reaction forces and marker trajectories were collected. The concurrent optimization of muscle activation and kinematics algorithm was utilized to estimate medial and lateral compartment tibiofemoral joint contact forces in the ACLR limb and pediatric matched control limb. A functional linear model was utilized to determine differences in joint contact force profiles throughout stance phase (0%-100%).
Results:
Pediatric patients with ACLR demonstrated a high occurrence of concomitant injuries (80% meniscal pathology; 13% chondral injuries) and walked with greater medial tibiofemoral joint contact forces in midstance (42%-63% of the stance phase; 339-N maximal difference) and greater lateral joint contact forces in the late stance compared with pediatric controls (69%-80%; 288 N).
Conclusion:
Pediatric patients with ACLR may demonstrate a less dynamic tibiofemoral joint contact force loading profile in the medial compartment, as evidenced by greater loading during midstance, compared with matched pediatric controls.
The development of knee osteoarthritis (KOA) is a serious clinical concern in adults with an anterior cruciate ligament (ACL) injury. 44 It is estimated that half of adults will develop radiographic evidence of KOA within decades of ACL injury regardless of undergoing ACL reconstruction (ACLR) and rehabilitation. 26 Therefore, substantial effort has been made in determining the factors that increase the risk of KOA to inform the development of novel intervention strategies to mitigate KOA development after ACL injury and reconstruction. The development of aberrant gait biomechanics after ACLR is linked to deleterious joint tissue changes consistent with KOA development.4,28,37,38 This has led to recent advancement in gait retraining interventions aimed at modifying harmful joint tissue changes after ACLR.2,6,13 Recent data have indicated that pediatric ACL injury rates have increased more than those of any other age category12,49; however, most studies that have evaluated the link between gait biomechanics and KOA development are in adults. Overall, it remains unknown if joint loading is altered in pediatric patients with ACLR. Consequently, it is difficult to make evidence-based decisions on developmentally appropriate rehabilitation for gait retraining in this population.
Less dynamic limb-level loading profiles (Figure 1) during walking, characterized by lesser first and second peak vertical ground-reaction force (vGRF) and greater vGRF during midstance,3,8,10 have been linked to altered articular cartilage composition and metabolic activity after ACLR in adults, consistent with early osteoarthritis development.2,4,28,37,38 Previous work has also identified that adult patients with ACLR reporting clinically relevant knee symptoms demonstrate components of a less dynamic limb-level loading strategy (ie, lesser first and second peak vGRF and greater midstance vGRF) compared with asymptomatic counterparts. 39 Preliminary data suggest that pediatric patients exhibit different limb-level loading compared with adult patients with ACLR 24 ; however, that study did not assess maturation status or include a developmentally matched pediatric control group. It is also unclear if altered limb-level loading in pediatric patients with ACLR translates to altered knee joint–level loading (ie, joint contact forces). Much of the previous research linking gait biomechanics and KOA development has focused on understanding limb-level loading via vGRF and net joint moments in adults, and there is limited overall research measuring the magnitude of joint-level loading. Estimating loading at the tibiofemoral articulation may provide the most specific information about the nature of aberrant loading to knee tissue.
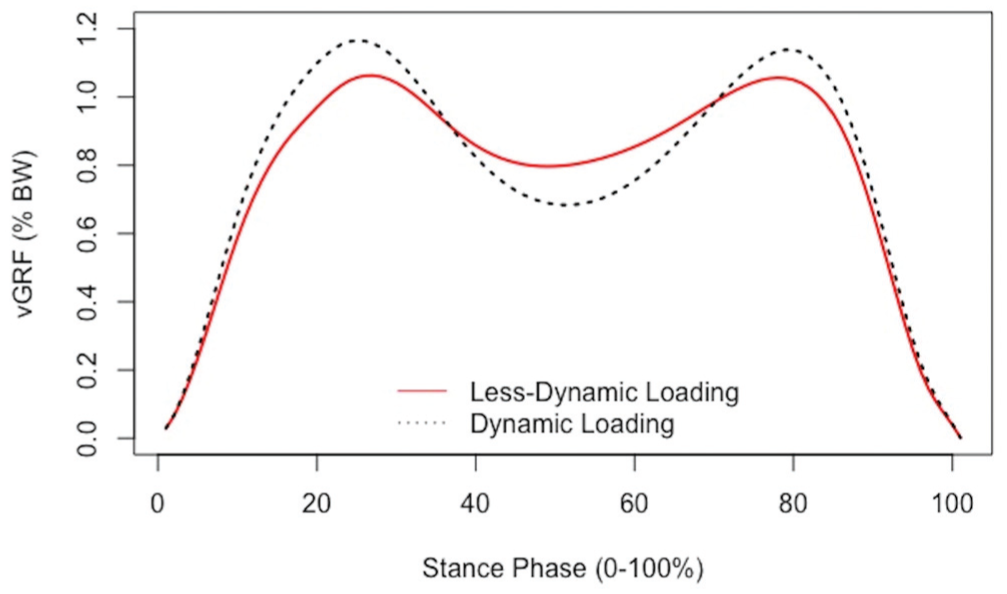
Less dynamic limb-level loading profiles are characterized by lesser vertical ground-reaction force (vGRF) magnitudes surrounding the first and second vGRF peaks and greater loading during midstance. BW, body weight.
Advances in computational modeling approaches have made it possible to estimate the contribution of soft tissue (ie, muscles, tendons, and ligaments) and simulate joint-level loading, specifically at the knee, to estimate loads experienced during dynamic activities. 5 Adults demonstrate lesser peak tibiofemoral joint force magnitudes in comparison with both the contralateral limb and uninjured controls within 3 years after ACLR. 40 In a separate cohort study, adult patients who walked with lesser peak tibiofemoral joint contact forces at 6 months after ACLR developed radiographic evidence of osteoarthritis at a 5-year follow-up. 48 However, the magnitudes of knee joint–level loading exhibited by pediatric patients with ACLR during walking are unknown, and it is unclear if pediatric patients with ACLR demonstrate different magnitudes of knee joint contact forces compared with uninjured pediatric controls.
The purpose of this study was to determine between-group differences in the medial and lateral tibiofemoral joint contact force profiles throughout the stance phase of walking. We hypothesized that, like in adult patients with ACLR, pediatric patients with ACLR would demonstrate less dynamic medial and lateral joint contact force profiles (ie, profiles with minimal offloading during midstance) compared with matched uninjured pediatric controls.
Methods
Study Design
We recruited pediatric patients (Tanner stages 1-4 and between 7 and 17 years of age) between 6 and 24 months after primary unilateral ACLR and respectively collected uninjured matched pediatric controls. Pediatric patients with ACLR were recruited from orthopaedic clinics, physical therapy clinics, and travel and school sport teams. Pediatric control participants were recruited from travel sport organizations and school sport teams. All pediatric participants provided written informed assent, with the parents or legal guardians of the participants providing parental permission, and were enrolled between December 2022 and March 2024. The institutional review board at the university approved all study procedures and recruitment strategies. All participants completed the Tanner stage questionnaire in a private room at the beginning of the testing session and placed the questionnaire in a sealed envelope to maintain discretion. Participants then completed a biomechanical gait analysis and questionnaires to collect concomitant injury information and sport participation level based on question 7 of the Hospital for Special Surgery Pediatric Functional Activity Brief Scale. A chi-square test was performed to determine between-group differences in sport participation level. Envelopes containing Tanner stage classification were opened after completion of the testing session. Only participants who did not report Tanner stage 5 on both the breast development/genitalia and pubic hair categories were included in the final analysis.
Participants
All pediatric participants self-reported a Tanner stage 1 to 4. Patients were excluded if a multiple-ligament reconstruction was required at the time of ACLR, a fracture occurred at the time of ACL injury, they were pregnant, they had a body mass index ≥35, or they were radiographically diagnosed with osteoarthritis. We included participants with multiple graft types and histories of concomitant meniscal and chondral injuries. Pediatric participants without a history of knee injury were recruited to serve as a comparison control group. Recruitment of uninjured controls was staggered from the ACLR group to specifically match each uninjured control to patients with ACLR by sex, Tegner activity level (±2), Tanner stage category (early pubertal or mid/late puberty), and limb (dominance). Control participants were excluded if they had a previous history of lower extremity surgery, were pregnant, had a body mass index ≥35, had received a radiographic diagnosis of osteoarthritis, or had a lower extremity orthopaedic injury within the last 6 months. A recent study conducted in our laboratory reported a strong effect (d = 0.83) for the maximum difference in knee flexion angle (4.16°; between 29% and 100% of the stance phase) between adolescent and adult patients between 6 and 12 months after ACLR. 24 Our analysis was a part of a larger study design that enrolled 25 participants per group and was powered (1 – β = .8) using a 2-sided .05 significance level (G*Power Version 3.1.9.2) to detect strong between-group differences (d > 0.83) for each traditional biomechanical outcome.
Tanner Stage Questionnaire
The Tanner stage questionnaire, originally developed with 5 stages of maturation, 47 was used to determine sexual maturity in all participants. Self-determined Tanner staging is a valid and reliable method for determining sexual maturity in children. 41 Pediatric participants were classified into the early pubertal (stage 1 or 2), mid/late pubertal (stage 3 or 4), or sexually mature (stage 5) category. Participants who self-reported a Tanner stage of 5 on both categories (ie, pubic hair or genitalia/breast development for males and females, respectively) were excluded from the analysis.
Biomechanics Collection
A total of 26 retroreflective markers were placed on participants, including the bilateral acromion, anterior superior iliac spine, greater trochanter, medial and lateral epicondyles, medial and lateral malleoli, first and fifth metatarsals, calcanei, and a single marker on the sternum. 29 Tracking markers were placed bilaterally on the thigh and tibia. 29 A 3-marker sacral plate was also utilized to estimate the bilateral posterior superior iliac spine and the coccyx. 29 Participants’ habitual walking speed was determined as previously described 36 using timing gates (Dashr Systems). Once participants were comfortable walking through the 6-m motion capture volume, a standing reference was recorded and overground gait biomechanics were collected from 5 walking trials within 95% to 105% of the participant’s habitual walking speed. Ground-reaction forces were collected from 3 staggered, embedded force plates (Bertec) and sampled at 1200 Hz. Marker trajectories were collected from a 10-camera motion capture system at 120 Hz (Vicon). The dominant or nondominant limb of the uninjured pediatric controls was selected for analysis based on whether the pediatric match with ACLR had torn their dominant or nondominant limb. We reported the varus angle of the knee during the standing reference capture. We first extracted the first peak vGRF of the 5 walking trials (occurring within the first 50% of the stance phase) in the ACLR limb and limb of uninjured controls. Because of the high computational demands, we then performed modeling and simulations using the step exhibiting the peak vGRF that demonstrated the smallest numeric difference in reference to each individual participant’s mean peak vGRF.
Concurrent Optimization of Muscle Activation and Kinematics
Marker trajectories from a standing trial were used as inputs to create a scaled generic musculoskeletal model in OpenSim. The model considered the tibiofemoral and patellofemoral (6 degrees of freedom [DOF]), hip (3 DOF), and ankle (1 DOF) joints, 23 as well as soft tissue elements, including 44 muscle-tendon units and 12 hip, knee, and ankle ligaments. 5 Marker trajectories and ground-reaction forces from the biomechanics collection, used as inputs to concurrent optimization of muscle activation and kinematics (COMAK), were low pass filtered at 6 and 10 Hz, respectively. A forward sweeping simulation was completed, as a function of tibiofemoral joint flexion, to estimate secondary DOF at the knee (ie, knee adduction/abduction and internal/external rotation). Next, inverse kinematics were performed using the knee hinge joint model to estimate the primary DOF of the lower extremity, allowing for 1 DOF at the ankle and knee and 3 DOF at the hip. The new marker coordinates and the ground-reaction forces were then inputted into the COMAK algorithm, which is a cost-optimization function that concurrently solves for lower extremity kinematics, soft tissue forces, and joint contact forces without limitations on the tibiofemoral and patellofemoral joint motions with reference to knee joint flexion. 45 We utilized the simulated medial and lateral tibiofemoral joint contact force estimates as primary outcome measures. In the primary analysis, medial and lateral joint contact forces were time-normalized to the stance phase of gait (0%-100%).
Surface Electromyography Acquisition and Processing
Electromyography (EMG) electrodes (Delsys; Trigno) were placed on participants according to SENIAM (Surface Electromyography for the Non-Invasive Assessment of Muscles) guidelines 16 and the most prominent portion of the muscle belly. Muscles included the medial and lateral vastus lateralis, medial and lateral gastrocnemius, semitendinosus, and biceps femoris. EMG data were collected at 2160 Hz during the same testing session of walking (Vicon) and postprocessed in Visual3D (C-Motion; 2020 × 64). EMG data were filtered using a 20- to 450-Hz linear envelope, rectified, and low pass filtered at 10 Hz (fourth-order Butterworth). Data for each individual muscle of the ACLR limb and matched control limb were time-normalized to the stance phase of gait, recognized as the time interval between heel strike (vGRF, >20 N) and toe-off (vGRF, <20 N).
Statistical Analysis
Demographic variables were assessed for normality using a Shapiro-Wilk test, and between-group differences were determined using independent-samples t tests. A Mann-Whitney U test was utilized for variables that were not normally distributed to determine between-group differences. A functional linear model with group waveform effects, modeled with Bayesian penalized spines, was constructed to compare medial and lateral joint contact force profiles throughout the stance phase of gait between the groups.18,34 In utilizing a smoothness penalty on the penalized spines, 22 we limit the potential for overfitting group waveform estimates. Open-script code (bayesFDA) available on GitHub was utilized and all analyses were run in R (Version 4.1.2; R Foundation for Statistical Computing). 17 Group means were estimated from the regression coefficients, and 95% confidence intervals were calculated around the group means. Any portion of the stance phase for which the 95% confidence interval of the mean difference waveforms did not cross zero was recognized as a statistically significant difference. The following statistical metrics were reported: regions of the stance phase with statistically significant differences and the maximum between-group difference within statistically significant regions. Walking speed is understood to influence knee kinetics in traditional biomechanical analyses 9 ; therefore, a sensitivity analysis was completed by replicating the primary analysis with the addition of walking speed as a covariate in the functional linear model. As pediatric males and females mature at different rates,25,41 we also performed a post hoc analysis using the same functional linear model to determine between-group (ie, ACLR and control) and between-sex differences in the medial and lateral tibiofemoral joint contact force profiles. We conducted an analysis of variance on body mass (kg) with main effects of group and sex, as well as the group by sex interaction, to ensure differences were not driven by group characteristics. We also conducted a separate sensitivity analysis utilizing the same functional linear model for the primary and secondary difference analyses after controlling for body mass.
Exploratory Post Hoc Analysis: Qualitative Model Validation
A qualitative assessment was performed post hoc for COMAK model validation. Muscle excitation values estimated from COMAK were extracted for the medial and lateral vastus lateralis, medial and lateral gastrocnemius, semitendinosus, and biceps femoris; low pass filtered at 40 Hz; and time-normalized to the stance phase (0%-100%). The maximum excitation value was identified for each muscle, and EMG data were normalized to the identified maximum excitation value occurring during the stance phase. Mean normalized excitation estimates and measured EMG values were visualized and qualitatively interpreted across the stance phase for a subset of pediatric patients with ACLR (n = 5) and pediatric controls (n = 5). The qualitative assessment will provide a precursory assessment of muscle activation agreement between measured EMG-based excitation and COMAK-estimated muscle excitations for future studies using COMAK.
Results
A total of 50 participants were included: 25 pediatric patients with ACLR and 25 uninjured pediatric controls. The majority of pediatric patients with ACLR were recruited from clinical sites (ie, orthopaedic clinic or physical therapy; n = 12), while others were recruited from travel teams (n = 7), school sport teams (n = 3), and general word of mouth (n = 3). Pediatric control participants were recruited from travel sport organizations (n = 9), school sport teams (n = 8), and general word of mouth (n = 8). The cohort consisted of 60% female participants (Figure 2). There were no statistically significant differences in age (P = .26) or gait speed (P = .13) (Table 1) between groups. Pediatric patients with ACLR did demonstrate greater knee valgus during quiet standing compared with pediatric controls (P < .01). Additionally, there were no statistically significant differences in sport competition level between the pediatric ACLR and control groups [χ2 (3, N = 50) = 5.47] (P = .14).
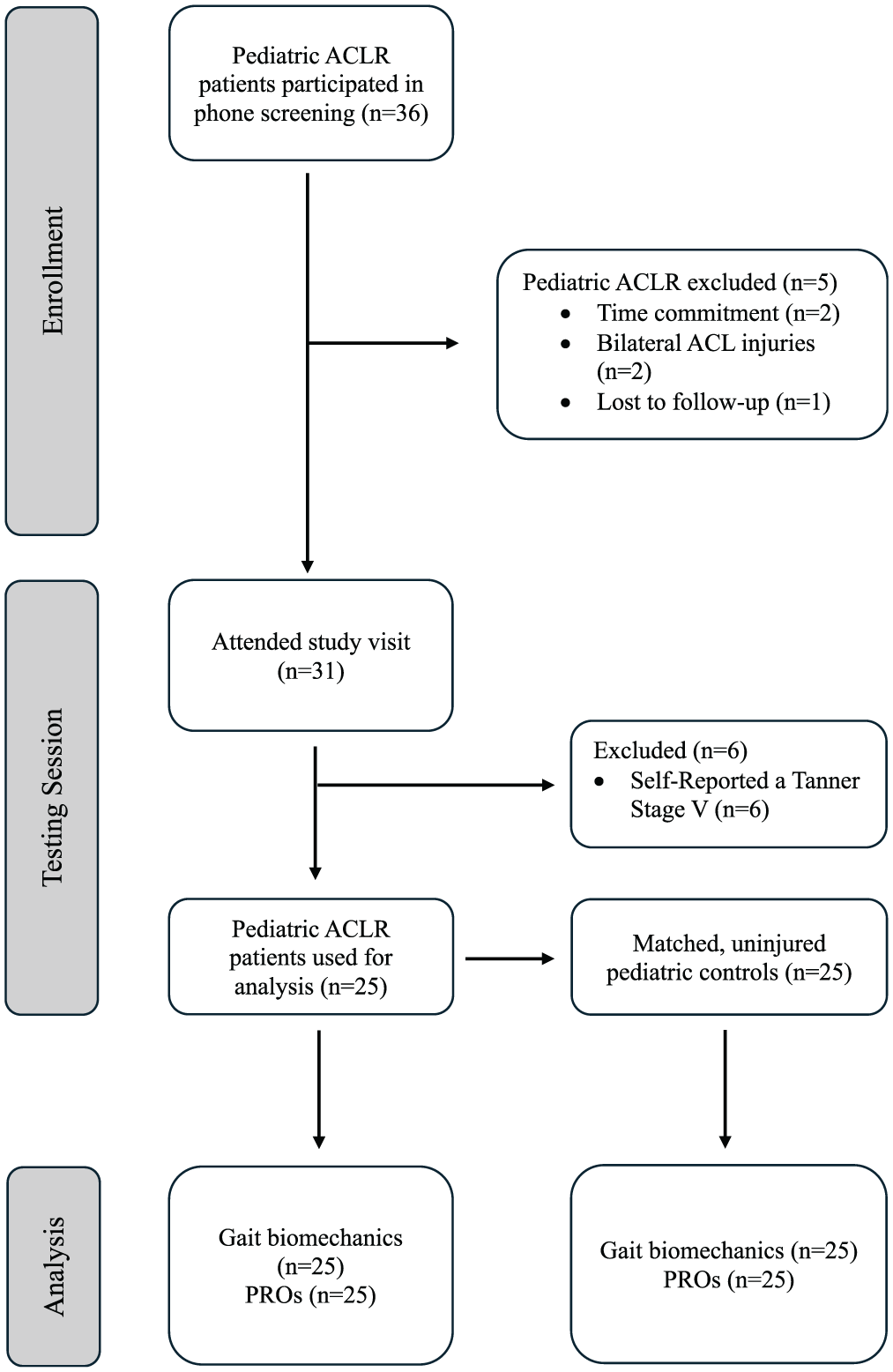
CONSORT (Consolidating Standards of Reporting Trials) flowchart depicting enrollment, data collection, and analyses of the pediatric anterior cruciate ligament (ACL)–reconstructed cohort and matched uninjured pediatric control cohort. ACLR, anterior cruciate ligament reconstruction; PRO, patient-reported outcome.
Participant Characteristics by Group a
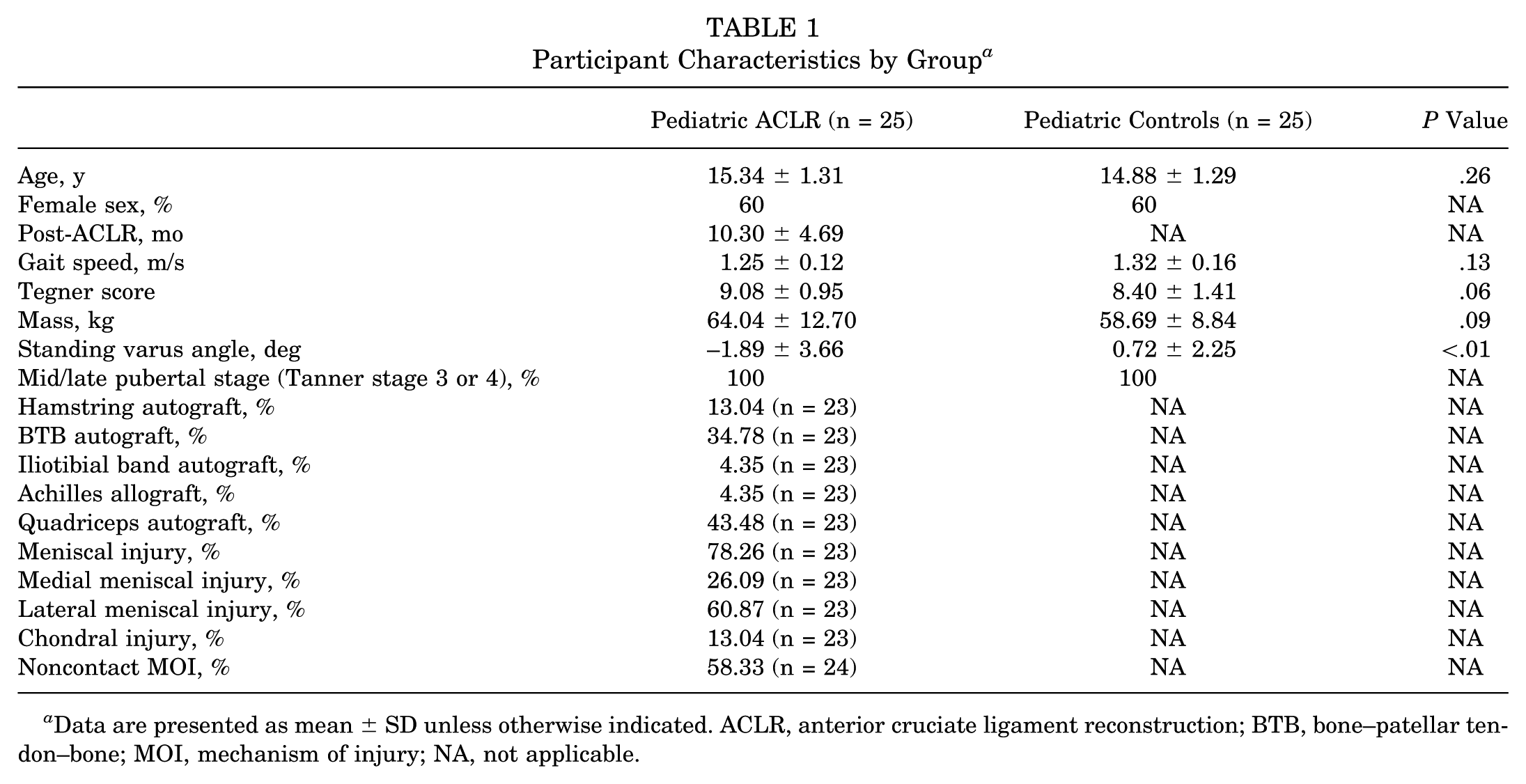
Data are presented as mean ± SD unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; MOI, mechanism of injury; NA, not applicable.
Primary Analysis: Medial and Lateral Tibiofemoral Joint Contact Force Profiles
Pediatric patients with ACLR demonstrated greater medial joint contact forces in midstance (42%-63% of the stance phase; 340-N maximum between-group difference) (Figure 3; Table 2) and greater lateral joint contact forces in the late stance (69%-80%; 288 N) (Figure 3) compared with pediatric controls. After controlling for walking speed in our sensitivity analysis, pediatric patients with ACLR still demonstrated greater medial joint contact forces in midstance (44%-57% of the stance phase; 302 N) (Table 2) and greater lateral joint contact forces in the late stance (65%-82%; 340 N) (Table 2).
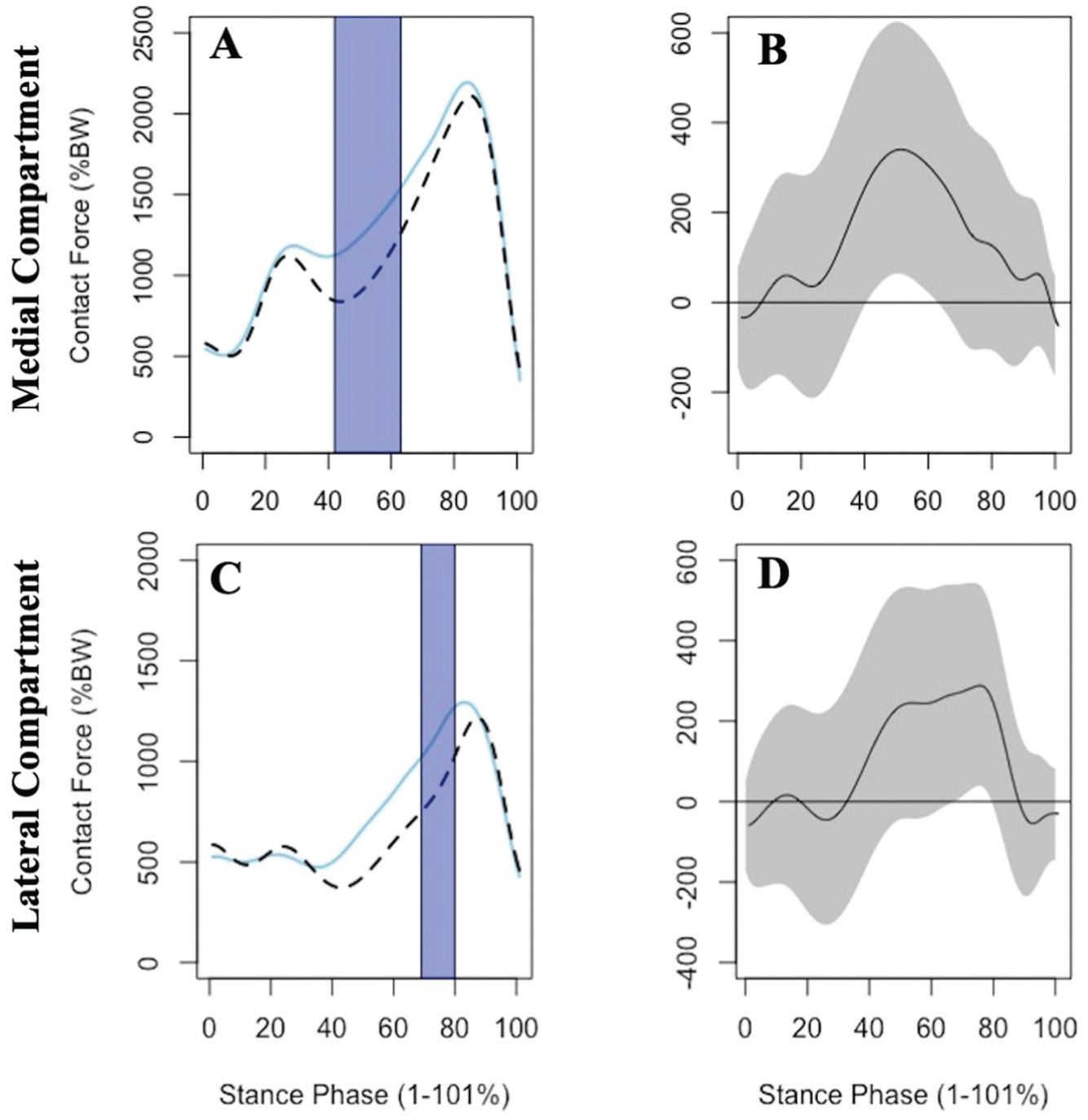
Group means and corresponding mean difference curves for the pediatric anterior cruciate ligament reconstruction (ACLR) cohort (solid) and uninjured pediatric cohort (dashed) are portrayed for the medial (A and B) and lateral (C and D) tibiofemoral joint contact forces of the ACLR limb throughout the entirety of the stance phase. Gray bands represent the associated 95% confidence intervals around the mean difference curves. BW, body weight.
Between-Group Differences in Absolute Magnitudes of Knee Joint CFs a
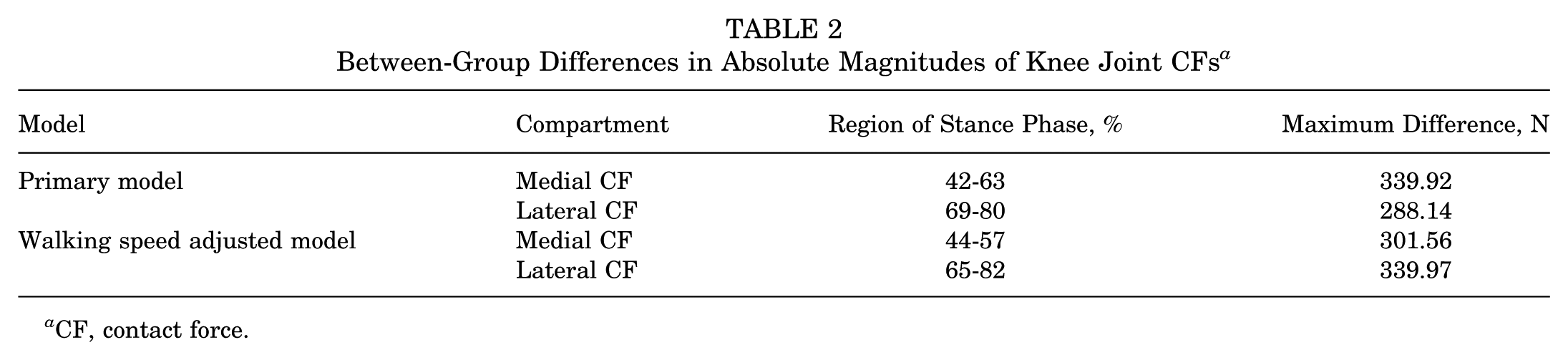
CF, contact force.
Post Hoc Analysis: Medial and Lateral Tibiofemoral Joint Contact Force Profiles by Sex
There was no difference in body mass between ACLR and control groups [F(1, 46) = 2.86; P = .097], sex [F(1, 46) = 0.01; P = .93], or group × sex [F(1, 46) = 0.21; P = .65]. Female pediatric patients with ACLR exhibited greater medial joint contact forces during the late stance compared with male pediatric patients with ACLR (84%-94%; –379 N) (Figure 4, A and B) and compared with female pediatric controls (45%-64%; –408 N) (Figure 4, E and F). No between-group differences were identified between the pediatric male and female controls or between the male patients with ACLR and male pediatric controls (Figure 4, C and D; Figure 2, G and H). Male pediatric patients with ACLR demonstrated greater lateral joint contact forces in the late stance than female pediatric patients with ACLR (63%-83%; 724 N) (Figure 5, A and B). Male uninjured controls exhibited greater lateral joint contact forces in the late stance than female uninjured controls (78%-97%; 501 N) (Figure 5, C and D). No differences between female ACLR and control groups were identified (Figure 5, E and F). Lastly, male patients with ACLR walked with greater lateral contact force magnitudes in the mid- to late stance compared with male pediatric controls (63%-79%; 588 N) (Figure 5, G and H).
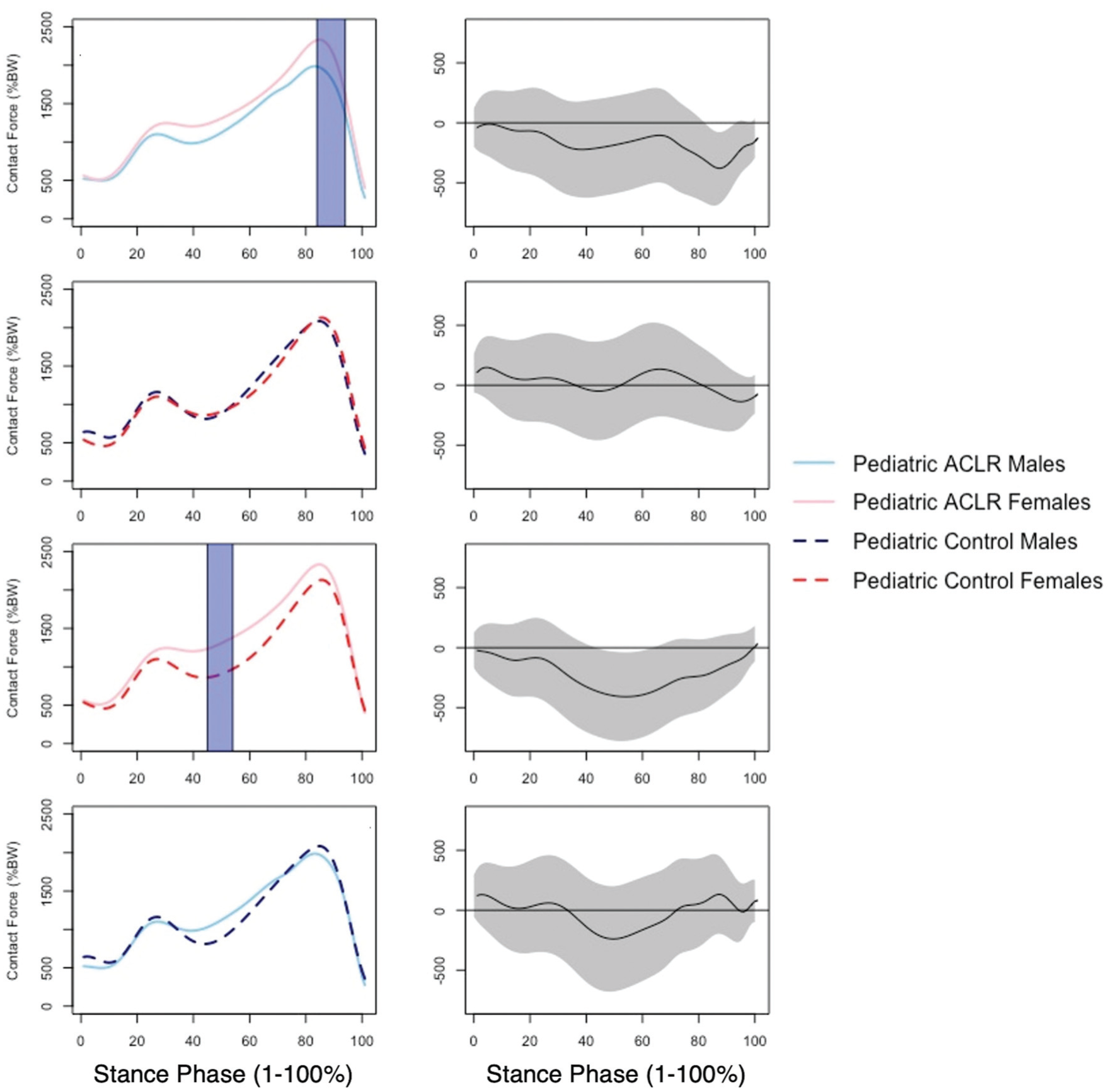
Group means and associated mean difference curves for pediatric anterior cruciate ligament reconstruction (ACLR) male (light blue), pediatric ACLR female (pink), pediatric male control (dashed navy), and pediatric female control (dashed red) cohorts are illustrated for the medial tibiofemoral joint contact forces for the ACLR limb throughout the entirety of the stance phase. Gray bands represent the associated 95% confidence intervals around the mean difference curves. Areas where the 95% confidence intervals did not cross zero were recognized as statistically significant differences and are denoted with shaded blue bars.
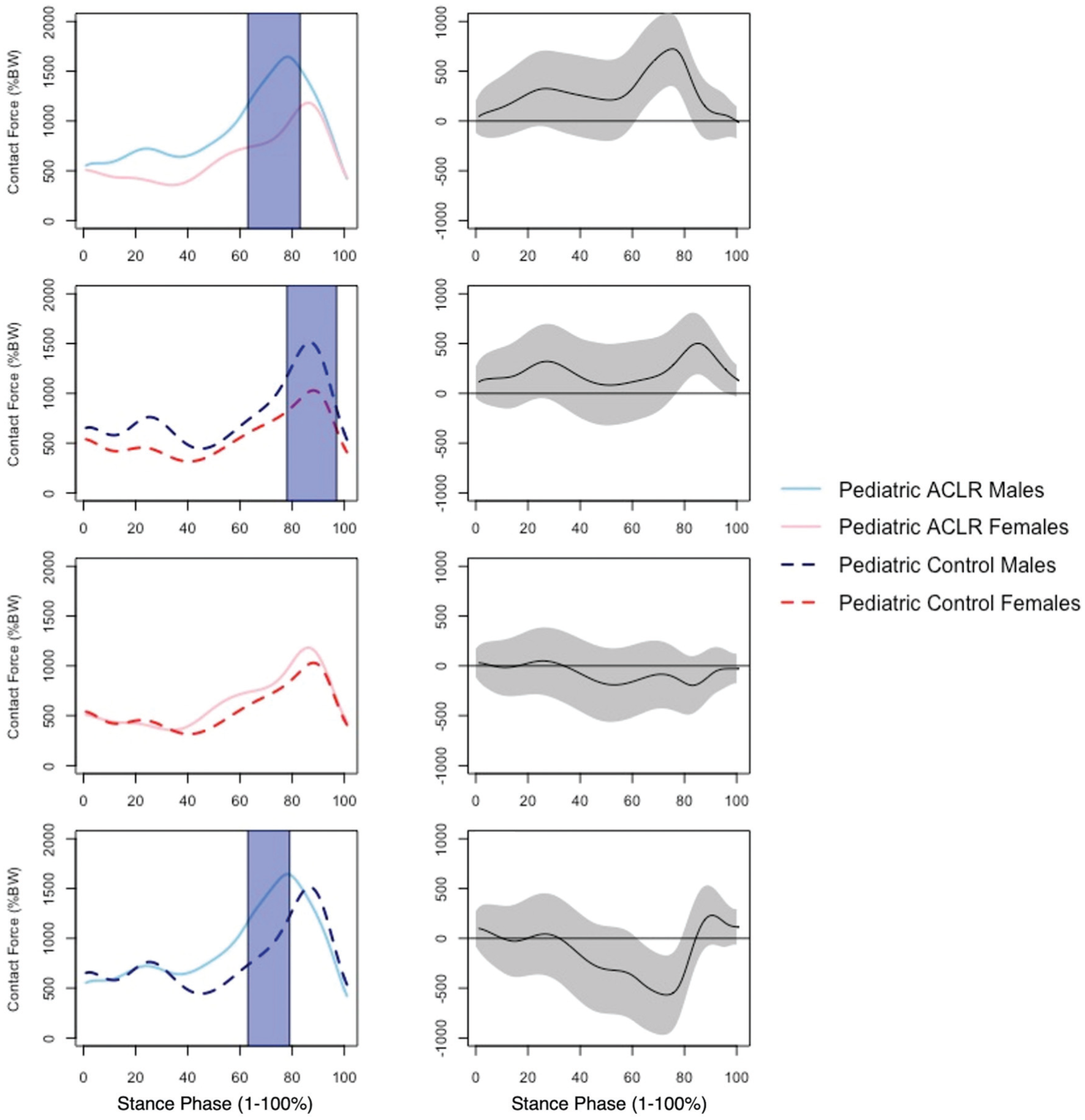
Group means and associated mean difference curves for pediatric anterior cruciate ligament reconstruction (ACLR) male (light blue), pediatric ACLR female (pink), pediatric male control (dashed navy), and pediatric female control (dashed red) cohorts are illustrated for the lateral tibiofemoral joint contact forces for the ACLR limb throughout the entirety of the stance phase. Gray bands represent the associated 95% confidence intervals around the mean difference curves. Areas where the 95% confidence intervals did not cross zero were recognized as statistically significant differences and are denoted with shaded blue bars.
Post Hoc Analysis: Controlling for Body Mass
No statistically significant differences between the pediatric ACLR group and control group were identified in the medial compartment after controlling for body mass. After controlling for body mass, pediatric patients with ACLR still demonstrated greater lateral compartment joint loading in the late stance (72%-77%; 267 N) (Appendix Table A1, available in the online version of this article).
Female patients with ACLR still exhibited greater medial tibiofemoral joint contact forces than the male patients with ACLR in the late stance after controlling for body mass (98%-100% vs 85%-94%; 179 N vs 326 N). As identified in the primary model, there were no between-group differences in medial compartment loading identified between the pediatric male and female controls or between the male patients with ACLR and male pediatric controls (Appendix Table A2, available online). After controlling for body mass, no statistically significant differences in medial compartment loading magnitudes were found between female patients with ACLR and female controls (Appendix Table A1, available online).
Male pediatric patients with ACLR still exhibited greater lateral joint contact forces in the late stance compared with female pediatric patients with ACLR (62%-84%; 730 N). After controlling for body mass, male uninjured controls exhibited greater lateral joint contact forces in the late stance compared with female uninjured controls (78%-100%; 485 N). As identified in the primary model, no differences between female ACLR and control groups were found. Finally, male patients with ACLR walked with greater lateral contact force magnitudes in the mid- to late stance compared with male pediatric controls (64%-79%; 557 N) (Appendix Table A2, available online).
Exploratory Post Hoc Qualitative Model Validation
All model-predicted excitation levels in the pediatric ACLR group were higher than those in the pediatric controls for all muscles but generally followed the same shape (Appendix Figure 1, available online). Similar EMG patterns were observed between the pediatric ACLR and control groups, with some notable differences in the semitendinosus profiles in the early stance. All model-predicted excitation levels in the pediatric ACLR group were higher than the EMG values and appeared to align better with EMG values for pediatric controls. Clear profile discrepancies between model-predicted excitations and EMG values for both groups were observed for the medial gastrocnemius.
Discussion
Our results support our hypothesis, as the pediatric ACLR group demonstrated greater loading magnitudes during midstance (42%-63%), which may be indicative of less dynamic medial tibiofemoral joint contact force profiles during walking. While these differences in medial tibiofemoral joint contact force remained similar after controlling for gait speed, there were no statistically significant differences in tibiofemoral joint contact forces between the pediatric ACLR and control groups after controlling for body mass. Pediatric patients with ACLR demonstrated greater lateral compartment loading surrounding the maximal peak (69%-76%) compared with pediatric controls, a finding that did not change substantially after adjusting for walking speed or body mass. To the best of our knowledge, the present study is the first to estimate tibiofemoral joint contact force profiles in pediatric ACLR individuals and compare them with those of matched pediatric uninjured controls. Our finding of greater joint-level loading during midstance in the medial compartment is consistent with less dynamic loading of the tibiofemoral joint—an outcome that may be important for understanding the link between gait biomechanics and deleterious changes in tibiofemoral articular cartilage early after ACLR in pediatrics. While recent work by Moran et al 32 estimated a low incidence of osteoarthritis clinical diagnoses in children (<16 years of age) within 5 years of ACLR, at 1.6%, no research has determined osteoarthritis incidence using structural outcomes at long-term clinical time points to compare with adult rates.
Previous work assessing limb-level loading profiles identified that vGRF magnitudes during midstance were most strongly linked to MRI estimates of worse tibiofemoral cartilage composition (ie, proteoglycan density) in adult patients at 12 months after ACLR. 4 Furthermore, vGRF profiles marked by lesser first and second peaks and greater midstance values (ie, less dynamic) are associated with worse patient-reported symptoms in adults. 39 Less dynamic limb-level loading profiles in adult patients with ACLR have similarly been conceptually linked to older adults with early radiographic KOA. 3 Therefore, identifying less dynamic knee joint–level loading in the medial compartment in our cohort is concerning for the cartilage health of a pediatric ACLR population. The pediatric ACLR group exhibited up to approximately 340 N larger medial contact forces during midstance compared with uninjured controls. Less dynamic loading profiles may contribute to harmful changes in articular cartilage by altering fluid flow and metabolic activity within the articular cartilage.1,19,31 As the medial compartment typically undergoes the earliest tibiofemoral articular cartilage changes associated with osteoarthritis development,11,35 there is a timely need for future studies to determine the observational link between less dynamic joint-level loading profiles and knee health in the pediatric ACLR population. We also found that pediatric patients with ACLR walked with greater lateral tibiofemoral joint loading in the late stance, which may reflect changes in frontal plane kinematics during the push-off portion of the stance phase. Additionally, we noted that the pediatric ACLR group demonstrated slight knee valgus during quiet standing. It is possible that an anatomic predisposition toward dynamic knee valgus may explain greater lateral compartment loading magnitudes in the pediatric ACLR group compared with controls. Previous work has identified that a second peak vGRF <1.11% body weight in late stance is 6.36 times more predictive of reporting worse patient-reported outcomes at 6 months after ACLR. 7 The association between joint loading in the late stance and biological outcomes is understudied but may be important for understanding cartilage health and osteoarthritis development.
We also identified sex differences in medial and lateral compartmental loading profiles in our post hoc analyses. Female pediatric patients with ACLR exhibited less dynamic knee joint loading profiles in the medial compartment (ie, greater midstance loading) compared with female controls; however, no statistically significant differences were found after controlling for body mass. Overall, similar less dynamic contact force profiles were found after controlling for body mass in the pediatric patients with ACLR; however, the effect between the ACLR and control cohorts may have been smaller in the sensitivity analysis due to lower statistical power. Female pediatric patients with ACLR also had greater second peak loading compared with male pediatric patients with ACLR, a finding that remained unchanged after controlling for body mass. Therefore, it is possible that pediatric girls may require targeted or lengthened intervention as compared with pediatric boys with ACLR. Conversely, male pediatric patients with ACLR exhibited greater lateral compartmental loading at the second peak compared with female pediatric patients with ACLR and male pediatric controls. Male pediatric controls demonstrated greater loading at the second peak compared with female pediatric controls in the lateral tibiofemoral compartment. Similar between-group differences in the lateral compartment remained after controlling for body mass, suggesting that a sex-specific loading profile may exist. In a cross-sectional analysis of healthy children (7-18 years of age), males possessed thicker articular cartilage compared with females, and the medial femoral cartilage was thicker than the lateral femoral cartilage across sexes. 43 In vivo loading profiles are associated with cartilage thickness 20 ; therefore, it is possible that either biological differences or biological adaptations to loading profiles may influence the sex differences in knee joint contact force profiles observed in the present study. Future studies should seek to determine the optimal magnitudes and profiles of tibiofemoral joint contact force loading in children and the unique link between contact force magnitudes and tibiofemoral articular cartilage composition.
Less dynamic knee joint loading early after ACLR may require precision gait interventions that may go above and beyond traditional rehabilitation. Previous work has utilized real-time gait biofeedback to cue an increase in first peak vGRF to acutely increase the dynamic nature of the vGRF waveform and sagittal plane motion.13,27 Acutely cuing changes in limb-level loading magnitudes during a standardized walking protocol has also been associated with reduced biomarker concentration in serum cartilage oligomeric matrix protein,2,6 a biomarker of cartilage breakdown. 15 Preliminary work has suggested that acutely cuing limb-level magnitude increases may concurrently increase the dynamic nature of joint-level loading profiles during walking in adult patients with ACLR 33 ; therefore, it may be a promising intervention strategy to reduce early osteoarthritis development. Additional work in this area is needed to determine if children could respond similarly to interventions currently developed for adult patients with ACLR.
While our findings are novel, there are some limitations that should inform future research. The computational model utilized for the current analysis was originally developed on a 26-year-old woman, 23 and there are inherent physiological differences between children and adults25,30 that reduce the availability of a robust pediatric-specific model. 46 However, the use of a developmentally matched comparison group increases confidence that biomechanical differences exist after ACLR in children. Future studies should seek to determine if there are differences in joint contact force magnitudes between pediatric and adult participants with ACLR with appropriate pediatric model corrections. Bilateral differences in gait biomechanical profiles exist in adults after ACLR 10 ; therefore, future work should also seek to assess between-limb differences in knee joint contact force magnitudes in pediatric patients with ACLR. Previous work assessing peak joint-level loading magnitudes in adult patients with ACLR has reported both raw and mass normalized units.14,40,42 Our choice to report raw values in our primary analysis reflects the cartilage-centric outcome of interest, and we additionally included a post hoc analysis to control for the effect of body mass. Nearly 80% of our pediatric ACLR cohort had meniscal pathology and 13% had chondral injuries, which logically decreases the surface area on which to distribute applied loads during walking and, consequently, may have increased the load experienced at the knee. Future research should assess pediatric ACLR joint contact loads in conjunction with MRI estimates of cartilage morphology. The small sample of pediatric patients with ACLR included in the analysis (n = 25) were between 6 and 24 months after ACLR, and we did not perform assessments at a specific postoperative time point. Furthermore, we cannot determine whether recruitment location influences injury cause; however, all pediatric ACLR participants in our sample reported participating in an athletic activity at the time of ACL injury. Pediatric patients with ACLR also varied in the type of ACLR procedure and graft type received, 21 and we did not exclude patients based on the surgical procedure or collect skeletal maturity status. Future work should determine if graft type affects joint-level loading magnitudes in pediatric patients during walking after ACLR. Additionally, while we acknowledge that anatomic knee varus angle is important in understanding knee joint loading profiles in pediatric patients with ACLR, our study reported the frontal knee angle measured using motion capture; future studies should utilize radiographic methods to determine the effect of anatomic knee alignment on magnitudes of medial and lateral knee joint contact forces. Lastly, our qualitative analysis identified good temporal alignment between COMAK-estimated muscle activation and measured EMG values for most muscles. However, the model appeared to overestimate muscle excitations for the medial gastrocnemius in both pediatric groups, and it is unknown how the overall contact force estimates were impacted. Future work is necessary to characterize muscle coordination patterns in pediatric patients with ACLR and, secondarily, determine if pediatric-specific model estimations may improve overall model performance in the pediatric ACLR population.
Conclusion
Pediatric patients with ACLR between 6 and 24 months after ACLR demonstrate greater medial, tibiofemoral joint contact forces during midstance of gait compared with pediatric matched uninjured controls. Female pediatric patients with ACLR may exhibit a more pronounced, less dynamic loading profile in the medial compartment compared with male pediatric patients with ACLR. Conversely, male pediatric patients with ACLR demonstrated greater loading in the lateral compartment during late stance when compared with female pediatric patients with ACLR. Less dynamic joint-level loading profiles during walking in pediatric patients with ACLR may highlight concern for articular cartilage health in a young, active patient population.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465251372465 – Supplemental material for Tibiofemoral Joint Contact Force Profiles of Pediatric Patients After Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-pdf-1-ajs-10.1177_03635465251372465 for Tibiofemoral Joint Contact Force Profiles of Pediatric Patients After Anterior Cruciate Ligament Reconstruction by Elizabeth Bjornsen, J. Troy Blackburn, Jason R. Franz, W. Zachary Horton, Darin A. Padua, Sandra J. Shultz, Samantha Tayne and Brian G. Pietrosimone in The American Journal of Sports Medicine
Footnotes
Submitted February 1, 2025; accepted July 30, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.B. received funding from the American College of Sports Medicine (22-01803) to complete this research. B.P. and J.R.F. are co-founders of VETTA Solutions, a company that makes wearable sensor solutions for gait retraining. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.