
Abstract
Background:
Partial articular supraspinatus tendon avulsion (PASTA) lesions are often seen in shoulders of throwing athletes. PASTA lesions in anterior instability are also found in recurrent anterior glenohumeral instability.
Purpose:
To investigate the prevalence and location of rotator cuff tears (RCTs), including PASTA lesions, in shoulders with recurrent anterior instability.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 842 shoulders in 801 patients with recurrent anterior instability (647 men, 154 women; mean age, 24 years; age range, 13-40 years) who underwent arthroscopic surgery at the age of 40 years or younger were enrolled. During surgery, the thickness and the sites of RCTs as well as patient factors associated with RCTs were examined.
Results:
RCTs were found in 57 shoulders (7%) in 56 patients. There were 4 shoulders with full-thickness RCTs and 53 shoulders with PASTA lesions. All lesions but 1 involved the anterior border of the supraspinatus (SSP). Participation in high-level athletics and older age at injury were associated with RCTs.
Conclusion:
The incidence of RCTs was 7% in shoulders with recurrent anterior instability at age 40 years or younger. Most RCTs were PASTA lesions that involved the anterior border of the SSP.
Keywords
It is well-known that partial articular supraspinatus tendon avulsion (PASTA) lesions are frequently seen in the shoulders of throwing athletes. 2,3,16,27 In our experience, PASTA lesions in anterior instability are often found in the most anterior part of the supraspinatus (SSP) and need to be repaired according to their severity, even in young patients.
An anatomic study demonstrated that the intramuscular tendon of the SSP inserts into the most anterior portion of the greater tuberosity, which corresponds to the anterior rotator cuff cable. 17 PASTA lesions in the most anterior portion of the SSP, involving the rotator cable, can cause abnormal glenohumeral kinematics 22,23 ; therefore, it is important to determine the prevalence and location of PASTA lesions in shoulders with anterior instability. Several articles, most of which are case reports, have been published concerning PASTA lesions in traumatic anterior shoulder instability in young populations. 1 –3,9 The purpose of this study was to investigate the prevalence and location of rotator cuff lesions in shoulders with recurrent anterior dislocation. We hypothesized that the site of rotator cuff lesions in patients with anterior instability would involve the anterior border of the SSP.
Methods
We received institutional review board approval prior to initiating this study and obtained written informed consent from all participating patients.
Patient Selection
Between April 2010 and August 2015, a total of 883 shoulders in 842 consecutive patients aged ≤40 years underwent arthroscopic shoulder stabilization for recurrent anterior glenohumeral instability at our institute. We excluded from the study 41 dominant shoulders in 41 throwing athletes because we aimed to examine the incidence of rotator cuff tears (RCTs) caused by anterior shoulder instability. The nondominant shoulders of throwing athletes were included. As a result, the sample for this retrospective study consisted of 842 shoulders in 801 consecutive patients, including 647 men and 154 women with a mean age of 24 years (range, 13-40 years) who underwent arthroscopic shoulder stabilization for recurrent anterior glenohumeral instability. There were 722 dominant and 120 nondominant shoulders. Of the 801 patients in the study, 584 (611 shoulders) were involved in sports with a high risk of dislocation (ie, collision/contact sports and mountain biking: 108 soccer, 106 rugby, 97 snowboard, 93 basketball, 62 judo, 37 American football, 22 handball, 13 martial arts, 10 mountain bike, 9 ice hockey, and 27 other). 4,20
Investigation of Rotator Cuff Tears
All surgeries were performed by one of the 2 senior authors (H.S., N.T.) with the patient in the beach-chair position under general anesthesia. During surgery, the thickness and site of RCTs were examined. Based on the thickness of the tear, it was classified as either a PASTA lesion or a full-thickness tear. We included only PASTA lesions with a thickness of grade 2 or higher according to the Ellman 5 classification, because grade 1 tears may have less clinical impact on shoulder function. The site of a rotator cuff lesion was classified based on the involvement of the rotator cable. We defined the anterior type as a tear in which the anterior border was located within 6 mm posterior to the long head of the biceps. The anteroposterior width of the rotator cable has been reported to be 12.5 mm, 2 and the anterior type tear included more than half of the cable. The other tears were defined as the posterior type. Rotator cuff repairs were performed for full-thickness tears and PASTA lesions with Ellman classification grade 3 depending on the individual patient's needs and background.
Assessment
Patient demographics were compared between shoulders with or without RCT: age at surgery, age at injury, sex, the number of dislocations, the rate of participation in high-risk athletics, the percentage of high-level athletes (national level or professional), the instability pattern (dislocation or subluxation), and the rate of severe glenoid bone loss (>20%). Glenoid bone loss was evaluated based on 3-dimensionally reconstructed computed tomography images (Alexion; Toshiba) showing en face views of the glenoid through use of Digital Imaging and Communications in Medicine (DICOM) viewer software (ShadeQuest/ViewC; Yokogawa Medical Solutions). 13,25 The measurements were performed in an independent and blinded manner by 2 shoulder surgeons (S.H., Y.U.) who were experienced in measuring glenoid bone loss, and the mean value of their measurements was used for the assessment.
Statistical Analysis
The chi-square test was used to compare categorical data, and the Student t test was used to compare continuous data. Logistic regression analysis was used to identify factors associated with RCTs. All statistical analyses were conducted with the use of R version 3.1.0 (R Foundation for Statistical Computing). The level of significance was set at P < .05.
Results
RCTs were found in 57 shoulders (7%) of 56 patients (41 men, 15 women) with a mean age of 27 years (range, 16-40 years): 10 judo players, 8 snowboarders, 5 rugby players, 4 soccer players, 3 mountain bikers, 2 martial artists, 1 basketball player, 1 football player, and 22 others (Table 1). There were 4 shoulders with full-thickness RCTs and 53 shoulders with PASTA lesions. Most lesions involved the anterior border of the SSP (Figure 1), with the exception of 1 lesion that was located only in the posterior cuff (Figure 2). Partial-thickness subscapularis tears were found in 5 shoulders with a mean age of 31 years (range, 20-38 years) combined with PASTA lesions. Rotator cuff repairs were performed for 21 RCTs (37%) in addition to Bankart repair (Table 1).
Demographic Data and Incidence of Rotator Cuff Lesions (N = 842 Shoulders [801 Patients]) a

a Values expressed as n (%) unless otherwise noted. PASTA, partial articular supraspinatus tendon avulsion; RCT, rotator cuff tear.

Partial articular supraspinatus tendon avulsion (PASTA) lesion (indicated by asterisk) involving the anterior border of the supraspinatus (SSP) in a shoulder with instability. HH, humeral head; LHB, long head of the biceps tendon.

Partial articular supraspinatus tendon avulsion (PASTA) lesion (indicated by asterisk) only in the posterosuperior part of the rotator cuff in a shoulder with instability. HH, humeral head.
Age at surgery (P = .03), age at injury (P < .001), and the rate of high-level athletic participation (P < .001) were significantly higher in RCT shoulders than non-RCT shoulders (Table 2). Logistic regression analysis found that high-level athletic participation (odds ratio, 3.76) and age at injury (odds ratio, 1.21) were associated with RCT (Table 2).
Comparison of Shoulders With or Without RCT a
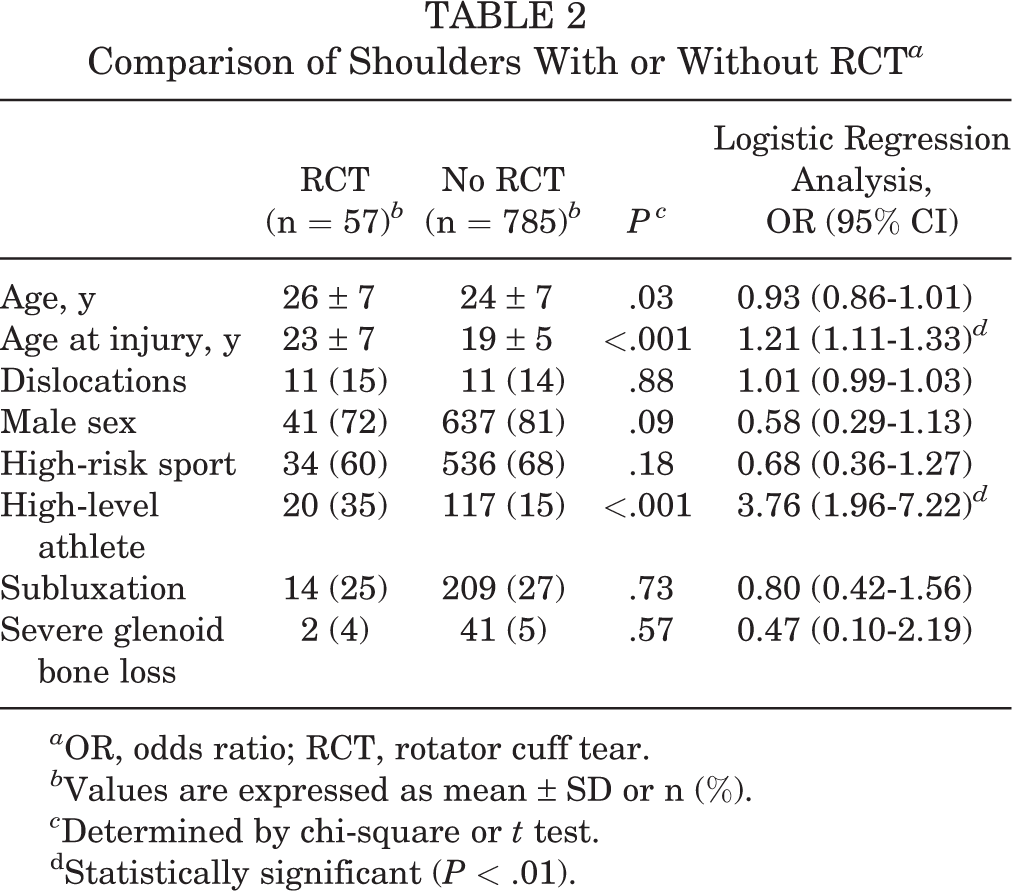
a OR, odds ratio; RCT, rotator cuff tear.
b Values are expressed as mean ± SD or n (%).
c Determined by chi-square or t test.
dStatistically significant (P < .01).
Discussion
This study revealed that the incidence of RCT was 7% in shoulders with recurrent anterior instability at the age of 40 years or younger, and most of the RCTs were PASTA lesions that involved the anterior border of the SSP. These characteristics are clearly different from those in elderly populations, where the incidence was found to be 35% to 100% and full-thickness tears were predominant. 1,8,19 The characteristics of RCTs in shoulder instability in a younger population are also different from those in throwing shoulders. The reported incidence of RCT in throwing shoulders ranged from 28% to 56%, 20 –27 and tears were located 13 to 17 mm posterior to the biceps tendon. 6,10,11,21
The relationship between RCTs and shoulder instability in a younger population remains unclear. Nakagawa et al 18 investigated RCTs in shoulders that underwent Bankart repair for shoulder instability and reported that RCTs were found in the anterior SSP in 70 of 145 (48%) shoulders, which were mostly PASTA lesions. The incidence of RCTs in the Nakagawa and Mizuno 18 study was higher than that in the current study (7%), but their study included patients between 13 and 71 years old who had Ellman grade 1 tears. The participants in our study were patients between 13 and 40 years old, and we included only grade 2 or higher PASTA lesions. These differences may be responsible for the discrepancy in results between the studies in the incidence of rotator cuff lesions.
The pathogenesis of RCTs in shoulders with anterior instability is unclear. An anterior shoulder dislocation usually occurs in shoulders with an abducted and externally rotated position. In this position, a displacement of the humeral head in the anteroinferior direction will generate a shear force to the undersurface of the anterior SSP. We assume that this force might be a cause of rotator cuff lesions in shoulders with instability. This study detected older age at injury and participation in high-level athletics as risk factors for RCTs.
High-level athletes might be more prone to receiving greater mechanical forces when their shoulder is dislocated or to developing deeper lesions by repetitive stress during sports activity. Older age might be associated with cuff degeneration; however, the mean age at injury in the current study was 23 years in patients with RCTs and 19 years in patients without RCTs. It is not clear how much impact the 4-year difference had on cuff degeneration. Further studies may be required to examine the relationship of the risk factors.
The intramuscular tendon of the SSP inserts into the most anterior portion of the greater tuberosity, 17 which corresponds to the anterior rotator cuff cable and plays an important role in shoulder stability. 12,22,26 Previous studies have reported that full-thickness RCTs destabilized the glenohumeral joint in shoulders with anterior instability and that a PASTA lesion with a thickness of more than 50% involving the rotator cable increased glenohumeral joint instability. 9,14,22,24 Given these findings, RCTs in the anterior SSP tendon should be repaired to stabilize the glenohumeral joint even in younger patients, if the depth of a tear is deeper than half of the tendon thickness. 7,12,15,22,24,26 Surgeons should pay attention to rotator cuff lesions in the anterior SSP in shoulders with anterior instability, although the incidence is not high.
This study has a few limitations. First, this was a retrospective study that entailed record review. Second, we examined only shoulders that underwent surgical treatment. This may produce a bias, but there was no other way to accurately determine the thickness and site of the RCT. Despite these limitations, this report may provide important information on the characteristics of rotator cuff lesions in younger patients with recurrent anterior dislocation.
Conclusion
This study revealed that the incidence of RCTs was 7% in the shoulders of patients aged ≤40 years with recurrent anterior instability. Most of the RCTs in shoulders with anterior instability were PASTA lesions that involved the anterior border of the SSP. Although the incidence of RCTs was not high, surgeons should bear in mind the possibility of RCT in patients with shoulder instability.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: H.S. is a paid speaker/presenter for Wright Medical, DePuy Synthes, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Funabashi Orthopaedic Hospital Institutional Review Board (ID 2014028).