
Abstract
Background:
Surgeon caseload has been shown to affect both health and economic outcomes in arthroscopic rotator cuff repair. Although previous studies have investigated disparities in access to care, little is known about disparities between low- and high-volume surgeons and facilities.
Purpose:
To identify where disparities may exist regarding access to high-volume surgeons and facilities.
Study Design:
Cross-sectional study.
Methods:
Univariate analysis was performed to analyze differences in the caseload between low- and high-volume surgeons and facilities. Cutoff values were set at 50 cases per year for high-volume surgeons and 125 cases annually for high-volume facilities. Multiple linear regression was then used to develop a cost model incorporating all variables significant under univariate analysis. We collected 18,616 cases with Current Procedural Terminology code 29827 (“arthroscopic rotator cuff repair”) from the 2014 Florida State Ambulatory Surgery and Services Databases.
Results:
A greater proportion of the caseload for low-volume surgeons and facilities was composed of patients who were of lower socioeconomic status, had government-subsidized insurance, or lived in areas with low-income ZIP codes. Low-volume surgeons and facilities also had higher total charges, higher postoperative admission rates, and lower distal clavicle excision rates (P < .001). In our cost model, a low facility volume significantly increased costs. Subacromial decompression, postoperative admission, distal clavicle excision, male sex, and government-subsidized insurance were all significant factors for increased costs in multivariate cost analysis.
Conclusion:
There are disparities in access to high-volume surgeons and facilities for patients undergoing arthroscopic rotator cuff repair in Florida. Patients with a lower socioeconomic status, government-subsidized insurance, and low income all faced decreased access to these high-volume groups. High-volume surgeons and facilities were associated with lower total charges, higher rates of distal clavicle excision, and lower readmission rates. Low-volume facilities added a significant amount of cost, even when controlling for all other significant variables. It is important for providers to be aware of these disparities and work to address them in their own practices.
Rotator cuff repair (RCR) is one of the most commonly performed surgical procedures by orthopaedic surgeons 15 and has been proven to be highly effective. 25 There are an estimated 250,000 outpatient RCR procedures performed every year, the majority of which are performed arthroscopically. 17 The incidence of RCR is also rising steadily. 6,28
It has previously been shown that physicians who perform a higher volume of RCR procedures tend to have lower costs, less time in the operating room, lower readmission rates, and lower complication rates leading to reoperations. 15,22,26 Facility volume has also been examined. Sherman et al 22 found that hospital volume was not a risk factor for readmissions, although their data included both open and arthroscopic RCR procedures and covered the time period from 1997 to 2002. Hospital volume has been found to be significant for a number of inpatient orthopaedic surgical procedures; studies have shown that a higher facility volume is associated with lower revision surgery rates, lower mortality rates, fewer complications, and a shorter length of stay. 9,11,19 However, few studies have examined facility volume and surgeon caseload volume for arthroscopic RCR with respect to their potential impacts on cost.
This study examined disparities between low- and high-volume surgeons and facilities using the State Ambulatory Surgery and Services Databases (SASD), a highly comprehensive source on outpatient procedures. 13 Although previous studies have investigated disparities in access to surgery across demographic groups, this study investigated disparities in both access to care and surgical outcomes for different demographic groups by caseload. 3,14,20,27 We hypothesized that patients of lower socioeconomic status will have less access to high-volume surgeons and have greater rates of hospital admissions after arthroscopic RCR. We also hypothesized that high-volume facilities and surgeons will have significantly lower costs for arthroscopic RCR.
Methods
Data Source
This study utilized the 2014 SASD from Florida. Florida is unique in the SASD in that it is one of the only states that provides identifiers so the caseload can be determined for surgical centers as well as physicians. The SASD is one of a number of databases developed under the Healthcare Cost and Utilization Project (HCUP). 13 Sponsored by the Agency for Healthcare Research and Quality, the HCUP databases form a comprehensive data source on health care. Specifically, 168 data points are provided for every patient encounter on a number of patient demographics, procedure codes, diagnosis codes, and surgical variables.
Data Collection
Every case that used Current Procedural Terminology (CPT) code 29827 (arthroscopically aided RCR) was included. Surgeon volume and facility volume were calculated using unique identifiers. Variables were then divided into patient characteristics and surgeon-specific factors. Patient variables included race, insurance provider, presence of comorbidities, and income quartile, determined according to the ZIP code where the patient lived (1 = lowest income quartile). Surgical variables included total charges, concomitant subacromial decompression or distal clavicle excision, and postoperative admission to the hospital. The total charges (in 2014 US$) represent the amount billed by the surgical center before any surgeon or professional fees. CPT code 29826 was used to identify subacromial decompression, and CPT code 29824 was used for distal clavicle excision.
Statistical Analysis
Univariate analysis was performed using the chi-square test and the independent-samples t test where applicable. Facility volume and surgeon volume were divided into low- and high-volume categories to aid in statistical analysis. We used 50 cases as the cutoff for high-volume surgeons. This value of 50 cases per year has been used to define high-volume surgeons for a number of surgical procedures. 2,8,16,24 For facilities, we used 125 cases per year as a cutoff for high volume. This value put 51% of cases in the low-volume category and 49% in the high-volume category. We then performed multiple linear regression using all variables that were significant under univariate analysis. For this regression, we used total charges as the primary endpoint to develop a model of how volume influences cost. A P value of <.05 was used to determine statistical significance. Analyses were performed using SPSS Statistics (v 21.0; IBM).
Results
There were 18,616 cases available for analysis for 2014. The mean surgeon volume was 104 ± 142 cases. The minimum was 1 case, and the maximum was 632 cases. A physician who performed 50 cases in 2014 was in the 45th percentile of surgeons by caseload. For facility volume, the mean was 198 ± 221 cases. The minimum was 1 case, and the maximum was 933 cases. A facility that had 125 cases performed in 2014 was in the 51st percentile.
Surgeon Volume
Surgical Variables
There were significant differences between surgeon volume groups regarding total charges, distal clavicle excision, and postoperative admission to the hospital (Table 1). Low-volume surgeons averaged $2024 more in total charges than their high-volume counterparts (P < .001). High-volume surgeons also performed distal clavicle excision 38% of the time, compared with 29% for low-volume surgeons (P < .001). Low-volume surgeons had a 67% higher postoperative admission rate than their high-volume counterparts (P < .001).
Univariate Analysis of Surgical Variables for Surgeon and Facility Volume

Patient Characteristics
We also found significant disparities between low- and high-volume surgeons regarding patient race, insurance provider, and income quartile (Table 2). The proportion of Hispanic patients was 49% higher for low-volume surgeons than for high-volume surgeons (P < .001). Low-volume surgeons also had a 14% greater proportion of patients with Medicare or Medicaid (P < .001) and 15% more patients living in ZIP codes with a low income, defined as being in the lower 2 income quartiles (P < .001). There was no significant difference between low- and high-volume surgeons regarding patient age, sex, and presence of comorbidities.
Univariate Analysis of Patient Characteristics for Surgeon and Facility Volume

Facility Volume
Surgical Variables
We found disparities between low- and high-volume facilities regarding total charges, distal clavicle excision, postoperative admission to the hospital, and subacromial decompression. Low-volume facilities generated higher costs, with $6453 more in total charges, on average, than high-volume facilities (P < .001). There were also 9.5% fewer distal clavicle excisions performed at low-volume facilities (P < .001). However, low-volume facilities did have 1.9% more subacromial decompressions performed than high-volume facilities (P < .001). Finally, low-volume facilities had a 104% higher postoperative admission rate than high-volume facilities (P < .001).
Patient Characteristics
There were also significant disparities between low- and high-volume facilities regarding patient race, insurance provider, and income quartile, as well as patient sex and presence of comorbidities. Low-volume facilities had a 17% greater proportion of Hispanic patients and an 18% greater proportion of black patients than high-volume facilities (both P < .001). These facilities also had a 14% greater proportion of patients with federally subsidized insurance and a 14% greater proportion of patients living in low-income ZIP codes (both P < .001). Additionally, low-volume facilities had 6.3% more female patients and 7.4% more patients with at least 1 medical comorbidity compared with high-volume facilities (both P < .001).
Multiple Linear Regression
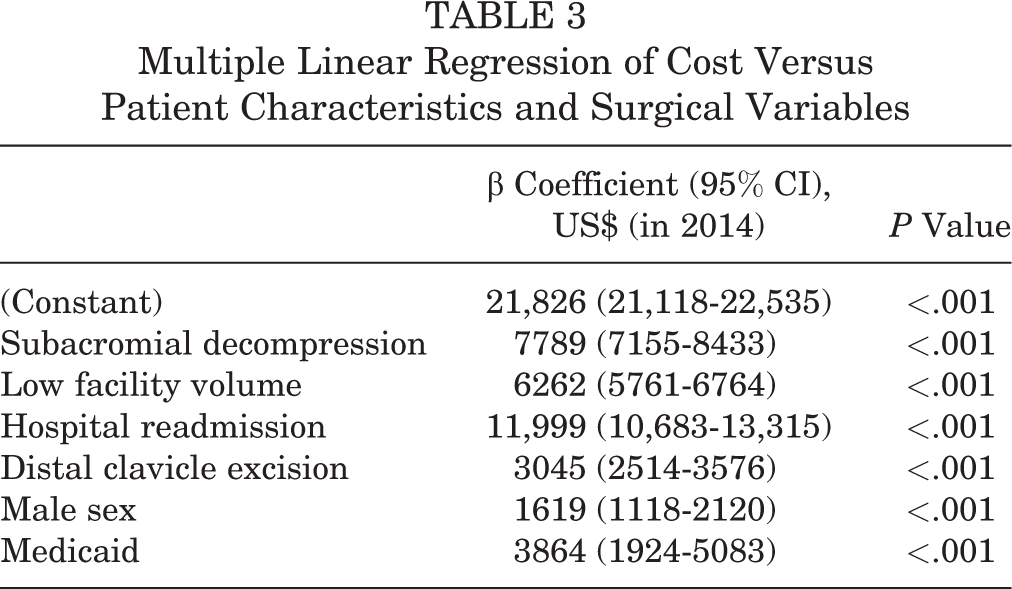
Our multivariate analysis identified several patient- and surgeon-specific factors that influenced cost (Table 3). The largest of these was postoperative admission, adding $11,999 (P < .001). Subacromial decompression added $7789 (P < .001), and distal clavicle excision added $3045 (P < .001). Male sex increased costs by $1619 (P < .001), whereas Medicaid insurance added $3864 (P < .001). Finally, facility volume was a significant determinant of the cost of RCR. Undergoing surgery at a low-volume facility increased costs by $6262 (P < .001).
Multiple Linear Regression of Cost Versus Patient Characteristics and Surgical Variables
Discussion
This study found disparities between volume groups for a number of patient and surgical characteristics in the area of study. Patients who were of lower socioeconomic status or had government-subsidized insurance received less care from high-volume surgeons and facilities. These high-volume groups provided a demonstrable economic and medical benefit to their patients, as they had lower total charges, greater rates of distal clavicle excision, and lower hospital readmission rates. We found that high-volume facilities saw more male patients, fewer patients with medical comorbidities, and fewer patients who underwent concomitant subacromial decompression. Our multiple linear regression model identified low facility volume as a significant driver of cost, even when controlling for all other variables significant under univariate analysis.
Higher physician caseload has been shown to decrease operative time and postoperative length of stay in total shoulder arthroplasty. 5 It has also been shown to decrease the risk of postoperative admission and nonroutine patient disposition upon discharge in RCR. 15 Scott et al 21 found that high-volume providers convey a substantial economic benefit over low-volume providers because of shorter admission periods and lower rates of readmission. Facility volume is also an important factor. Studies on inpatient orthopaedic procedures have shown that higher facility volume is associated with lower revision surgery rates, lower mortality rates, fewer complications, and a shorter length of stay. 9,11,19 This may be because of the surgical staff’s greater familiarity with the procedure. The disparities identified in this study are thus important to address, as they substantially affect both health and economic outcomes.
We found disparities for several patient demographics. A higher proportion of the patients for low-volume surgeons and facilities were black or Hispanic, indicating that these minority patients were less likely to receive care at high-volume centers. Similarly, a study on thyroid and parathyroid surgery found that black and Hispanic patients had longer lengths of stay and higher mortality rates in addition to having less access to high-volume surgeons. 18 It is possible that these patients are less likely to see high-volume surgeons because of differences in health insurance or geographic access to care. It is also possible that there are racial biases among surgeons, resulting in lower minority access to high-volume surgeons and facilities. More work is needed on how race affects access to eliminate these inequalities.
We also found large disparities regarding insurance and income groups. Low-volume surgeons had approximately twice the proportion of Medicaid patients as their high-volume counterparts, and low-volume facilities had over 3 times the proportion, indicating that Medicaid patients have decreased access to high-volume surgeons and facilities. It has been previously shown that Medicaid patients are 8.8 times less likely than privately insured patients to obtain an appointment with an orthopaedic surgeon for a rotator cuff tear. 20 A similar study found that only 27% of Medicaid patients were able to obtain an orthopaedic consultation compared with 91% of privately insured patients. 27 These findings may be a direct result of low reimbursement, as Medicaid reimbursement rates have been shown to be significantly lower than private insurance rates; the authors in the aforementioned study 27 estimated that private insurance reimbursed US$2125 for arthroscopic RCR, whereas Medicaid only reimbursed US$827. High-volume surgeons may therefore be incentivized to seek a higher proportion of privately insured patients. We found a similar disparity between income groups. Low-volume surgeons and facilities saw a greater proportion of patients who lived in low-income ZIP codes. In our study, 59% of patients in the highest income quartile had private insurance, whereas only 38% of patients in the lowest income quartile did (P < .001) (Table 4).
Patients With Private Insurance by Income Quartile of Patient’s ZIP Code

a Statistically significant difference compared with quartile 4.
We also found several disparities relating to surgeon-specific factors. Low-volume surgeons and facilities charged more compared with their high-volume counterparts. It is possible that high-volume surgeons have more experience with arthroscopic RCR and thus are able to complete cases in less time. Although our database did not include operative time as a variable, a previous study has indeed shown that high-volume surgeons require less time to perform arthroscopic RCR. 21
We also found a disparity in the rates of distal clavicle excision. Low-volume surgeons and facilities performed distal clavicle excision in a significantly lower proportion of cases compared with their high-volume counterparts. As with operative time, the additional experience that high-volume surgeons have with RCR may mean that they are more likely to perform concomitant procedures with RCR. For subacromial decompression, there was a disparity between facility volume groups but not between surgeon volume groups. Patients undergoing arthroscopic RCR at low-volume facilities were slightly more likely to undergo subacromial decompression concomitantly. More research is needed on concomitant procedures to understand why certain volume groups perform them at different rates and, more importantly, if patient outcomes are affected.
There was also a disparity in postoperative admission rates between volume groups, in that the rate for low-volume surgeons was 67% greater than that of high-volume surgeons. Furthermore, the postoperative admission rate at low-volume facilities was approximately double that of high-volume facilities. This is in contrast to the findings of Sherman et al, 22 who reported that hospital volume has no effect on readmission rates. Our study demonstrates that both surgeon and facility volume are important factors in the risk of postoperative admission.
To determine how surgeon and facility volume affected cost, we performed multiple linear regression with all variables significant under univariate analysis. The variable that contributed most to cost was postoperative admission to the hospital. This is likely because of the large amount of resources required for an inpatient stay. Both concomitant subacromial decompression and distal clavicle excision also significantly increased costs. These procedures have additional CPT codes that surgeons can bill for and that require additional time. Several demographic factors also increased costs in our model. Male sex added $1619. Although our database did not include information on injury severity, it is possible that men experience higher grade tears than women, which require more time in the operating room to fix. Medicaid insurance also increased the cost of arthroscopic RCR in our study.
Finally, we found that surgeon volume does not affect cost but that facility volume does. Low-volume facilities were associated with significantly higher costs, even when controlling for all other variables significant under univariate analysis. It may be that these facilities are unable to run as efficiently as their high-volume counterparts and therefore may compensate with differences in charges.
Limitations
There are several limitations to the present study. As is a risk with any claims-based database, it is possible that the Florida SASD contains misclassified elements. Because it is a state-based database, we also cannot draw broad geographic conclusions. Other states or countries may have differing delivery and payment structures, so the disparities that we found in Florida may not exist elsewhere. The SASD also does not collect information about injury characteristics, so we were unable to determine how injury severity is associated with provider or facility volume. It is possible that there is some association between injury severity and demographics. Because larger tears are more difficult and more costly to treat, this is a confounding factor in our study. Because we utilized CPT codes, there are limitations surrounding the billing of each case. Different surgeons and facilities may have differences in coding and billing practices. It is also possible that some RCR procedures were not included in our study because of coding mistakes made by a provider. The charge associated with a CPT code is only an estimate of the total cost because it often is based solely on the fee schedule for a particular contract that a surgeon has. In addition, we could not track patients through time, so we were unable to calculate the rates of revision surgery or complications other than hospital readmission. Despite these limitations, this study relied on a large sample size to minimize the effects of missing or misclassified elements. The SASD collects information on many useful patient and surgical variables, which allowed us to identify disparities in arthroscopic RCR. The utility of these databases has been well established for a number of different procedures. 1,4,7,10,12,23
Conclusion
There are disparities in access to high-volume surgeons and facilities for patients undergoing arthroscopic RCR in Florida. Patients with a lower socioeconomic status, government-subsidized insurance, and low income all faced more limited access to these high-volume groups. High-volume surgeons and facilities were associated with lower total charges, higher rates of distal clavicle excision, and lower readmission rates. Low-volume facilities added a significant amount of cost, even when controlling for all other significant variables. It is important for providers to be aware of these disparities and work to address them in their own practices.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.L.B. has received educational support from Stryker. B.D.O. is a consultant for DePuy, Linvatec, the Musculoskeletal Transplant Foundation, and Vericel and is a paid associate editor for The American Journal of Sports Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.