
Abstract
Background:
Glenohumeral instability is common in athletes. There are an estimated 0.12 episodes of instability per 1000 sporting exposures. Instability can lead to time away from sport and an increased risk of shoulder arthritis.
Purpose:
To determine the prevalence, demographic data, anatomic features, and likelihood of surgery for the different types of instability as defined by the FEDS (frequency, etiology, direction, and severity) classification system for different sports.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Databases at 3 institutions (University of Iowa, Vanderbilt University, and University of Pennsylvania) were searched for International Classification of Diseases--Ninth Revision codes related to shoulder instability in 2010. Demographic data, symptoms, causes, imaging findings, and operative reports were obtained. Data were entered into a custom-designed REDCap online survey. Patients with subjective instability related to sporting activities were included for analysis.
Results:
A total of 184 athletes had glenohumeral instability; 20.1% were female. The mean age at the time of the first instability episode was 19.0 years for both male and female patients. The most common sports were football (29.3%), basketball (19.0%), and wrestling (9.8%). The most common type of instability based on the FEDS system was occasional, traumatic, anterior dislocation. Surgery was performed on 69.6% of athletes, and 14.1% had a recurrence of instability after surgery overall. Football had the highest rate of recurrence postoperatively at 23.8%. There was no difference in surgery rates between athletes with subluxations versus dislocations (P = .8458). Surgery was significantly more likely in those with frequent dislocations (P < .0001) and posterior instability (P = .027). There was a 10.7% recurrence rate overall with conservative treatment.
Conclusion:
Glenohumeral instability most commonly occurs in contact sports, affects male more than female patients, and is most frequently in the anterior direction. Recurrent instability is most common in football players. Attention should be turned to the specific characteristics of each type of instability to determine the best treatment for each athlete.
Glenohumeral instability is common in sporting activities. In collegiate athletes, instability episodes have been reported to occur at a rate of 0.12 per 1000 sporting exposures. 11 Instability can lead to time away from sport, which can be difficult, as athletes place significant importance on sport and desire a quick return to play. In a study of National Collegiate Athletic Association (NCAA) athletes, 45% required at least 10 days away from sport secondary to an instability episode. 11 Glenohumeral instability also leads to increased rates of arthritis and disability in the shoulder, 3,9 negatively affecting the athlete for life.
Contact sports are most commonly associated with shoulder instability. Sports such as football, wrestling, ice hockey, and rugby have been shown to have the highest rates of instability events. 1,11 Previous studies have shown that the majority of instability events are anterior and that there is a high recurrence rate. 1,4,11,12
The purpose of this study was to understand the epidemiology of shoulder instability related to different sports using the FEDS (frequency, etiology, direction, and severity) classification system of glenohumeral instability. 6,7 The FEDS system has high interrater and intrarater agreement and is the only classification system based on a systematic review of the literature and a survey of experts. 7 We also sought to evaluate how successful current treatments for instability are in the athletic population. Understanding the epidemiology and success of our current treatments will allow us to better treat athletes with glenohumeral instability in the future.
Methods
Institutional review board approval was obtained at 3 institutions: University of Iowa, University of Pennsylvania, and Vanderbilt University. The International Classification of Diseases–Ninth Revision (ICD-9) codes related to shoulder instability for the year 2010 were queried at all 3 institutions (Table 1). Each chart was retrospectively reviewed, and demographic data, causes, symptoms, imaging findings, and operative reports were obtained. Indications for imaging were not standardized, although almost all patients underwent radiography and many underwent magnetic resonance imaging (MRI) or computed tomography. We collected information on patients across the entire institution (all departments) to determine the incidence of shoulder instability for all patients presenting to a clinic/hospital. Data were entered into a custom-designed REDCap online survey. The survey included questions on basic demographic data, nature of instability, sport participation, imaging results, surgical technique, and any history of subsequent instability. There was no standardization of imaging, treatment, or surgical indication, making this a true epidemiological cross-sectional study of actual practice. Follow-up frequency and duration were not consistent among institutions or patients. Patients were excluded from analysis if there was no subjective feeling of instability, if they were not able to be clearly defined by the FEDS system, or if their instability did not result from playing a sport.
International Classification of Diseases–Ninth Revision (ICD-9) Codes a

a NEC, not elsewhere classified; NES, not elsewhere specified; NOS, not otherwise specified.
Study Definitions
As described by Kuhn et al, 7 the 4 parts of the FEDS system have the following definitions. “Frequency” is defined as the number of instability episodes in the preceding year. There are 3 possibilities: solitary (1 episode), occasional (2-5 times/year), and frequent (>5 times/year). “Etiology” is related to a history of trauma. If the first episode of instability was related to an injury, it was considered to be traumatic as opposed to atraumatic. “Direction” is related to the primary direction of instability and can be anterior, posterior, or inferior. Provocative testing in the clinic can be used to determine the direction that most closely replicates the patient’s symptoms. Finally, “severity” is either a dislocation or a subluxation. If the patient needed assistance at any time to reduce the shoulder, this was considered a dislocation. Self-directed reduction maneuvers were considered subluxations. Accounting for each combination, there are 36 possible types of instability, with 15 combinations being extremely uncommon. 7
Results
Study Population
We identified 1537 patients with ICD-9 codes related to shoulder instability; 894 were excluded secondary to no subjective feeling of instability (errors in coding, not instability patients), and 260 were excluded secondary to missing data in the FEDS system. This left 383 total patients who were able to be clearly defined by the FEDS system (59.6%). Of these, 184 occurred during a sporting activity (48.0%). There were 147 male (79.9%) and 37 female (20.1%) patients. The mean age at the time of the first instability episode was 19.0 years for both male and female patients. Football was the most common sporting activity that led to instability, accounting for 29.3%. This was followed by basketball (19.0%) and wrestling (9.8%). These data can be seen in Table 2.
Prevalence of Shoulder Instability by Sport (N = 184 Athletes)

a Sample sizes apply to each sport in the row individually, rather than collectively.
The most common frequency of episodes was occasional with 73 athletes (39.7%), followed by solitary (33.1%) and frequent (27.2%). Trauma was the etiology in 97.8% of athletes. Anterior instability (82.6%) was the most common direction, followed by posterior (16.9%) and inferior (0.5%). Dislocations accounted for 50.5% of the severity. The most common type of instability according to the FEDS system was occasional, traumatic, anterior dislocation with 40 athletes (21.7%), followed by single, traumatic, anterior dislocation with 32 athletes (17.4%). These data can be seen in Figure 1.
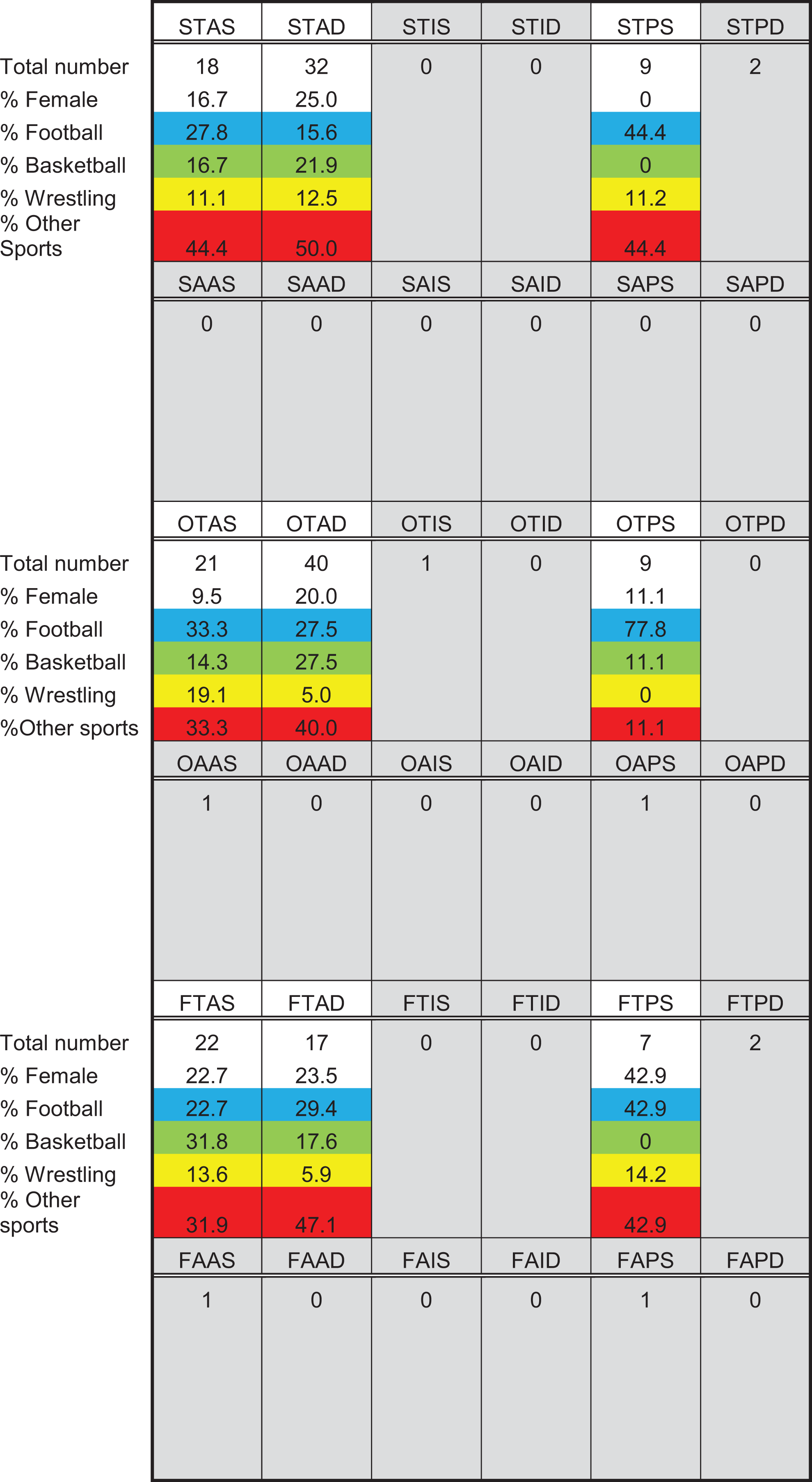
FEDS (frequency, etiology, direction, and severity) classification table. The first letter in each cell heading indicates frequency (single [S], occasional [O], or frequent [F]); the second indicates etiology (traumatic [T] or atraumatic [A]); the third indicates direction (anterior [A], inferior [I], or posterior [P]), and the fourth indicates severity (subluxation [S] or dislocation [D]).
The majority of the athletes underwent surgery (69.6%). Of those who underwent surgery, 14.1% had recurrent instability. Of those who did not undergo surgical procedures, 10.7% had recurrent instability. Those with frequent dislocations were more likely to undergo surgery than those with solitary or occasional dislocations (83.5% vs 43.6%, respectively; P < .0001). Posterior instability was more likely to be operative than anterior instability (71.4% vs 61.1%, respectively; P = .027). There was no difference in surgical rates for athletes with subluxations versus dislocations (62.7% vs 60.2%, respectively; P = .8458).
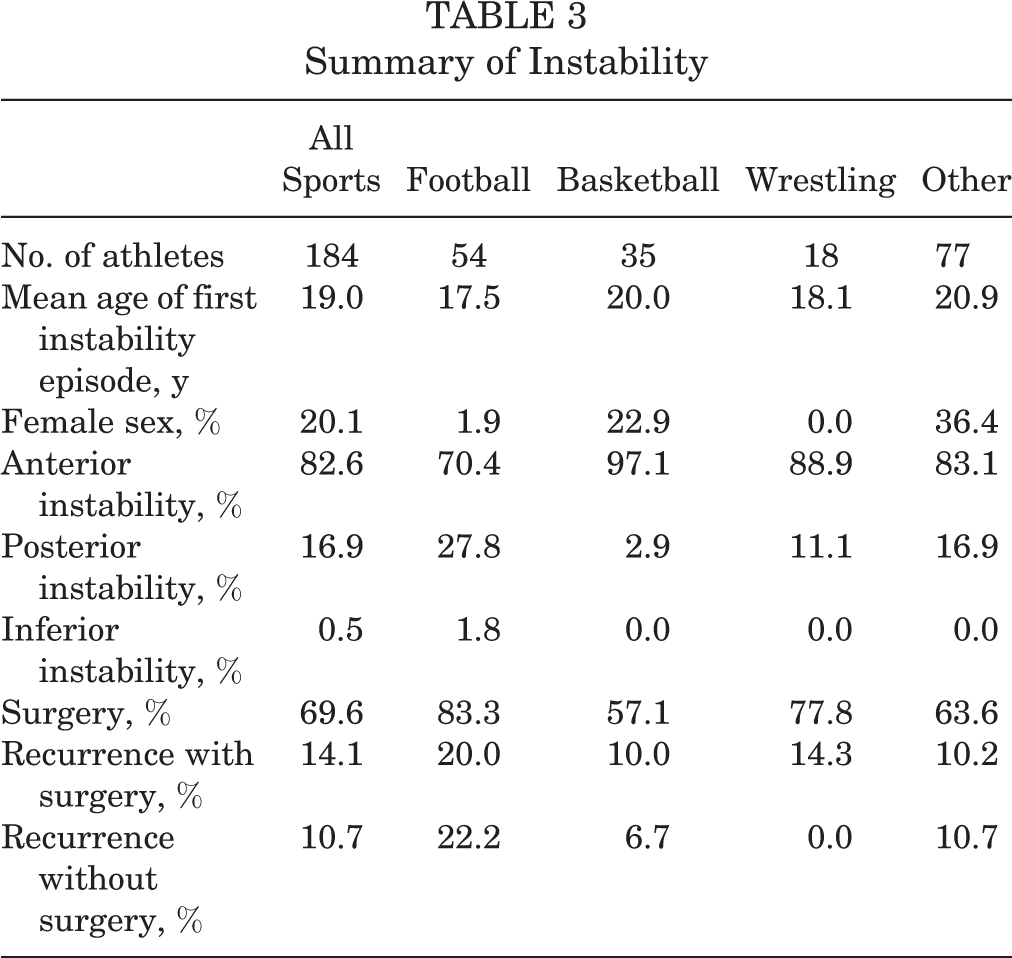
A summary of the findings overall and for football, basketball, and wrestling can be seen in Table 3, with radiographic findings by sport in Table 4.
Summary of Instability
Radiological Findings by Sport a
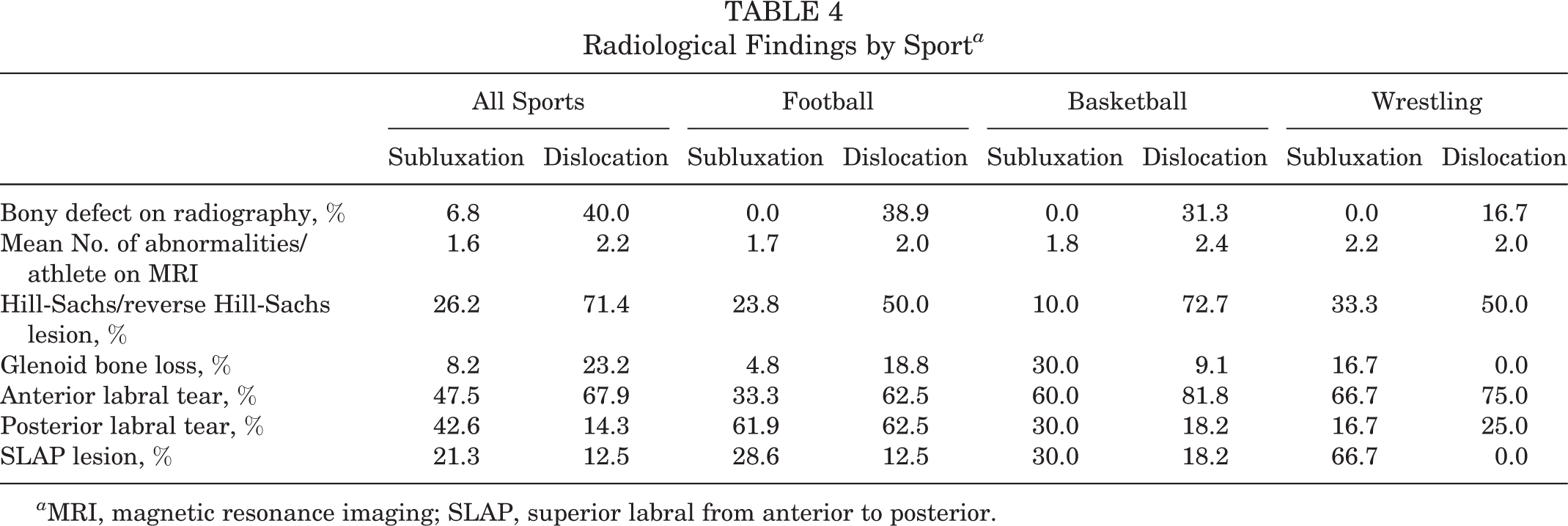
a MRI, magnetic resonance imaging; SLAP, superior labral from anterior to posterior.
Football
The vast majority of the athletes seen in football were male, with 53 male athletes and 1 female athlete. The mean age at the time of the first instability episode was 17.5 years. The most common frequency was occasional (48.1%), followed by solitary (27.8%) and frequent (24.1%). All of the instability episodes were traumatic in nature. Anterior instability was most common (70.4%), followed by posterior (27.8%) and inferior (1.9%). Most episodes were related to subluxations (59.2%). The most common type of instability according to the FEDS system was occasional, traumatic, anterior dislocation.
Plain radiographs were available for 20 athletes with a history of subluxation instability and 18 athletes with dislocations. There were no bony abnormalities seen in the subluxation group, and 7 dislocating athletes had abnormalities, with the most common being a defect on the humeral side only (85.7%). MRI scans were available for 21 athletes with subluxations and 16 athletes with a history of dislocations. There was a mean of 1.7 imaging abnormalities per athlete in the subluxation group, with posterior labral tear (61.9%), anterior labral tear (33.3%), and superior labral from anterior to posterior (SLAP) lesion (28.6%) being the most common. For the dislocation group, there was a mean of 2.0 abnormalities per person. The most common lesions were anterior labral tear (62.5%), Hill-Sachs lesion (50.0%), and anterior glenoid bone loss (18.8%).
Surgery was performed on 45 of the 54 football athletes (83.3%). In the subluxation group, 75.0% underwent surgery. The most common procedures were posterior labral repair (66.7%), anterior labral repair (50.0%), and SLAP repair (12.5%). Four of the 24 (16.7%) who underwent surgery had recurrent instability, compared with 2 of the 8 (25.0%) who were treated nonoperatively. For the dislocation group, 95.5% underwent surgery. Anterior labral repair (85.7%) was the most common procedure, followed by anterior capsule plication (23.8%), SLAP repair (14.3%), and remplissage (14.3%). Five of the 21 (23.8%) had recurrent instability, compared with 1 of 1 (100.0%) who was treated nonoperatively.
Basketball
There were 27 male and 8 female athletes in the basketball group. The mean age at the time of the first instability episode was 20.0 years. The most common frequency was occasional (42.8%), followed by solitary and frequent (28.6% each). Trauma accounted for 100.0% of the instability episodes. The vast majority had anterior instability (97.4%), with only 1 athlete (2.9%) experiencing posterior instability. Most episodes of instability were dislocations (60.0%). The most common type of instability was occasional, traumatic, anterior dislocation (31.4%).
Plain radiographs were available for 10 athletes with a history of subluxations only and 16 patients with dislocations. There were no bony abnormalities seen in the subluxation group. Five of the 16 patients (31.3%) with dislocations had bony abnormalities, with 60.0% having a humeral defect only. MRI scans were available for 10 athletes with subluxations and 11 athletes with dislocations. There was a mean of 1.8 lesions in the subluxation group. The most common abnormality seen was anterior labral tear (60.0%). A Hill-Sachs lesion, posterior labral tear, and SLAP lesion were seen in 30.0% of athletes. For the dislocation group, a mean of 2.4 lesions were seen per athlete. The most common was anterior labral tear (81.8%), Hill-Sachs lesion (72.7%), and supraspinatus tear (36.4%).
Surgery was performed on 20 of 35 (57.1%) basketball athletes overall. In the subluxation group, 80.0% underwent surgery, and a mean of 2.5 procedures were performed. Anterior labral repair was the most common procedure (75.0%), followed by anterior capsule plication (50.0%), posterior labral repair (37.5%), and interval closure (37.5%). There was no recurrence of instability in the surgical or nonsurgical group. In the dislocation group, 57.1% of athletes underwent surgery. A mean of 2.3 procedures were performed, with the most common being anterior labral repair (75.0%). This was followed by posterior labral repair (41.7%) and anterior capsule plication (33.3%). Two of 12 athletes in the surgical group had recurrent instability, while 1 of 9 in the nonsurgical group had recurrent instability.
Wrestling
All 18 athletes were male, with a mean age at the time of the first instability episode of 18.1 years. The most common frequency was single (38.9%), followed by occasional (33.3%) and frequent (27.8%). Trauma accounted for 100.0% of the instability episodes. Anterior instability accounted for 88.9%, with posterior instability only accounting for 11.1%. The majority of instability events were subluxations (61.1%) as opposed to dislocations (38.9%). The most common types of instability according to the FEDS system were occasional, traumatic, anterior subluxation and single, traumatic, anterior dislocation, with 4 athletes each (22.2%).
Plain radiographs were available for 10 athletes with subluxation instability and 6 athletes with dislocations. There were no abnormalities seen in the subluxation group, and 1 athlete in the dislocation group had both a humeral head and glenoid defect. MRI scans were available for 6 athletes with subluxations and 4 athletes with dislocations. There was a mean of 2.2 lesions per athlete in the subluxation group, with the most common lesions being anterior labral tear (66.7%) and SLAP lesion (66.7%). In the dislocation group, there was a mean of 2.0 lesions per athlete, with the most common being anterior labral tear (75.0%) and Hill-Sachs lesion (50.0%).
Surgery was performed on 14 of 18 athletes (77.8%) overall. In the subluxation group, 81.8% underwent surgery, and a mean of 2.9 procedures per athlete was performed. The most common procedures were anterior capsule plication (55.6%), interval closure (55.6%), anterior labral repair (44.4%), and SLAP repair (44.4%). Two of the 14 (14.3%) who underwent surgery had a recurrence of instability, and 1 of 2 (50.0%) in the nonsurgical group had a recurrence of instability. In the dislocation group, 71.4% underwent surgery, with a mean of 1.0 procedures performed per athlete. The most common procedures were anterior labral repair (80.0%), interval closure (80.0%), and anterior capsule plication (60.0%). There was no recurrence of instability in either the surgical or the nonsurgical group.
Discussion
Shoulder instability is common in athletics, especially in contact sports. In 1 study, 88% of glenohumeral instability events were related to contact with either another athlete or an object. 4 In our series of patients, the most common sports with instability were football, basketball, and wrestling, and almost all injuries resulted from trauma. Previous analyses of sports have shown that football, ice hockey, and wrestling were the most injurious sports. 4 Our study had very few hockey injuries, which is likely explained by the institutions involved and the popularity of the sport in those geographic areas.
It has previously been reported that male patients are more likely to experience glenohumeral instability. A male-to-female ratio between 1.1:1 to 5.1:1 has been noted in the general population. 2,5,10,13 –15 In the younger, more active population, a ratio as high as 6.3:1 has been reported. 12 Our male-to-female ratio was 4.0:1, which is consistent with previously reported ratios.
The most common direction for instability in our population was anterior (82.6%). This is comparable with a study by Owens et al 12 in young military recruits (88%). Of those with dislocations, 95.7% were anterior. Previous reports range from 88% to 98%. 5,14,15 When comparing sports, both basketball and wrestling had predominately anterior instability. This is likely related to the arm position being in an abducted and externally rotated position. For football, 27.8% of the instability events were in the posterior direction. This is likely accounted for by linemen, who block with their arms in front of their body, leading to a posteriorly directed force of their humeral head. In a report by Mair et al, 8 8 of the 9 athletes with posterior labral injuries confirmed by arthroscopic surgery were football linemen.
Most reports on glenohumeral instability focus on dislocations, as many people with subluxation instability do not seek medical attention. The report by Owens et al 12 on young military recruits did follow both types. They found that a very high percentage (85%) had subluxation instability. 12 In our cohort, 49.5% experienced subluxation instability. The difference could be related to the sports involved. In the Owens et al cohort, boxing was part of the mandatory physical education class for male participants. They noted that all instances of instability in this sport occurred during a missed punch and resulted in anterior shoulder subluxation. 12
Pathological lesions were seen both on plain radiography and on MRI. On plain radiography, 21.7% had a Hill-Sachs lesion and 2.3% had a reverse Hill-Sachs lesion. On the glenoid side, 4.7% had a bony Bankart lesion and 0.8% had a reverse bony Bankart lesion. These results are very similar to a study by Owens et al 11 on collegiate athletes, with 13.0% of their cohort having a Hill-Sachs lesion, 0.0% having a reverse Hill-Sachs lesion, 16.7% having a bony Bankart lesion, and 0.9% having a reverse bony Bankart lesion. On MRI, there were more lesions, on average, for those with dislocations as opposed to subluxation instability (2.2 vs 1.6 lesions/athlete, respectively). Overall, 47.9% had a Hill-Sachs lesion or reverse Hill-Sachs lesion. This is very comparable with the report by Owens et al 12 of 51%. In our cohort, there were more bony lesions seen in the dislocation group compared with the subluxation group. Both groups of instability also saw a large number of labral lesions, which was the most common abnormality seen on MRI.
The majority of our athletes underwent surgery. The mean number of coded procedures during surgery was 2.5 for the subluxation group and 2.3 for the dislocation group. Previous studies looking at instability related to both dislocations and subluxations did not report surgical rates, so it is difficult to estimate the prevalence of surgery among athletes. More detailed studies on specific teams and positions will need to be conducted to determine the best treatment for the type of instability in a given position.
The main limitation of this study is that it is retrospective in nature. The quality of the data depends on the accuracy of clinical notes. We had to exclude a large number of patients secondary to missing information. Another limitation is that all of the participating sites were university-based practices, which take care of university teams, and also tertiary referral centers and, as such, may not reflect usual general practice or routine shoulder instability cases. This could potentially introduce selection bias with a higher percentage of athletes and more complex cases. There was not consistent imaging, treatment, and follow-up because of the retrospective nature of the study. This can be interpreted as a limitation or strength, as it tells us what is naturally occurring across all providers in these institutions. Additionally, there was a lack of consistent imaging, treatment, and follow-up between patients and institutions. The specifics of surgical procedures were also not captured. Last, 2 of the institutions are in states where wrestling is very popular, and therefore, it may be overrepresented in this study.
The strengths of this study are that it involves 3 separate institutions from different parts of the country, including all departments, for an entire year. This allowed for the inclusion of a large number of athletes who were treated by a variety of physicians. This also is the first study of this kind in a nonmilitary population, making it more generalizable. There were also a large number of athletes from different sports, allowing better understanding of the type of instability seen in each sport.
Conclusion
Glenohumeral instability most commonly occurs in contact sports, affects male more than female patients, and is most frequently in the anterior direction. Attention should be turned to the specific characteristics of each type of instability and the demands of the particular sport to determine the best treatment for each athlete.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.W. has received educational support from Synthes and hospitality payments from Stryker and Smith & Nephew. S.J. has received educational support from Arthrex, Gemini Mountain Medical, and Smith & Nephew and research support from Arthrex and DJO. J.C. has received research support from AlloSource, Anika Therapeutics, and Vericel; has received honoraria from Vericel; has received consulting fees from Vericel; and is a paid associate editor for The American Journal of Sports Medicine. B.R.W. has received educational support from Conmed Linvatec, Smith & Nephew, and Wardlow Enterprises; has received consulting fees from Conmed Linvatec; and is the owner/founder of SportsMed Innovate. C.M.H. has received research support from Zimmer Biomet, consulting fees from Pacira, and hospitality payments from Arthrex and Tornier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Iowa Institutional Review Board (No. 201111745).