
Abstract
Background:
When treated conservatively, unstable distal clavicle fractures demonstrate a high symptomatic nonunion rate. While a variety of surgical techniques have been described, many of these techniques are associated with high failure rates and hardware-related complications. The surgical technique used in this study has shown promising biomechanical results; however, long-term clinical results have not yet been described.
Purpose:
To assess the clinical and radiological outcomes of a surgical technique for fixing displaced distal clavicle fractures using a combination of cortical button fixation and coracoclavicular (CC) ligament reconstruction.
Study Design:
Case series; Level of evidence, 4.
Methods:
We conducted a retrospective review of 22 consecutive patients with displaced, unstable Neer type II or V distal clavicle fractures who underwent this surgical technique from 2012 to 2019. Primary outcome variables were radiographic union, patient satisfaction, and postoperative shoulder function. Preoperative and postoperative University of California, Los Angeles (UCLA), and American Shoulder and Elbow Surgeons (ASES) scores were compared. Secondary outcome variables included intraoperative complications, postoperative complications, time to radiographic union, and preoperative and postoperative CC distance. Quality of life was assessed using preoperative and postoperative 36-Item Short Form Health Survey (SF-36) scores.
Results:
Nearly all (21/22) patients were available for a final review; 1 patient was lost to follow-up at 2 weeks. All 21 patients achieved radiographic union by 4 months (mean, 60.38 days; range, 41-84 days; 95% CI, 53.80-66.96 days). All patients were satisfied with the surgical procedure and their functional outcome. The mean UCLA score improved from 5.36 (95% CI, 4.14-6.60) preoperatively to 32.52 (95% CI, 30.56-34.48) postoperatively (mean difference, 27.14; P < .001). The mean ASES score improved from 16.23 (95% CI, 9.79-22.67) preoperatively to 88.11 (95% CI, 81.82-94.40) postoperatively (mean difference, 71.91; P < .001). Statistically significant improvements in SF-36 scores were seen in the physical functioning, role limitations due to physical health, pain, social functioning, and emotional well-being categories. There were 3 postoperative complications, including 1 patient with a minor complication secondary to hardware irritation, 1 patient with adhesive capsulitis, and 1 patient with wound dehiscence requiring wound closure.
Conclusion:
We describe a surgical technique for fixing displaced distal clavicle fractures using a combination of cortical button fixation and CC ligament reconstruction that resulted in a 100% union rate and excellent clinical outcomes with acceptable complications.
Distal third clavicle fractures represent only 25% of all clavicle fractures, 25,28,31 but they account for a high proportion of complications related to clavicle fracture treatment. Neer 24 originally classified these fractures based on the position of the fracture line relative to the coracoclavicular (CC) ligament. Unstable distal clavicle fractures, classified as Neer types II and V, present a unique challenge for surgical fixation because of the small size and comminution of the lateral fragment, disruption of the CC ligament, and large deforming forces on the fracture fragments. An injury to the CC ligament leads to vertical instability of the medial fragment and a high rate of pseudarthrosis. While these fractures are rare, Neer 23,24 found that distal fractures may account for up to 50% of clavicle nonunion.
While many techniques have been described to treat unstable distal clavicle fractures, ‡ most techniques utilize rigid fixation with plate osteosynthesis. Despite excellent union rates, these techniques are associated with a high complication rate, with complications ranging from acromial osteolysis and peri-implant fractures to pin migration. 7,8,12,13,19,29,36 In addition, many of these techniques require a second surgical procedure for hardware removal.
In response to these limitations, newer techniques have been described 6,17 that are modeled conceptually after techniques used to surgically treat acromioclavicular joint dislocations. These newer techniques, which can be performed either open or arthroscopically, utilize CC fixation with cortical button devices to achieve anatomic reduction of the fracture. These techniques have demonstrated excellent clinical and radiographic outcomes with low overall complication rates. 6,17
The purpose of this study was to assess the clinical and radiographic outcomes of a surgical technique for fixing displaced, unstable distal clavicle fractures using a combination of cortical button fixation and CC ligament reconstruction, as previously described by Yagnik et al. 38 Our hypothesis was that this technique would result in union rates comparable with plate osteosynthesis with fewer complications.
Methods
Between 2012 and 2019, there were 22 consecutive patients with displaced, unstable type II or V distal clavicle fractures treated with a combination of CC stabilization with cortical button fixation and CC ligament reconstruction as described by Yagnik et al. 38 All procedures were performed by 1 of 2 surgeons (G.P.Y., C.J.J.) utilizing the same surgical technique and postoperative rehabilitation protocol. Patients with other distal clavicle fracture types (I or III) were excluded from analysis. One patient was lost to follow-up at 2 weeks. This was an international patient who was presumed to have returned to his home country and could not be contacted despite multiple attempts. The mean age at the time of injury was 55.5 years (range, 24-87 years), and the mean time to surgery was 11.82 days (range, 3-42 days).
Clinical and Radiological Outcomes
Patients were followed in the office until they achieved radiographic union and returned to their baseline activity level. Radiographic union was assessed by 2 independent physicians and was defined by the presence of a callus on clavicle radiographs (anteroposterior, Zanca). Patients who had less than 12 months’ in-office follow-up were contacted by telephone after 12 months had passed from the date of surgery to repeat an assessment of functional status. Primary outcome variables were radiographic union, patient satisfaction, and postoperative shoulder function. Shoulder function was assessed using preoperative and postoperative University of California, Los Angeles (UCLA), scores and American Shoulder and Elbow Surgeons (ASES) scores and compared using a paired 2-sample t test of the mean at a confidence level of 95%. Secondary outcome variables included intraoperative complications, postoperative complications, time to radiographic union, and preoperative and postoperative CC distance. Quality of life was assessed using preoperative and postoperative 36-Item Short Form Health Survey (SF-36) scores. Scaled scores were compared using a paired 2-sample t test of the mean at a confidence level of 95%.
Surgical Technique
All patients underwent surgical fixation using cortical button fixation and CC ligament reconstruction as described by Yagnik et al 38 (Figure 1). After the administration of a regional interscalene block and the induction of general anesthesia, the patients were placed in a modified beach-chair position. A 5-cm vertical incision was made 2 to 3 cm medial to the acromioclavicular joint with the base of the incision at the proximal aspect of the coracoid. The deltotrapezial fascia was carefully incised in line with the clavicle to facilitate later closure over the implants. The medial and lateral soft tissues adjacent to the coracoid were bluntly dissected to facilitate later passage of the sutures and graft around the coracoid.

Illustration of distal clavicle repair using a combination of cortical button fixation and coracoclavicular ligament reconstruction. Image courtesy of Arthrex.
Graft Preparation
A 7 × 240–mm semitendinosus allograft was used in all procedures. The ends of the graft were tapered and whip-stitched using a No. 2 nonabsorbable suture. The graft was tapered so that both ends passed easily through a 6-mm tunnel.
Graft Passage and Fixation
A coracoid passer was then placed around the coracoid, and a strong passing suture was shuttled through the instrument and passed under the coracoid. Two different colored suture tapes (FiberTape; Arthrex) and the prepared allograft were then shuttled around the coracoid. A 2.4-mm drill was used to create a bicortical drill hole for the suture tapes as close to the fracture site as possible while still preserving 5 mm of bone laterally to prevent iatrogenic fractures through this drill hole. A second tunnel for the graft was created with a 6.0-mm cannulated reamer over a 2.4-mm guide wire at least 15 mm medial to the first tunnel to ensure an adequate bone bridge. The FiberTape sutures were shuttled through the lateral tunnel before passing the graft so that the sutures lay posterior to the graft. Both ends of the graft were then passed through the 6-mm tunnel using a second shuttle suture (Figure 2A). The 4 limbs of FiberTape sutures were passed through a cortical button (Dog Bone; Arthrex) and tied down, reducing the medial fragment to the lateral fragment. The graft was then tensioned and fixed using a 5.5 × 10–mm PEEK interference screw (Arthrex) (Figure 2B). After fixing the graft, the free ends of the graft were amputated. A free needle was then used to pass the free ends of the FiberTape sutures through the anterior deltotrapezial fascia in a horizontal mattress fashion. These sutures were then tied, repairing the deltotrapezial fascia to the clavicle and burying the knot stacks to minimize the risk of soft tissue irritation. The incision was closed in a standard fashion.
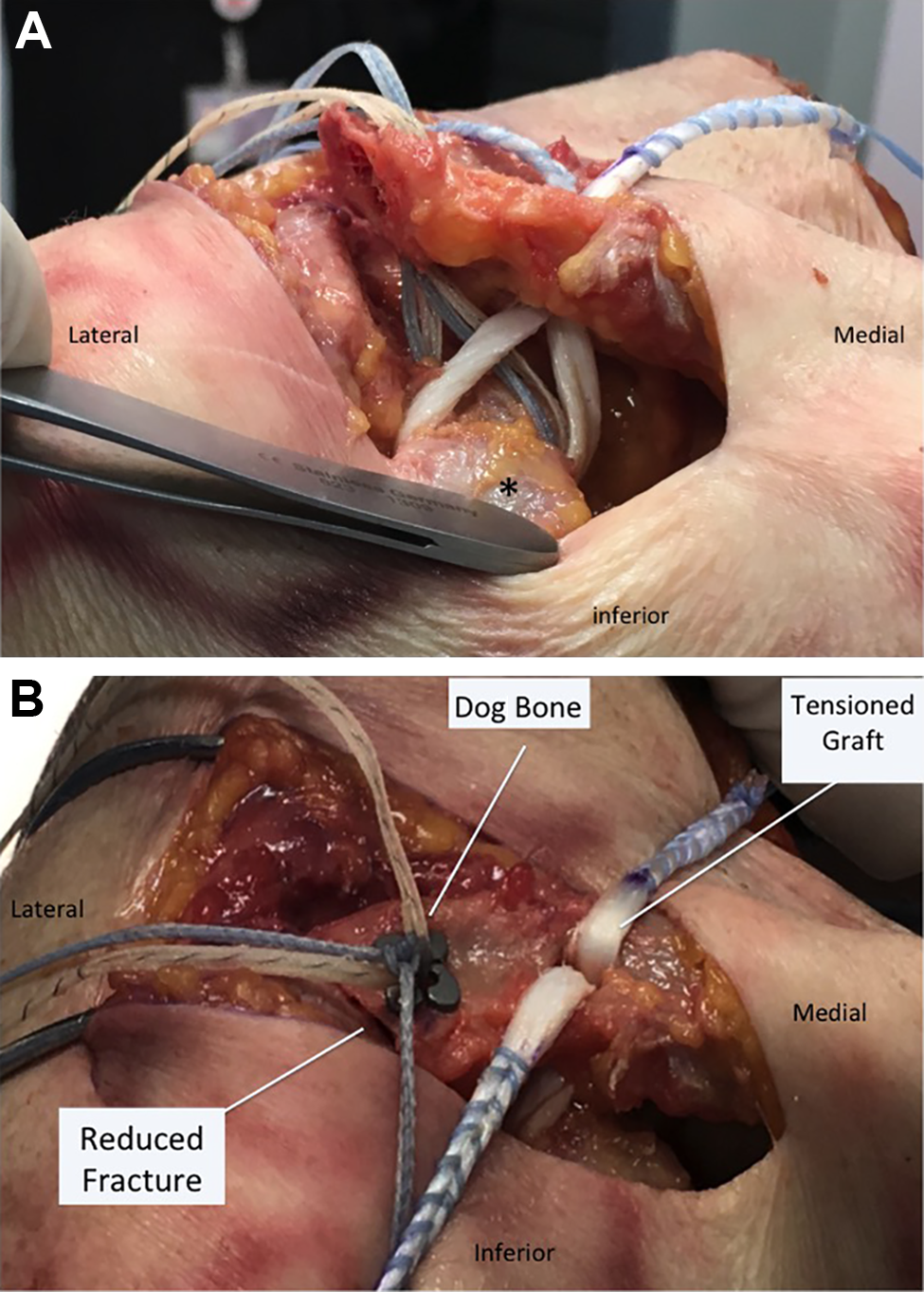
(A) Distal clavicle fracture in a right shoulder with suture tapes passed through a laterally based tunnel and the allograft passed through a medial tunnel. Asterisk (*) indicates the coracoid process. (B) Final construct demonstrates reduction of the distal clavicle fracture with suture tapes tied over a cortical button and the graft tensioned with an interference screw. The graft is passed anterior to the suture tapes.
Postoperative Rehabilitation
Postoperatively, the patients were placed into a sling to minimize tension on the repair site for 4 to 6 weeks. Supine passive range of motion of the shoulder was initiated immediately postoperatively. At 4 to 6 weeks, the patients began active and active-assisted range of motion exercises. Strengthening was initiated at 8 weeks. Full return to activity and sport began around 4 months.
Results
A total of 21 of 22 patients were available for final review. One patient was lost to follow-up at 2 weeks. The mean in-office follow-up was 4.55 months (range, 1.42-16.9 months), and the mean overall follow-up period was 30.19 months (range, 9-78 months; 95% CI, 21.25-39.13 months). Eighteen patients had type IIB fractures, and 4 patients had type V fractures. The mechanism of injury included bicycle accidents (n = 8), mechanical falls (n = 7), motor vehicle collisions (n = 5), and unknown (n = 2). Demographic factors are summarized in Table 1.
Patient Demographics

All patients (100%) achieved radiographic union (Figure 3). The mean time to union was 60.38 days (range, 41-84 days; 95% CI, 53.80-66.96 days). The mean preoperative CC distance was 27.45 ± 4.18 mm. The mean postoperative CC distance was 9.05 ± 3.34 mm.

Preoperative and postoperative radiographs. All patients achieved radiographic union.
The UCLA score improved from a mean of 5.36 (95% CI, 4.14-6.60) preoperatively to 32.52 (95% CI, 30.56-34.48) postoperatively at the time of final follow-up (mean difference, 27.14; P < .001). The ASES score improved from a mean of 16.23 (95% CI, 9.79-22.67) preoperatively to 88.11 (95% CI, 81.82-94.40) postoperatively at the time of last follow-up (mean difference, 71.91; P < .001). There was no significant difference in mean UCLA or ASES scores at the time of the final in-office visit and at telephone follow-up (mean UCLA score at final in-office visit: 30.81, mean ASES score at final in-office visit, 87.15; P > .05).
Quality of life was assessed using the SF-36. Scaled scores for each category in the SF-36 improved postoperatively. Statistically significant improvements were seen in the physical functioning, role limitations due to physical health, pain, emotional well-being, and social functioning categories. The increases in scores in energy/fatigue, role limitations due to emotional problems, and general health categories were not statistically significant.
There were no intraoperative complications. Three patients experienced postoperative complications. One patient had a minor complication secondary to hardware irritation, and the hardware was removed after fracture healing. A second patient with severe Ehlers-Danlos syndrome experienced wound dehiscence approximately 2 weeks after the initial surgical procedure. This patient underwent formal irrigation and debridement and primary wound closure in the operating room. All hardware was retained, and the patient went on to uneventful healing and an excellent clinical outcome. A third patient experienced transient adhesive capsulitis that resolved with physical therapy.
Discussion
The principal finding of this study is that displaced, unstable distal clavicle fractures treated with a combination of cortical button fixation and CC ligament reconstruction resulted in excellent clinical and radiographic outcomes. At the time of final follow-up, 100% of patients achieved radiographic union, which is comparable to fractures treated with plate osteosynthesis. Clinically, nearly all patients returned to their preinjury functional status. Finally, low-profile hardware resulted in an acceptable overall complication rate, with only 1 patient undergoing a second surgical procedure for hardware removal.
The surgical treatment of unstable distal clavicle fractures remains challenging. Traditional techniques include locking or hook plates, Kirschner wires, CC screws, suture anchors, or suture tension band wiring. 2,4,6,9,10,12,15,20,21 Despite satisfactory union rates, various complications have been associated with these techniques including loss of reduction, hardware migration, acromioclavicular joint arthritis, coracoid fractures, and hardware irritation. 3,7,11,13,16,35,36 Many of these techniques also require a second surgical procedure for hardware removal. A systematic review by Oh et al 26 demonstrated a 41% complication rate with hook plate fixation, which has been long considered the gold standard in the treatment of unstable distal clavicle fractures.
In response to these complications, newer techniques have been described that incorporate lower profile hardware and CC stabilization with a cortical button in an attempt to treat these fractures with less overall morbidity. 6,18,30 These techniques achieve fracture union by reducing the medial fracture fragment to the lateral fragment using low-profile hardware that is fixed to the coracoid. There are several advantages to these techniques when compared with plating. The primary advantage is that they can be used in most distal clavicle fracture patterns, including fractures with small or comminuted lateral fragments. Lower profile hardware also requires less soft tissue stripping of the superior clavicle, thereby resulting in less postoperative hardware irritation and subsequent surgery for implant removal.
Both arthroscopic 17,18,22 and open 6,30,34 techniques have been described, and both have reported excellent clinical results. Motta et al 22 presented 14 unstable distal clavicle fractures that were treated arthroscopically with a TightRope (Arthrex) alone. The authors reported a 100% union rate and excellent functional outcomes at final follow-up. In a larger arthroscopic series, Kraus et al 17 reported an 85% union rate and high patient satisfaction with the treatment of displaced distal clavicle fractures using a single TightRope technique. The authors did report 2 cases of asymptomatic nonunion and 1 fixation failure requiring revision with plate osteosynthesis. Most recently, Blake et al 5 performed arthroscopic cortical button fixation on 17 patients with Neer type II distal clavicle fractures using a TightRope device. Despite excellent functional outcomes, the authors did report a 17.5% nonunion rate and a hardware-related complication requiring implant removal.
Other authors have advocated for an open approach when treating unstable distal clavicle fractures using cortical button fixation. An open approach is less technically demanding, often resulting in shorter operative times. We feel that an open approach is superior, as it allows for direct anatomic reduction of the fracture site and removal of interposed soft tissue, which may be the cause of nonunion seen in studies utilizing arthroscopic techniques. Robinson et al 30 reported a 94% union rate and very low complication rate with open reduction and Endobutton fixation of 16 displaced distal clavicle fractures. Cho et al 6 treated 18 type IIB distal clavicle fractures with open CC stabilization using an Endobutton. They reported satisfactory clinical and radiographic outcomes with a nearly 95% union rate. Despite the excellent union rate, complications in this study included 1 intraoperative coracoid fracture and 4 cases of subsidence of the clavicular button into the upper cortex of the clavicle.
Our results are in concordance with these studies and further support the use of CC stabilization as a stand-alone procedure for treating unstable distal clavicle fractures. There are 2 unique features with our technique compared with other similar techniques. First, no bone tunnels are drilled through the coracoid. Instead, all sutures are passed around the coracoid, minimizing the risk of coracoid fractures. Studies describing techniques that drill through the coracoid have reported at least 1 coracoid fracture–related complication, 6,22 while no such fractures were encountered in the current study. Our technique does, however, include 2 bone tunnels in the clavicle. While we did not see any postoperative clavicle fractures, there is a theoretical risk thereof. When treating young athletes in contact sports, multiple drill holes may be a source of postoperative clavicle fractures, and thus, one must be aware of the risk in this population.
Second, not only is the distal clavicle fracture reduced and stabilized with CC fixation using a cortical button, but also the normal soft tissue attachments between the coracoid and clavicle are reconstructed using an allograft. Many of the other similar techniques utilize a single point of fixation with a TightRope-type device and fail to fully address the disrupted soft tissue attachments between the coracoid and clavicle. This creates high strain on the implant that can lead to CC button migration and subsidence and, in some cases, loss of reduction. 6,17,22 In our series, there was no incidence of implant subsidence, which may in part be related to the load-sharing qualities of ligament reconstruction.
In addition to load sharing, we believe that the graft strengthens the overall construct by providing a second point of fixation to further stabilize the construct. This theory was supported by a recent biomechanical study by Yagnik et al 37 that evaluated the current cortical button with a CC reconstruction technique using an allograft and compared it with several other techniques including a cortical button alone and a locking plate for the treatment of distal clavicle fractures. This biomechanical study found the cortical button and CC allograft reconstruction group to be the strongest group with the highest load to failure. The mean displacement after cyclic loading was also 47% less in the cortical button and CC allograft reconstruction group when compared with a locking plate, demonstrating the stiffness of the construct.
There are, however, some disadvantages to the surgical technique used in this study. The addition of allograft reconstruction does add complexity and surgical time to the procedure. The graft is also passed through a 6-mm bone tunnel in the clavicle, theoretically creating a stress riser. We feel that the stress fracture risk is minimized by near-complete filling of this tunnel with a 5.5-mm PEEK interference screw. It should also be noted that passing sutures and a graft around the coracoid comes with its own set of potential complications, including the risk of neurovascular injuries secondary to dissection around the coracoid, increased cost, and increased operative time. While this procedure may not be suitable for all distal clavicle fracture patterns, including highly comminuted or long oblique fractures, it does provide a solution to managing most Neer type II and V fracture patterns.
There are several limitations to this study. The number of patients in this study is small, and there is no control group. However, these fractures are rare, and the size of our patient cohort is comparable with that in other similar studies. While our data were prospectively collected on consecutive patients, our study design was a retrospective chart review and therefore has the same limitations of other similarly designed studies. Further well-designed prospective randomized clinical studies are needed to determine the optimal management of unstable distal clavicle fractures.
Conclusion
The management of unstable distal clavicle fractures with cortical button fixation and CC ligament reconstruction yields excellent clinical and radiographic outcomes. This technique can be used for most fracture patterns and provides a biomechanically strong construct with minimal risk of obligatory hardware removal.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: G.P.Y. has received educational support, consulting fees, and nonconsulting fees from Arthrex. C.J.J. has received consulting fees from Advanced Orthopaedic Solutions. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Baptist Health South Florida Institutional Review Board.