
Abstract
Background:
Rotator cuff muscle atrophy and fatty infiltration are predictors of negative outcomes after rotator cuff repair. However, the impact of muscle degeneration on nonsurgical treatment is unknown.
Hypothesis:
Rotator cuff muscle atrophy and fatty infiltration will reduce the outcomes of operative repair while having a minimal effect on nonsurgical treatment. Additionally, in the setting of atrophy and fatty infiltration, surgical and nonsurgical treatment will produce equivalent outcomes.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients undergoing operative and nonoperative treatment of full-thickness rotator cuff tears were prospectively enrolled into a nonrandomized cohort study. Muscle quality was assessed on magnetic resonance imaging by use of the supraspinatus tangent sign, Warner atrophy, and Goutallier fatty infiltration classifications. Grading was performed by 2 independent observers who were blinded to patient treatment and outcomes. Normalized Western Ontario Rotator Cuff (WORC) index was the primary patient-reported outcome. Multivariate linear regression analysis was used to determine the impact of muscle quality on treatment outcomes.
Results:
The cohort consisted of 157 patients, 89 (57%) surgical and 68 (43%) nonsurgical, with a mean follow-up of 2.4 years (range, 1-5 years). Tangent sign had the best inter- and intrarater reliability, with kappa statistics of 0.81 and 0.86, respectively. Reliability for Warner atrophy was 0.69 to 0.76 and for Goutallier classification was 0.54 to 0.64. Overall, improvement in WORC scores was higher in the surgical group than the nonsurgical group (39.3 vs 21.2; P < .001). A positive tangent sign was the only independent predictor (P < .01) of worse outcomes in the surgical group, accounting for an estimated 22-point lower improvement in WORC scores.
Conclusion:
A positive tangent sign was predictive of worse operative outcomes, resulting in equivalent improvements between surgical and nonsurgical treatment. The tangent sign is a reliable, prognostic indicator that clinicians can use when counseling patients on the optimal treatment of rotator cuff tears.
Keywords
Chronic rotator cuff tears are associated with degenerative changes in the corresponding muscles, which have been classified as atrophy and fatty infiltration. 11,17 Atrophy refers to a loss in muscle volume caused by disuse, whereas fatty infiltration occurs when adipose tissue forms between the muscle pennae. 11,22 The exact cause of fatty infiltration is not fully understood, but it is thought to be due to a combination of mechanical unloading, altered muscle pennate angle, and traction injury to the suprascapular neve in chronic, retracted tears. 4,9,20,22
Although muscle atrophy and fatty infiltration are likely interrelated processes, both have been found to be independent predictors of negative outcomes after rotator cuff repair. 10 Degenerative rotator cuff muscle changes are associated with tissue fibrosis, cellular apoptosis, and a decreased capacity for tendon healing. 5,9,19,22 Additionally, in patients undergoing rotator cuff repairs, atrophy and fatty infiltration are associated with decreased tear reparability, higher retear rates, and lower patient-reported outcomes. 1,2,7,13,21,27
Despite the negative effects of muscle degeneration on rotator cuff repair, it is unclear how the presence of muscle atrophy and fatty infiltration affects clinical practice. One of the challenges is the high variability between observers in assessing rotator cuff muscle quality on magnetic resonance imaging (MRI). 18,25 Furthermore, the impact of fatty infiltration and atrophy on the outcomes of nonsurgical treatment of rotator cuff tears is unknown. Therefore, it is challenging for the clinician to use muscle quality as a prognostic indicator to guide treatment decisions.
In this study, we used prospective, parallel cohorts to investigate the impact of muscle quality on the surgical and nonsurgical treatment outcomes of rotator cuff tears. We hypothesized that atrophy and fatty infiltration will reduce the outcomes of operative repair, while having a minimal effect on nonoperative treatment. Additionally, we hypothesized that in the setting of atrophy and fatty infiltration, surgical and nonsurgical treatment will produce equivalent outcomes.
Methods
Patient Enrollment
This study received approval from our institutional review board. Patients presenting to our institution with rotator cuff tears between 2009 and 2015 were prospectively enrolled into a research registry. To be included in the registry, patients had to be at least 18 years of age and diagnosed with a full-thickness rotator cuff tear on either ultrasonography or MRI. Patients with subscapularis tears or a history of prior ipsilateral shoulder surgery were excluded. Surgical or nonsurgical treatment was chosen by the patients after a discussion with the treating surgeon on the risks and benefits of each option. Operative treatment consisted of arthroscopic rotator cuff repair performed by 4 board-certified shoulder surgeons. The repair technique was left to the discretion of the treating surgeon. Nonoperative treatment consisted of a referral to physical therapy with a standardized rotator cuff rehabilitation protocol consisting of shoulder stretching in all planes, rotator cuff resistance band strengthening, and scapular stabilization exercises. Additionally, patients were treated nonoperatively with anti-inflammatory drugs and periodic steroid injections as needed for symptomatic control.
We identified 316 patients in the registry who had at least 1 year of clinical follow-up: 165 surgical and 151 nonsurgical patients. For the purposes of this study, we included only patients who had a pretreatment shoulder MRI within 1 year of registry enrollment with adequate T1-weighted sagittal-oblique sequences to enable rotator cuff muscle grading. Of the 316 patients, 157 had adequate MRI imaging for inclusion (Figure 1). No significant differences were found in patient demographics or treatment group between the included and excluded patients.
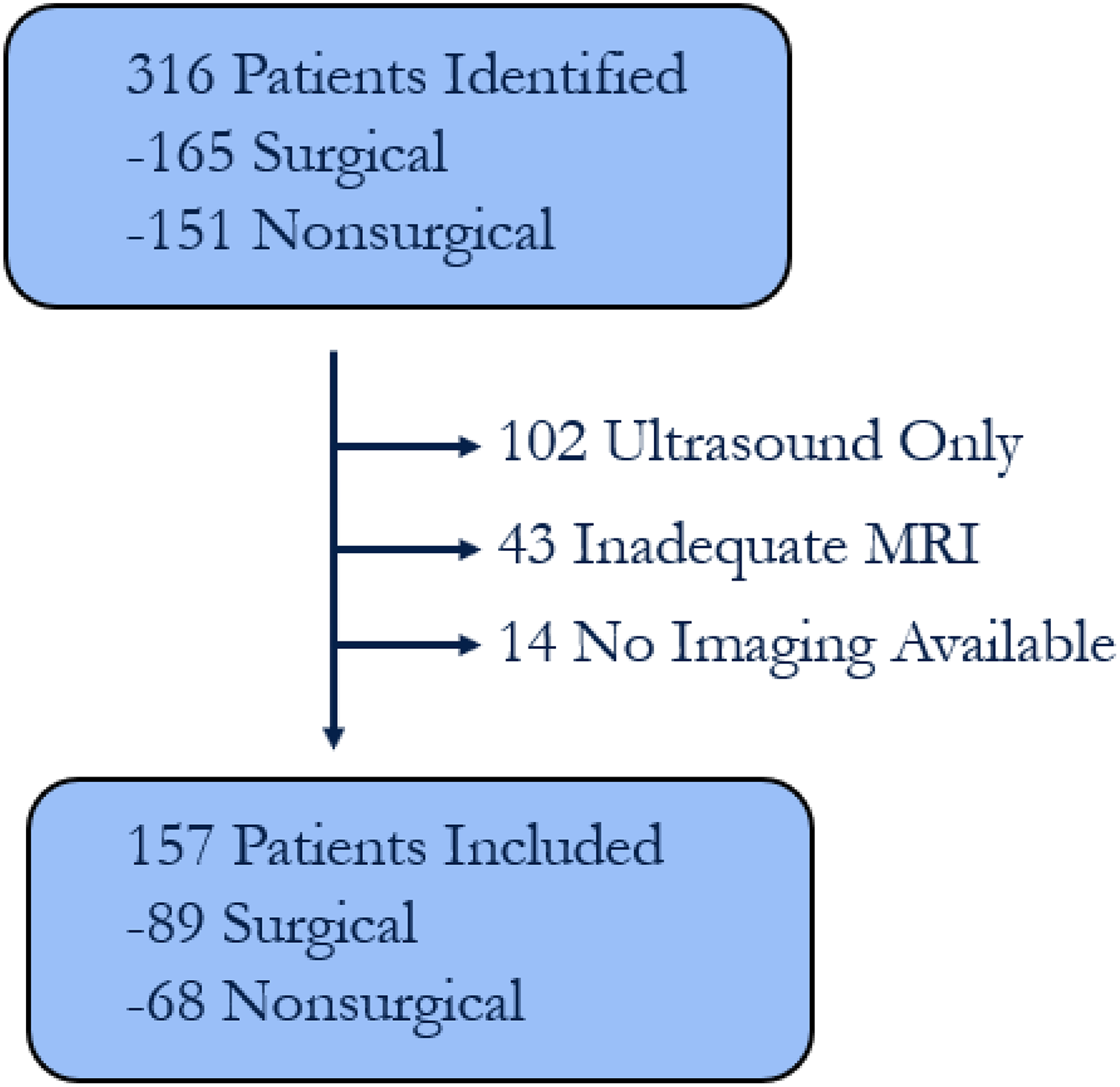
Flowchart of patient selection. MRI, magnetic resonance imaging.
MRI Evaluation
All patients had MRIs performed on at least a 1.5-T magnet with proper T1-weighted sagittal-oblique sequences to enable cross-sectional evaluation of the rotator cuff musculature. Tear size was measured by multiplying the maximal anteroposterior and mediolateral dimensions of the tear to generate the surface area or cuff tear index (CTI). 29 Muscle grading was performed on the most lateral sagittal-oblique cut where the scapular spine was in continuity with the body.
Muscle atrophy was assessed through the use of 2 methods: Warner classification and supraspinatus tangent sign. In the Warner classification, lines are drawn on the sagittal-oblique view between the tip of the coracoid and superior border of the scapular spine and between the superior scapular spine and inferior aspect of the scapula. Atrophy is then determined by the gross amount of muscle above or below these lines and is graded as none, mild, moderate, or severe (Figure 2). 31 The supraspinatus tangent sign was introduced by Zanetti et al. 32 If the supraspinatus muscle belly does not intersect the line connecting the tip of the coracoid to the superior aspect of the scapular spine, then it is considered to have a positive tangent sign indicating muscle atrophy (Figure 3). A positive tangent sign corresponds to moderate or severe atrophy in the Warner classification.

Warner classification for muscle atrophy; illustration from Warner et al. 31 Atrophy is graded using lines drawn between the tip of the coracoid and superior scapular spine and between the superior scapular spine and inferior angle of the scapula. The gross amount of infraspinatus and supraspinatus muscle relative to the line determines the degree of atrophy.
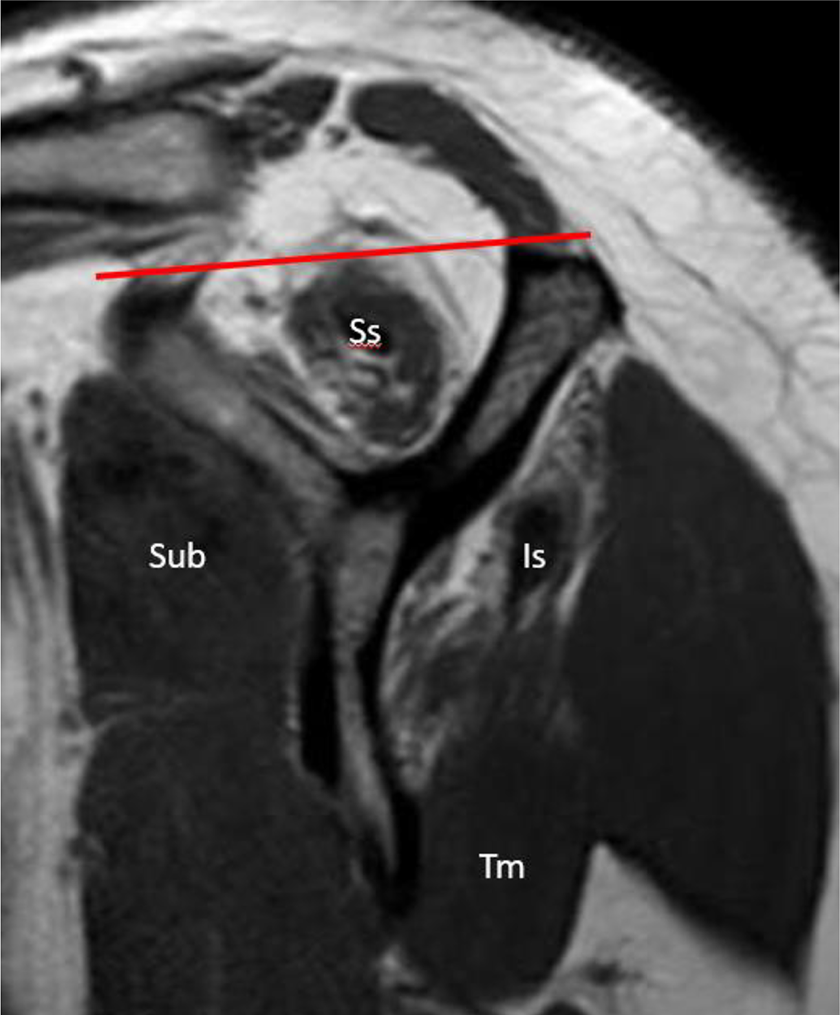
Sagittal oblique, T1-weighted MRI image demonstrating a positive supraspinatus (Ss) tangent sign. Fatty infiltration of the infraspinatus (Is) muscle is also demonstrated, in contrast to normal muscle quality of the subscapularis (Sub) and teres minor (Tm).
Fatty infiltration was graded on the sagittal-oblique T1-weighted sequences for both supraspinatus and infraspinatus from 0 to 4 according to the classification originally described by Goutallier et al 11 and later modified for MRI analysis by Fuchs et al 8 : grade 0, normal muscle; grade 1, some fat streaks; grade 2, fatty infiltration with more muscle than fat; grade 3, equal amounts of fat and muscle; and grade 4, more fat than muscle.
The muscle grading was performed independently by 2 orthopaedic surgery sports medicine fellows (M.N., T.T.) who were blinded to the patient’s information, treatment group, and outcomes. To assess interrater reliability, muscle grading was performed by each grader on all 157 patients. Any discrepancies between graders were resolved by a third assessment performed by the senior author (B.M.). Each grader then re-graded a random subset of 50 patients 4 weeks later to assess intrarater reliability.
Patient-Reported Outcome Measures
Upon enrollment into the cohort, each patient completed a demographic questionnaire in addition to the Western Ontario Rotator Cuff (WORC) index, 14 American Shoulder and Elbow Surgeons (ASES) score, 23 and visual analog scale (VAS) for pain. In this study, the WORC was the primary outcome measure because it is specifically designed and validated for use in patients with rotator cuff tear. 6 We used the normalized version of the WORC index, where 0 is the worst outcome and 100 is the best. Outcome measures were collected at 6 months, 12 months, and then annually thereafter.
Statistical Methods
Descriptive and inferential statistics were analyzed with SPSS v 22 (IBM). The Student t test was used to evaluate differences between the treatment groups at baseline and final follow-up. Kappa statistics were calculated for muscle inter- and intrarater reliability. A regression analysis was performed to assess the relative contribution of each muscle quality measure on change in normalized WORC scores. First, a mixed-effects regression model was generated using the 4 different treating surgeons as the random variable and change in WORC norm as the primary outcome variable. The treating surgeon was found to have no substantial effect on outcomes. Therefore, we proceeded with a multivariate linear regression analysis that controlled for both baseline WORC scores and follow-up duration. Age, sex, cuff tear index, and each muscle quality factor were used as independent variables. For the purpose of the regression, muscle atrophy was grouped as either none or present (mild, moderate, or severe) and fatty infiltration was grouped by grades 0 and 1 versus grade 2 or higher. 10 Separate multivariate linear regression models were constructed for the surgical and nonsurgical groups. P values less than .05 were considered significant.
Results
Of the 316 patients initially identified with rotator cuff tear, 157 patients met the inclusion criteria. There were 89 (57%) surgical and 68 (43%) nonsurgical patients, with a mean follow-up of 2.4 years (range, 1-5 years). Table 1 compares the baseline characteristics of the surgical and nonsurgical groups. At presentation, nonsurgical patients on average were 5 years older (63.2 vs 58.4, P < .01) and had a nonsignificant trend toward having larger tears (4.5 vs 3.3 cm2, P = .054) compared with surgical patients. No baseline differences were found in WORC, ASES, or VAS scores between the 2 groups.
Baseline Characteristics of the Surgical and Nonsurgical Groups a

a Bolded P value indicates statistically significant difference between groups (P < .05). Except as noted, values are expressed as mean ± SD. ASES, American Shoulder and Elbow Surgeons score; CTI, cuff tear index; WORC, Western Ontario Rotator Cuff index; VAS, visual analog scale.
The reliability of the muscle grading measures is displayed in Table 2. The tangent sign demonstrated the best inter- and intrarater reliability, with kappa statistics of 0.81 and 0.86, respectively. The reliability of the Warner atrophy grading ranged from 0.69 to 0.76, and Goutallier classification had the worst reliability, with kappa statistics of 0.54 to 0.64. The pretreatment muscle quality characteristics were not significantly different between the surgical and nonsurgical groups (Table 3).
Muscle Grading Reliability a
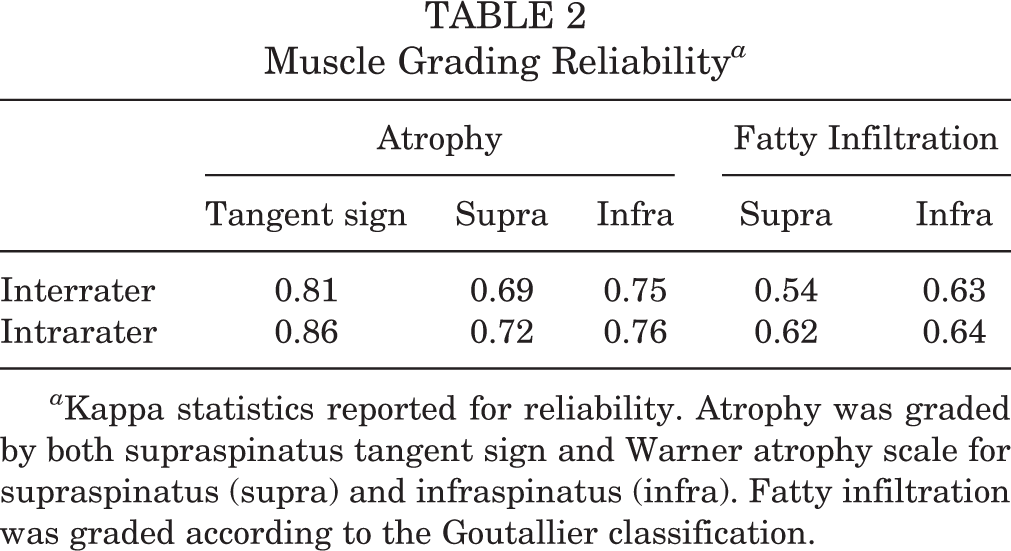
a Kappa statistics reported for reliability. Atrophy was graded by both supraspinatus tangent sign and Warner atrophy scale for supraspinatus (supra) and infraspinatus (infra). Fatty infiltration was graded according to the Goutallier classification.
Muscle Quality of Surgical and Nonsurgical Groups a

a Comparison of preoperative muscle quality between the surgical and nonsurgical groups. Values are expressed as n (%).
The outcomes of the surgical and nonsurgical groups are shown in Table 4. Overall, the change in normalized WORC scores were higher in the surgical group compared with the nonsurgical group (39.3 vs 21.2, respectively, P < .001). When outcomes were compared based on muscle quality factors, the surgical group continued to significantly outperform the nonsurgical group in every subset except in the setting of a positive supraspinatus tangent sign (P = .13).
Improvements in Normalized WORC Scores a

a Improvement from baseline Western Ontario Rotator Cuff (WORC) scores at final follow-up. Values are expressed as mean ± SD. Bolded P values indicate statistically significant difference between groups (P < .05). FI, fatty infiltration.
The multivariate linear regression models for the surgical and nonsurgical groups are shown in Tables 5 and 6, respectively. In the surgical group, a positive tangent sign was the only significant predictor of worse outcomes (P < .01), accounting for an estimated 22-point worse outcome in normalized WORC scores. In the nonsurgical group, none of the muscle quality factors had a significant impact on patient outcomes. Age, sex, and CTI did not have a significant effect on patient outcomes in the regression analysis for either the surgical or nonsurgical groups.
Surgical Multilinear Regression Analysis Table a

a Bolded P value indicates statistical significance (P < .05). CTI, cuff tear index; FI, fatty infiltration.
Nonsurgical Multilinear Regression Analysis Table a

a CTI, cuff tear index; FI, fatty infiltration.
Discussion
In our study, we observed that patients who chose to undergo surgical repair had on average an 18-point better improvement in normalized WORC scores than patients who chose nonsurgical treatment, exceeding the previously reported minimal clinically important difference (MCID) of 11.7. 15 The improvement of the surgical group compared with the nonsurgical group was significantly greater in the setting of both atrophy and fatty infiltration, with the exception of a positive supraspinatus tangent sign. When the supraspinatus tangent sign was positive, the difference between the surgical and nonsurgical groups did not reach statistical significance or the MCID. Regression analysis further confirmed that a positive tangent sign had an estimated 22-point negative effect on normalized WORC scores, even when accounting for age and tear size.
Previously, atrophy and fatty infiltration have been reported to reduce repair success and patient-reported outcomes. After describing fatty infiltration, Goutallier et al 12 reported a series of 220 patients who underwent open repairs and had computed tomography scans performed at an average of 3 years postoperatively to assess repair integrity. Those investigators found that all patients with fatty infiltration of at least grade 2 averaged across the rotator cuff muscles had evidence of retear compared with a 19% rate in patients without fatty infiltration. Meanwhile, Thomazeau et al 30 showed that patients with decreased supraspinatus muscle volume on preoperative MRI had higher retear rates and worse outcomes after cuff repair. Gladstone et al 10 found both atrophy and fatty infiltration to be independent negative predictors of decreased strength, patient-reported outcomes, and repair integrity. Conversely, Burkhart et al 1 reported good outcomes of rotator cuff repair even in the setting of stage 3 or 4 fatty infiltration.
One of the challenges of assessing atrophy and fatty infiltration, in both research and clinical practice, is the poor grading reliability between observers. Using MRI images, Lippe et al 18 reported kappa values of 0.41 for fatty infiltration and less than 0.37 for atrophy between 3 independent, board-certified shoulder surgeons. Others have reported interobserver agreement between 0.36 and 0.68 for fatty infiltration and between 0.25 and 0.59 for atrophy. 3,25,28 The tangent sign offers a simplified and reliable way to quickly evaluate supraspinatus muscle atrophy, with interobserver agreement reported to be as high as 0.87. 26 In our study, we found similar interobserver reliability, with tangent sign having the highest interrater reliability of all the measures at 0.81.
Recent randomized controlled trials have demonstrated only a modest benefit of rotator cuff repair over physical therapy. 16,24 Therefore, it is important to identify which patients will benefit from surgical versus nonsurgical treatment of rotator cuff tears. We hypothesized that muscle quality would be an important prognostic indicator because it has been shown to affect the healing capacity of the rotator cuff. 5,9 Furthermore, even in the setting of a successful cuff repair, reversal of muscle atrophy and fatty infiltration may not occur. 10 Future studies on treatment of rotator cuff tears should examine and quantify muscle quality to determine whether similar results are found.
In contrast to these recent randomized trials, we found that patients saw a significantly greater improvement in outcomes after rotator cuff repair compared with nonsurgical treatment. To our knowledge, this is the first study to use muscle quality to compare surgical and nonsurgical treatment of rotator cuff tears. One of the strengths of our study is the use of a rigorous, blinded, muscle quality grading protocol that allowed us to assess 3 different classifications for atrophy and fatty infiltration. Additionally, we used WORC as our primary outcome, which is a scale that was specifically designed and validated for use in rotator cuff repairs and has increased responsiveness to rotator cuff treatment. Overall, we found that supraspinatus tangent sign was both the most reliable muscle quality measurement and the strongest predictor of worse outcomes following operative repair.
Our study had limitations that should be noted. First, this was not a randomized study. Patients could choose between surgical and nonsurgical treatment, making our results vulnerable to a selection bias. Although we accounted for basic demographics and cuff tear size in our regression analysis, fundamental differences between treatment groups may have been present that could not be accounted for, such as activity level. Another limitation is that we could not standardize the preoperative MRIs because several MRIs were obtained at outside facilities. Although differences in MRI magnet strength and protocols may have affected our muscle grading reliability, they likely provide a more accurate reflection of clinical practice. Finally, repair integrity was not assessed via follow-up imaging. Therefore, we cannot comment on whether repair integrity correlated with outcomes.
Conclusion
In a nonrandomized, prospective cohort of patients with full-thickness rotator cuff tears, arthroscopic repair resulted in superior outcomes compared with nonsurgical treatment. Supraspinatus tangent sign proved to be the most reliable method of assessing rotator cuff muscle quality, followed by Warner atrophy classification and then Goutallier fatty infiltration grade. A positive tangent sign was predictive of worse operative outcomes, resulting in equivalent benefits of surgical and nonsurgical treatment. In clinical practice, the tangent sign is a prognostic indicator that can be used to counsel patients on the optimal treatment of rotator cuff tears.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B. has received consulting fees from Arthrex, Smith & Nephew, and Stryker; royalties from Arthrex; speaking fees from Arthrex and Smith & Nephew; and educational support from the CDC. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Michigan Institutional Review Board (study No. HUM00024612).