
Abstract
Background
Distal clavicle fractures and acromioclavicular joint dislocations frequently require surgical stabilization, and hook plate fixation is widely used but can be complicated by peri-implant fractures. This study aimed to evaluate patient, anatomical, and implant-related factors associated with peri-implant fractures after hook plate fixation for these injuries.
Methods
A retrospective cohort study was conducted at a single tertiary center including adults who underwent open reduction and internal fixation with a pre-contoured clavicle hook plate for distal clavicle fractures or acromioclavicular joint dislocations between October 2013 and November 2023. Demographic data, implant characteristics, and radiographic parameters (clavicle diameter, clavicle length, plate diameter, plate length, and their ratios) were collected. Patients with and without peri-implant fracture were compared using univariable statistical tests, and exploratory univariable logistic regression was performed to estimate associations between selected variables and peri-implant fracture.
Results
Among 282 patients, 9 (3%) developed peri-implant fractures after hook plate fixation. Patients with peri-implant fractures were older, shorter, and had lower body weight than those without fractures. The peri-implant fracture group also showed a smaller clavicle-to-plate diameter ratio, a higher plate-to-clavicle length ratio, and more frequent use of plates with a greater number of holes, indicating relatively thinner clavicles and disproportionately longer plates.
Conclusions
Peri-implant fractures after hook plate fixation for distal clavicle fractures and acromioclavicular joint dislocations were uncommon in this cohort but were associated with older age, smaller skeletal build, longer plates, and poor dimensional matching between the clavicle and plate. Careful assessment of clavicle morphology and judicious selection of plate length may help reduce stress concentration at the medial plate end and lower the risk of peri-implant fracture.
Introduction
Fractures of the distal clavicle and acromioclavicular (AC) joint dislocations are common injuries in orthopedic practice, often necessitating surgical intervention to restore shoulder function and ensure optimal recovery.
1
Among the various surgical options, open reduction and internal fixation (ORIF) using a hook plate has become a widely accepted technique due to its ability to provide stable fixation and facilitate bone healing.
2
However, despite its clinical effectiveness, hook plate fixation can be complicated by implant-related problems, and peri-implant fractures represent an uncommon but clinically relevant complication, with reported incidences generally ranging from 1.3 to 10% in series of distal clavicle fractures treated with hook plates.3–8 Late functional outcomes and overall complication rates after hook plate implantation have also been shown to depend on implant retention time, underscoring the need to better understand hook plate–related complications, including peri-implant fracture
9
(Figure 1). A case of a 19-year-old male with Neer classification type IIA distal clavicle fracture treated with the DePuy Synthes clavicle hook plate; (a), Anteroposterior radiograph at the time of injury. (b), Immediate postoperative radiograph after open reduction and internal fixation. (c), Postoperative day-17 radiograph demonstrates a peri-implant fracture originating from the medial end of the locking plate.
Peri-implant fractures occurring after hook plate fixation represent a significant clinical challenge. While the hook plate is designed to stabilize the distal clavicle or AC joint, its biomechanical configuration can unintentionally create stress risers, particularly at the medial end of the plate.3,8,10 These stress concentrations may predispose the surrounding bone to fracture, especially in anatomically or structurally vulnerable regions of the clavicle. 11
Advanced age and the lack of intraoperative hook plate bending have been identified as independent risk factors for peri-implant midshaft clavicle fractures after hook plate fixation. 7 This highlights the importance of surgical technique and patient-specific factors in minimizing fracture risk.
This study aimed to evaluate the demographic, anatomical, and implant-related risk factors associated with peri-implant fractures in patients treated with hook plates for distal clavicle fractures and AC joint dislocations. Identification of these contributing variables may facilitate the development of more tailored surgical strategies and contribute to reducing complication rates in clinical practice.
Materials and methods
This retrospective cohort study was conducted at a single tertiary medical center to comprehensively evaluate post-operative outcomes following open reduction and internal fixation (ORIF) with a hook plate for distal clavicle fractures and acromioclavicular (AC) joint dislocations. The study included patients who underwent ORIF with a hook plate between October 2013 and November 2023.
All study procedures involving human participants were reviewed and approved by the Institutional Review Board of our institution (IRB number 20250505R). Written informed consent was waived by the IRB as the research met the criteria for minimal risk studies, according to relevant guidelines and regulations. All procedures were conducted in accordance with the Declaration of Helsinki and institutional policies.
Patients underwent open reduction and internal fixation using a pre-contoured 3.5-mm LCP Clavicle Hook Plate (DePuy Synthes, Warsaw, Indiana) under general anesthesia. Plate length (5-, 6-, or 7-hole) was selected according to fracture pattern and clavicular length, with the aim of achieving sufficient medial screw fixation while avoiding unnecessary extension into the midshaft region.
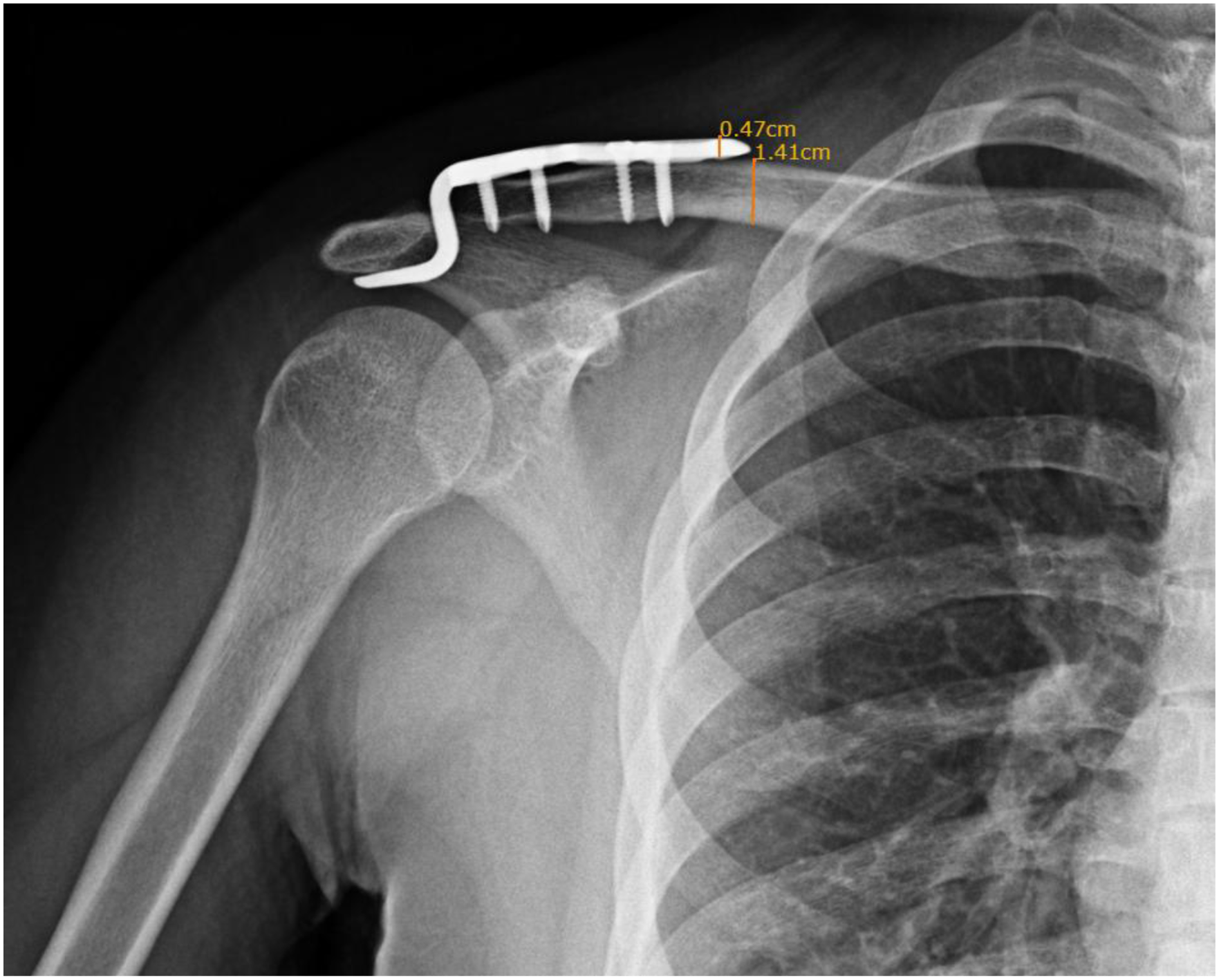
Postoperative standardized anteroposterior clavicle radiographs were obtained immediately after surgery and at routine outpatient follow-up visits and were used for radiographic measurements. Measurements were performed on a Picture Archiving and Communication System (EBM Technologies Inc., Taipei, Taiwan) by one orthopedic surgeon and independently checked by a second senior orthopedic surgeon; however, formal assessment of inter- and intra-observer measurement reliability was not undertaken in this study. Clavicle length was defined as the linear distance between the central points of the medial and lateral ends of the clavicle, and hook plate length as the distance from the medial end of the plate to the base of the hook, excluding the curved hook portion (Figure 2). Clavicle diameter was measured at the level of the medial end of the plate as the vertical distance between the superior and inferior cortices, and plate diameter as the plate thickness at the medial end on anteroposterior radiographs (Figure 3). For each patient, the clavicle-to-plate diameter ratio and plate-to-clavicle length ratio were calculated to describe dimensional matching between the implant and clavicle. Clavicle length was defined as the linear distance between the central points of the proximal and distal ends of the clavicle. Hook plate length was defined as the distance from the medial end of the plate to the base of the hook, excluding the curved hook portion. Clavicle diameter was measured at the level of the medial end of the hook plate, defined as the vertical distance between the superior and inferior cortices of the clavicle at that site. Hook plate diameter was defined as the plate thickness at its medial end, measured as the vertical height of the plate on anteroposterior radiographs.
Peri-implant fracture was defined as a new clavicular fracture occurring adjacent to the medial end of the hook plate on follow-up radiographs after the index operation, in an unfractured segment of bone. 3 Fractures were categorized as stress-related when they occurred without a reported recent traumatic event; for the purposes of this study, only stress-related peri-implant fractures without preceding new trauma were included in the analysis.
Patient-specific variables, including age, sex, body height, weight, and body mass index (BMI), were systematically extracted from medical records. Descriptive statistics were used to summarize demographic and clinical characteristics. Categorical variables were compared between patients with and without peri-implant fracture using the chi-square test, and continuous variables using the Student’s t-test as appropriate. Given the anticipated low event rate of peri-implant fractures, statistical analyses focused on univariable comparisons between patients with and without peri-implant fracture. Univariable logistic regression was additionally performed as an exploratory analysis to estimate odds ratios (ORs) with 95% confidence intervals (CIs) for the association between selected patient- and implant-related variables and peri-implant fracture, and all regression results were prespecified to be hypothesis-generating rather than confirmatory, with no complex multivariable models constructed to avoid overfitting in the setting of sparse outcome data. All statistical analyses were conducted using IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY, USA), and a p-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics
Characteristics, including implant features of the 2 groups.

Chi-square tests evaluated the categorical variables, and t tests evaluated the continuous variables *indicates statistical significance (p < 0.05).
The proportion of females was higher in the peri-implant fracture group than in the non-fracture group (56% vs 27%), although this difference did not reach statistical significance (p = 0.066). Diagnosis type was significantly associated with peri-implant fracture occurrence (p = 0.038), with distal clavicle fractures present in 89% of cases with peri-implant fractures and 54% of those without.
Patients who experienced peri-implant fractures were significantly older (60.56 ± 15.53 years vs 44.80 ± 14.93 years, p = 0.002), shorter in height (159.50 ± 8.94 cm vs 167.93 ± 8.34 cm, p = 0.005), and had lower body weight (57.54 ± 10.27 kg vs 69.86 ± 14.83 kg, p = 0.014) than those without fracture (Table 1). Mean BMI was lower in the peri-implant fracture group (22.23 ± 2.25 kg/m2 vs 24.65 ± 4.06 kg/m2), but this difference was not statistically significant (p = 0.096).
Radiographic parameters and implant dimensions
Radiographic analysis demonstrated significant anatomical differences between groups. The clavicle-to-plate diameter ratio was significantly lower in the peri-implant fracture group (2.30 ± 0.42) compared with the non-fracture group (2.84 ± 0.41, p < 0.001). The plate-to-clavicle length ratio was significantly higher in the peri-implant fracture group (0.50 ± 0.08 vs 0.43 ± 0.06, p = 0.002), suggesting that disproportionate plate size relative to clavicular dimensions may increase fracture risk.
Regarding implant characteristics, hook depth (15 mm vs 18 mm) did not differ significantly between groups (p = 0.365) in this cohort. In contrast, the number of plate holes was significantly associated with peri-implant fracture occurrence (p = 0.002). Only 11% of the peri-implant fracture group received a 5-hole plate for fixation, compared with 65% in the non-fracture group, whereas 6-hole and 7-hole plates were more common in the peri-implant fracture group (67% and 22%, respectively).
Logistic regression analysis
In univariable logistic regression, several patient- and implant-related variables showed significant associations with peri-implant fracture. Older age, shorter stature, and lower body weight were each associated with higher odds of peri-implant fracture, whereas sex and body mass index were not statistically significant. A smaller clavicle-to-plate diameter ratio and a greater number of plate holes—reflecting relatively thinner clavicles and longer plates—were also significantly associated with peri-implant fracture, suggesting that dimensional mismatch and increased plate length may contribute to stress concentration at the medial plate end.15–17
Univariable logistic regression for predicting peri-implant fracture.

CI: confidence interval, *indicates statistical significance (p < 0.05).
Univariable logistic regression models with peri-implant fracture as the dependent variable. Given the low number of events (n = 9), all results should be interpreted as exploratory and hypothesis-generating.
Discussion
This study evaluated patient-specific, anatomical, and implant-related factors associated with peri-implant fracture following ORIF of distal clavicle fractures and AC joint dislocations using a clavicle hook plate. The incidence of peri-implant fracture in this cohort was 3%, which is lower than the 9–11% reported in previous series of hook plate fixation for distal clavicle injuries.3,12,13
Patients with peri-implant fracture were generally older and more often female, and distal clavicle fractures were more frequent in this group. These demographic findings are consistent with existing evidence that advanced age and reduced bone mineral density increase implant-related stress and susceptibility to failure.18,19
Radiographic analysis showed that a lower clavicle-to-plate diameter ratio and a higher plate-to-clavicle length ratio were significantly associated with peri-implant fractures. A lower clavicle-to-plate diameter ratio reflects a thinner clavicle relative to the fixed plate thickness, indicating a poor anatomical match and a greater tendency for localized stress concentration.11,20 A higher plate-to-clavicle length ratio indicates that the plate occupies a larger proportion of the clavicle, increasing the likelihood that it extends into structurally weaker regions, particularly the midshaft. 11 Together, these mismatches between implant and bone anatomy may predispose the clavicle—especially at the medial end of the plate—to increased mechanical stress and a higher risk of fracture.15,21
These findings are consistent with known anatomical variation along the clavicle. The medial end is typically thickest to bear axial loads through the sternoclavicular joint, whereas the lateral end has moderate thickness related to ligamentous attachments and the acromioclavicular joint. In contrast, the middle third is the narrowest and thinnest segment and is the most common site of clavicle fractures. 11 Longer plates are more likely to span this vulnerable midshaft region, which may cause stress concentration at the medial plate end, particularly in patients with lower bone density, thereby increasing the likelihood of peri-implant fracture.4,15,16,18,19
In this study, plates with a greater number of holes, representing longer implants, were more common in patients with peri-implant fracture. Longer plates may span weaker regions of the clavicle and increase the lever arm during shoulder movement, further amplifying stress at the implant–bone interface. These observations align with biomechanical principles indicating that oversized implants in relatively thin bone can act as stress risers and contribute to implant-related complications.17,22
The present results can be integrated with prior reports on hook plate complications. Earlier studies have focused mainly on lateral complications, such as subacromial impingement, rotator cuff lesions, acromial osteolysis, and implant-related pain requiring early removal.9,23 In contrast, this analysis emphasizes the medial portion of the plate and its interaction with clavicular anatomy, thereby extending the understanding of complications associated with hook plate fixation.
Biomechanical work by Hung et al., Lee et al., and Wang et al. has shown that stress distribution around hook plates depends not only on hook angle and depth but also on plate dimensions and their relationship to the underlying bone.15–17 The clinical associations observed in the current cohort are consistent with these biomechanical findings and support the concept that anatomical mismatch between the clavicle and plate can increase complication rates.15–17
Overall, these results agree with previous reports indicating that appropriate implant selection is critical for successful outcomes in clavicular hook plate fixation. Although commercially available hook plates are manufactured in limited standardized sizes, our data suggest that a more individualized approach to implant sizing—taking into account clavicular morphology and patient build—may help reduce mechanical complications. 20
Clinical implications and limitations
The findings of this study primarily support cautious selection of hook plate length and consideration of clavicular morphology, particularly in patients with smaller skeletal frames.11,15–17,21,22 Surgeons should avoid unnecessarily long plates that extend into the midshaft in relatively thin clavicles to reduce potential stress concentration at the medial plate end and the risk of peri-implant fracture.15–17,21,22
Recommendations regarding alternative fixation strategies, implant removal timing, and rehabilitation protocols remain speculative and should be interpreted with caution, as these aspects were not directly evaluated in this cohort. This study also has several limitations that should be acknowledged. It was a retrospective single-center analysis with a small number of peri-implant fracture events, which limits statistical power and precludes robust multivariable adjustment, and radiographic measurements were obtained by a single observer and only verified by a senior surgeon, without formal assessment of inter- or intra-observer reliability, which may introduce measurement error when interpreting the radiographic associations reported in this study. In addition, the study population was heterogeneous, including both distal clavicle fractures and acromioclavicular joint dislocations, which differ in pathology, surgical indications, and biomechanical environment; although diagnosis type was compared between patients with and without peri-implant fracture and showed a significant univariable association, the very small number of events precluded meaningful multivariable adjustment for injury type together with other covariates, and residual confounding by diagnosis cannot be excluded.
Conclusion
In this single-center cohort of 282 patients treated with a clavicle hook plate for distal clavicle fractures and acromioclavicular joint dislocations, peri-implant fractures were uncommon, with an incidence of 3%. These fractures were associated with older age, smaller skeletal build (lower body weight and shorter stature), and dimensional mismatch between the clavicle and implant, including a smaller clavicle-to-plate diameter ratio and the use of longer plates with more holes. These findings suggest that careful consideration of patient morphology and implant dimensions may help reduce the risk of peri-implant fracture following hook plate fixation.
Footnotes
Ethical considerations
All study procedures involving human participants were reviewed and approved by the Institutional Review Board of our institution (IRB number 20250505R).
Consent to participate
Written informed consent was waived by the IRB as the research met the criteria for minimal risk studies, according to relevant guidelines and regulations. All procedures were conducted in accordance with the Declaration of Helsinki and institutional policies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan (NSTC114-2622-E-341-001) and Shin Kong Wu Ho-Su Memorial Hospital, Taiwan (2024SKHADR023). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.