
Abstract
Background:
Meniscal injury in skeletally immature patients is increasingly reported. During meniscal repair, all-inside devices may protrude beyond the posterior limits of the meniscus, putting the neurovascular structures at risk.
Purpose:
The purposes of this study were (1) to examine the relationship between the popliteal artery and the posterolateral and posteromedial aspects of the menisci, (2) to examine the relationship of the peroneal nerve to the posterolateral meniscus, and (3) to develop recommendations for avoiding neurovascular injury during posterior meniscal repair in pediatric patients.
Study Design:
Descriptive laboratory study.
Methods:
A total of 26 skeletally immature knee cadaveric specimens (7 females and 19 males) were included. Specimens were divided into age groups: 2-4, 5-8, and 9-11 years. The most posterior extent of the lateral and medial menisci was identified via sagittal and axial views on computed tomography (CT) scans. The shortest distance from the most posterior aspect of the lateral and medial menisci to the popliteal artery and the shortest distance from the posterior aspect of the lateral menisci to the anterior rim of the peroneal nerve were measured, and 3-dimensional models of representative specimens were re-created through use of CT scans.
Results:
For the age groups 2-4, 5-8, and 9-11 years, the mean minimum distance from the posterolateral meniscus to the popliteal artery was 5.2, 6.7, and 8.2 mm, respectively, and the mean minimum distance from the posteromedial meniscus to the popliteal artery was 12.7, 15.4, and 20.3 mm, respectively. In all groups, the distance between the posteromedial meniscus and the popliteal artery was greater than that between the posterolateral meniscus and the popliteal artery. The mean distance from the peroneal nerve to the lateral meniscus was 13.3, 15.0, and 17.9 mm for the respective groups.
Conclusion:
Many all-inside meniscal repair devices have sharp tips that penetrate posterior to the meniscus and capsule. This study demonstrated that the distance between the posterior meniscus and popliteal artery is relatively small in pediatric patients, especially for the lateral meniscus region.
Clinical Relevance:
Because of the higher potential for meniscal healing, meniscal repair is more likely to be performed in pediatric patients. The data in this study regarding the proximity of the lateral meniscus and neurovascular structures may be used to guide safe surgical repair of posterior meniscal tears during the use of all-inside meniscal repair devices in these patients.
The incidence of meniscal tears is increasing in skeletally immature patients, both in isolation and concomitant to anterior cruciate ligament tears 26 and tibial spine fractures. 3,11,20,29 Repair of these traumatic meniscal injuries has been reported in patients as young as 5 years, 27 and symptoms of meniscal tear are occasionally present in children younger than 8 years. Primary repair and revision meniscal repair are also frequently indicated in younger patients, 29, 31 for syndromic 2 and discoid 2,13 meniscal tears. Some studies have suggested that meniscal repairs may be more efficacious in skeletally immature patients than in older patients owing to increased blood supply and better overall healing rates in younger patients. 18,19,26,29
Previous studies in adults have examined the relationship between the popliteal artery, meniscus, and the joint line 15 as well as the potential risk factors for damaging the popliteal artery during posterior meniscal repair. 6,14 At the level of the knee joint, the popliteal artery is located between the femoral condyles and between the medial and lateral head of the gastrocnemius muscle origin. 9,33 In most cases, the artery is located just posterior to the posterior horn of the lateral meniscus at the joint line. 20,22,30 Injury to the popliteal artery is rarely reported in adults 10,11 but can lead to serious complications, including amputation. 11,23 To our knowledge, popliteal artery injury during meniscal repair surgery has not been reported in children, but the smaller distance between the meniscus and at-risk structures in children suggests that the risk of injury could be higher in this population than in adult patients.
Discoid meniscal surgery is performed in children younger than 10 years, and this includes meniscal repair. Because of the small size of these children, the need for surgery in patients with symptomatic lateral discoid meniscal abnormality, and the increasing interest in meniscal preservation and repair, it is vital to understand the anatomic parameters of these smaller patients.
Meniscal repairs, including inside-out and outside-in approaches, 12,23 allow for placement of retractors that may protect the posterior neurovascular structures. This technique is not used with all-inside meniscal repair devices. The number of devices that can be used to repair meniscal tears with all-inside arthroscopic techniques has increased given recent advancements in design and manufacturing. Many of the all-inside devices rely on hollow needle penetration of the meniscus and joint capsule. These devices may protrude well beyond the posterior limits of the meniscus during repair, thus putting the neurovascular structures at risk.
Previous studies have compared techniques, devices, and positioning in attempts to decrease the risks associated with posterior meniscal repair in adult patients. 23 Such studies have not been published for the pediatric population. Because of the increasing incidence of knee injuries in younger athletes, their smaller knee dimensions, and higher rates of meniscal healing after meniscal repair, 17,18,27,31 the anatomic details of the posterior knee are of value to surgeons performing meniscal repair procedures on small and/or skeletally immature patients. Given increases in meniscal injuries in children younger than 10 years as well as increases in the number of discoid meniscal surgeries being performed, data on the skeletally immature patient are becoming increasingly important. Great interest has arisen in meniscal preservation and revision, and the demand for data relating to this specific age group has increased. The findings of this study provide a minimal distance between the menisci and at-risk structures during a meniscal repair.
The purpose of this study was 3-fold: (1) to examine the relationship between the popliteal artery and the posterolateral and posteromedial aspects of the menisci, (2) to examine the relationship of the peroneal nerve to the posterolateral meniscus in pediatric specimens, and (3) to develop recommendations for avoiding neurovascular injury during posterior meniscal repair in pediatric patients.
Methods
This study was considered exempt from review by an institutional review board, as it was performed on donated cadaveric specimens; patients/families were not contacted and did not request any follow-up information, medical history, or genetic information. At the time of tissue donation, consent was obtained from families to use the tissue for research purposes.
A series of 26 skeletally immature knee cadaveric specimens between the ages of 2 and 11 years were examined through anatomic dissection. There were 7 female and 19 male specimens, with 14 right and 12 left knees (Table 1). The specimens were divided into 3 groups depending on the age of the donors: 2-4, 5-8, and 9-11 years. The specimens from 2- to 4-year-old donors were grouped together because, to our knowledge, surgical corrections of the menisci in this young age group have not been reported. As such, this age group was evaluated for purely anatomic, educational purposes and general developmental trajectory knowledge. The 5- to 8-year-old donors were grouped together, as they encompass the youngest ages of reported meniscal reconstructive and discoid meniscal surgery. These measurements provide a much-needed baseline for the distances between anatomic structures for surgeons performing surgery on this young age group.
Specimens by Age, Sex, and Laterality a

a F, female; L, left; M, male; R, right.
Computed tomography (CT) scans (GE LightSpeed) using 0.625-mm slices were analyzed through use of OsiriX Imaging Software (version 7.5.1). The shortest distances from the most posterior aspect of the lateral menisci to the peroneal nerve and from the lateral and medial menisci to the popliteal artery were measured at the level of the knee joint. The most posterior aspect was chosen because it is a consistent landmark that can be readily identified on the sequences. The lateral and medial menisci were identified through use of the sagittal and axial views simultaneously, to ensure that measurements were taken from the most posterior extent of the menisci. Concomitantly, the popliteal artery and peroneal nerve were identified in the axial view. Vertical and horizontal localization lines were used to verify the correct identification and localization of the posterior menisci on the axial and sagittal planes, respectively (Figures 1 and 2). The measurements were taken by 1 individual (A.B.D.), and then the point measurements on both menisci were confirmed by an orthopaedic surgeon (K.G.S.) and a musculoskeletal radiologist (A.H.).

Measurement technique. (A) Sagittal and (B) axial computed tomography images of a right knee from a 9-year-old male donor. Vertical and horizontal lines were used to confirm image slice. Measurements were taken from the most posterior extent of the medial and lateral meniscus.
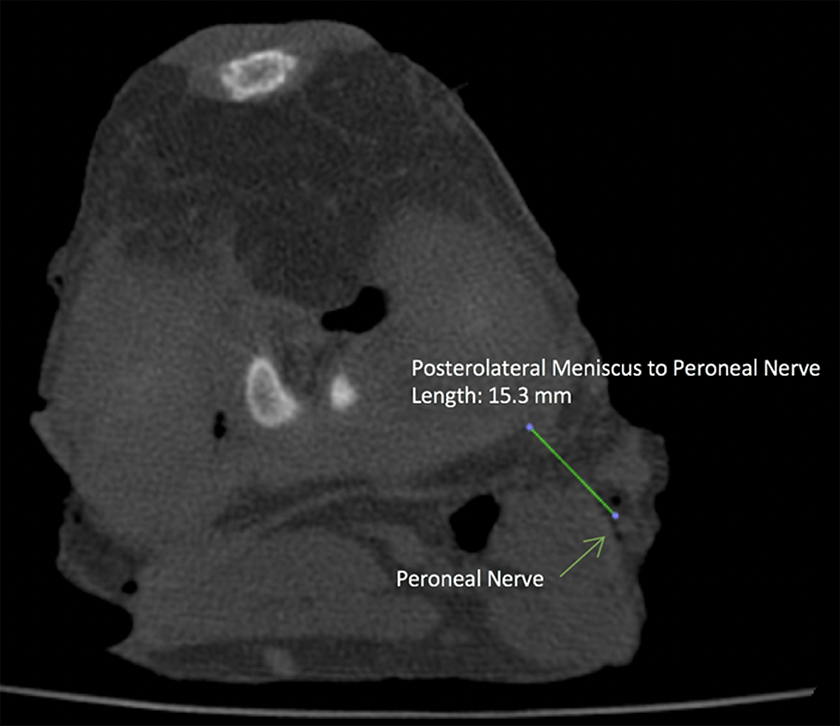
Measurement technique of a computed tomography image axial view demonstrating peroneal nerve measurement to the posterior aspect of the lateral menisci.
In addition to the measurements taken, 3-dimensional (3D) images of the meniscus, popliteal artery, and peroneal nerve were generated for 2 representative cadaveric specimens. Regions of interest were defined, outlining the menisci and neurovascular structures, which were then used to create 3D images via the 2-dimensional surface rendering feature in OsiriX and exported into Blender (version 2.75a) as stereolithography image files. These 3D models were made purely for demonstration purposes and were not used for measurement.
Results
The mean minimum distance from the posterolateral meniscus to the popliteal artery was 5.9 mm (range, 2.6-8.8 mm). Table 2 shows the mean distances for all 3 measurements by specimen age. A linear trend was observed as the distance between the posteromedial and posterolateral menisci and the popliteal artery increased with increasing patient age (Figure 3).
Distances From the Posterior Extent of the Lateral and Medial Menisci to the Popliteal Artery and Peroneal Nerve a
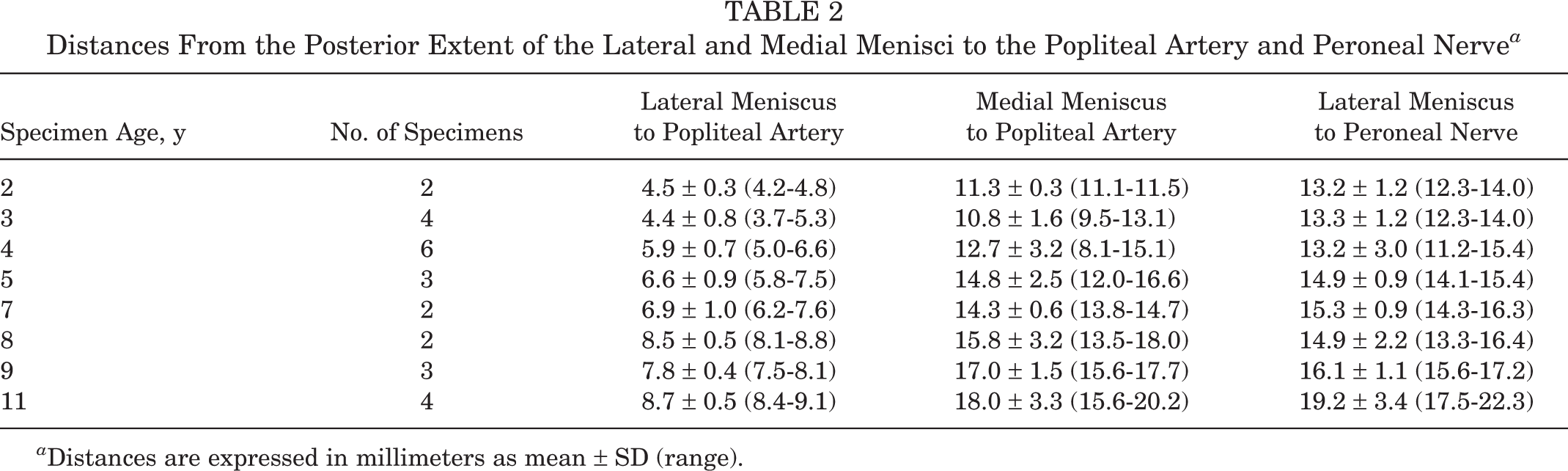
a Distances are expressed in millimeters as mean ± SD (range).

The mean distance to the popliteal artery from the lateral and medial menisci and from the peroneal nerve to the lateral menisci by age.
The mean distances for age groups 2-4, 5-8, and 9-11 from the posterolateral meniscus to the popliteal artery were 5.2, 6.7, and 8.2 mm, respectively. The mean distances from the posteromedial meniscus to the popliteal artery were 12.7, 15.4, and 20.3 mm for each age group, respectively (Table 3).
Average Distances to Popliteal Artery and Peroneal Nerve From Lateral and Medial Menisci by Age Group a

a Distances are expressed in millimeters.
The distance between the posteromedial meniscus and the popliteal artery was greater than the distance between the posterolateral meniscus and the popliteal artery (Figures 3 and 4). In addition, the distance between the posteromedial meniscus and the popliteal artery increased with age.

The mean distance to the popliteal artery from the lateral meniscus (LM) and medial meniscus (MM) and from the LM to the peroneal nerve by age range.
The mean distances from the posterolateral meniscus to the peroneal nerve were 13.3, 15.0, and 17.9 mm for each age group, respectively. This distance also increased with increasing age.
The typical relationship of the popliteal artery and posterior meniscus regions is represented by a 3D reconstruction with an axial perspective in Figure 5.
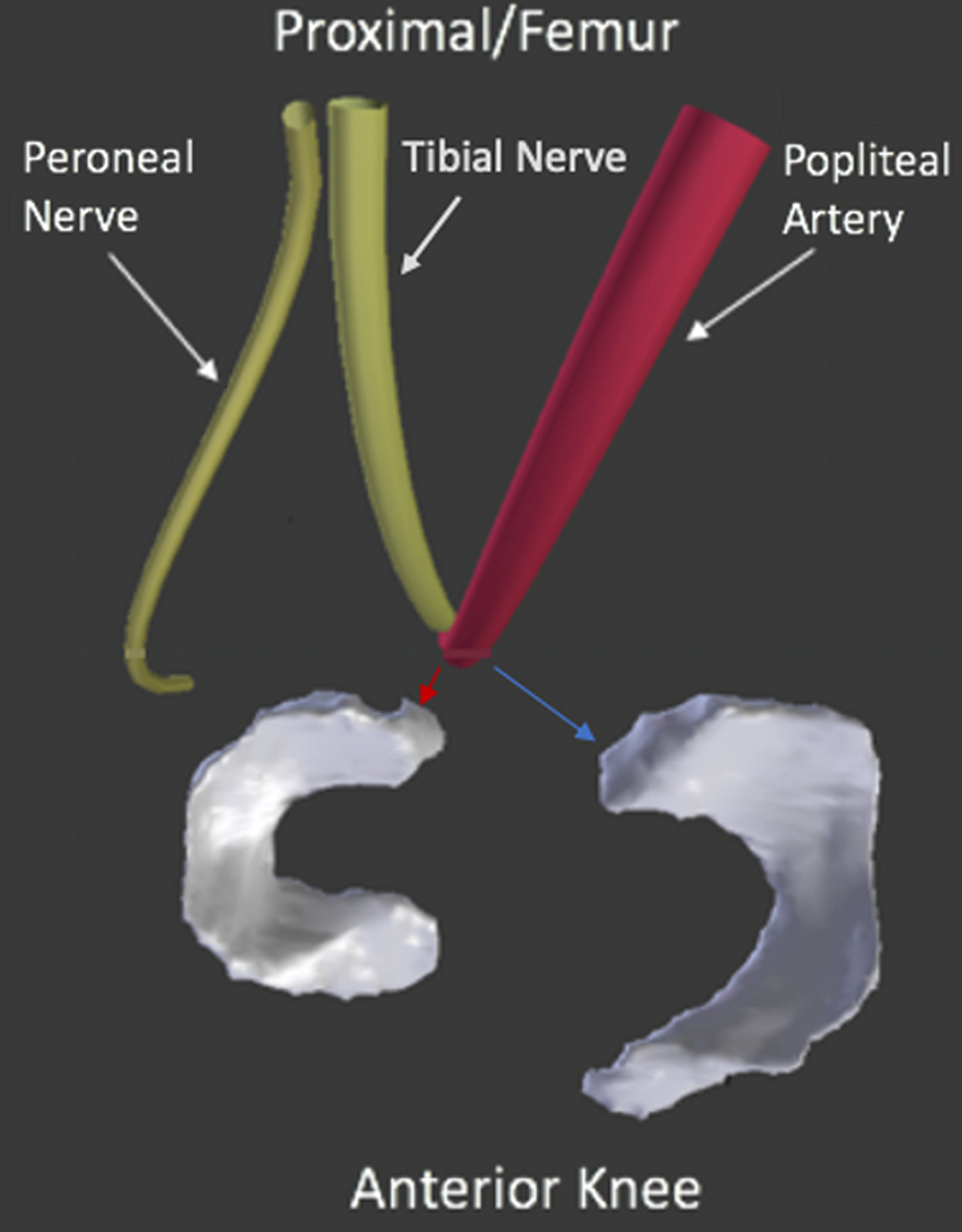
Axial view demonstrating the relationship between the popliteal artery, peroneal nerve, and posterolateral meniscus (red arrow) and posteromedial meniscus (blue arrow).
Discussion
Although meniscal tears have been considered rare in young patients, increasing rates of anterior cruciate ligament and tibial spine injury and associated meniscal injuries have increased the need for meniscal repair in pediatric patients. Many all-inside meniscal repair devices have sharp tips that penetrate several millimeters beyond the posterior meniscus and capsule, to deploy the suture and anchor. Although rare, iatrogenic neurovascular injuries have been reported in pediatric patients undergoing meniscal repairs. 5,8,16 In 2011, Camathias et al 8 reported a postoperative temporary neurapraxia of the peroneal nerve after an inside-out meniscal repair concomitant with the fixation of an osteochondritis dissecans lesion. Those authors presumed that this occurred “from stretching of the nerve during the approach to the posterior knee capsule as part of the suturing technique.”
The present study demonstrates that the distance between the posterior meniscus and popliteal artery is relatively small, especially in the lateral meniscal region. Likewise, the distance from the posterolateral menisci and the peroneal nerve is relatively small. Both distances are proportionally smaller in younger patients. The distance from the lateral meniscus to the peroneal nerve is larger but still relativity close to the meniscus to warrant caution during meniscal repair. To avoid iatrogenic neurovascular injury during placement of all-inside meniscal repair devices, surgeons should consider these distances and the close relationship of the neurovascular structures.
In our review of these data, some general recommendations about meniscal repair and avoiding the neurovascular structures have been developed. 3,4,21 Suture-based mattress repair patterns can be performed at an angle that is nearly perpendicular to the meniscal structure. In repairs of the anterior or middle regions of the meniscus, the approach angle from either the portal on the same or on the opposite side of the meniscus does not direct the advancing needles toward the neurovascular bundle (Figure 6, green arrows). The tibial spine and cruciate ligament structures may constrain the angle of approach for meniscal repair; in some cases, this constraint may require that posterior region repairs start from arthroscopic portals on the same side as the meniscal tear. This starting position may aim more centrally toward the popliteal artery, which may carry a higher risk of neurovascular injury (Figure 6A, red and orange arrows). If the repair device is aimed at the central region of the popliteal area for tears of the most posterior meniscal regions, the depth of penetration should be minimized to avoid neurovascular injury. The safe penetration zone/depth may be greater on the medial meniscus in comparison with the lateral meniscus (Figure 6B). These recommendations are most appropriate for all-inside repair devices with sharp needle tips that require significant penetration beyond the meniscal substance to engage the fixation on the joint capsule. During inside-out repairs, retractors may protect these neurovascular structures from direct injury.

(A) Representation of safer (green arrows) and less safe (orange and red) angles of approach with sharp-tipped meniscal repair devices. (B) The artery is offset laterally, positioning the artery closer to the lateral meniscus.
In the present series, the popliteal neurovascular bundle was found to be closer to the posterior region of the lateral meniscus versus the medial meniscus in all cases. Other studies have shown some variation in the popliteal artery position; Keser et al 15 demonstrated that popliteal artery localization was lateral to the central axis in 94.3% of cases but was on the central axis in 5.7%. The findings by Keser et al 15 and the current study demonstrate that the most posterior and central axial regions of both the medial and the lateral menisci are at the greatest risk of neurovascular injury during the use of all-inside repair devices with sharp needle tips.
Although traumatic meniscal tears in association with significant ligamentous knee injury can occur in young patients, symptomatic discoid meniscal tears are also seen in this patient population. 1,7,13,17,24,34 In some cases, discoid meniscal treatment may include meniscal preservation surgery 1,24 that includes trimming or contouring of the meniscus, which may be combined with suture repair. The anatomic information reported here regarding the proximity of the lateral meniscus and neurovascular structures may be of value in planning surgical repair of a discoid meniscus. This may be especially important in cases of saucerization and peripheral stabilization of the meniscal rim to the capsule, owing to the proximity of the popliteal artery and peroneal nerve. 3,25,32
The finding in the present study of a linear growth pattern of increasing distance between neurovascular structures and the lateral menisci is in line with findings from study conducted on adult specimens. 25 The average distance from the lateral meniscus to the popliteal artery in our specimens by increasing age group was 5.2, 6.7, and 8.2 mm compared with the adult measurement of 10.1 mm reported by Sanz-Perez et al. 25 Likewise, our linear increase of distance with increasing age was in line with their mean distance from the lateral menisci to the peroneal nerve: Sanz-Perez et al 25 reported a distance of 17.4 mm, whereas our measurements increased with age: 13.3, 15.0, and 17.9 mm for age groups 2-4, 5-8, and 9-11 years, respectively.
The present study has several limitations. Because the cadaveric specimens were stored in full extension and had become frozen in this position, the specimens were imaged at or close to full extension, as bending the frozen tissue, even after thawing, could introduce some artifact. Full knee extension may bring the neurovascular structures more anterior and decrease the space between the meniscus and at-risk structures. Knee position may also influence the interval between the popliteal artery and the posterior meniscus regions. Nishimura et al 23 demonstrated in adult participants that with the knee in flexion and in the figure-of-4 position, the distance from the artery and the posterior aspect of the lateral meniscus is much greater. Some conflicting results have come from in vivo studies, with some studies showing that the artery may, in fact, move closer to the tibial surface in flexion. 28,35 Regardless, the measurements in the present study may represent the minimal distance in extension, and it is possible that these measurements could increase in flexion.
Another limitation is the use of CT scans as opposed to magnetic resonance imaging (MRI) scans. MRIs have the distinct advantage of relatively clear delineation of soft tissue structures, including the meniscus, artery, and nerve. However, MRI is limited to slice thickness of 3.0 to 4.0 mm, whereas the CT scans allow for 0.625-mm slice thickness. CT scans offer better delineation of osseous structures and less clear tissue distinction for soft tissues. In this series, the planes of the menisci, nerve, and arteries were relatively easy to delineate on the CT scans. The specimens had all skin and subcutaneous tissue removed, which allowed for air penetration into the tissues. This air penetration enhanced the contrast between tissue planes and made delineation clearer in some cases.
Conclusion
Meniscal repairs secondary to trauma and discoid meniscus are increasingly common in young, skeletally immature patients. The design of some all-inside repair devices requires sharp needle tip penetration posterior to the meniscal tissue to the level of the capsule, which has the potential to cause direct neurovascular injury. The measurement data reported here clarify the relationship between the posterior meniscus and associated neurovascular structures in young patients and may be used to guide safe surgical repair of posterior meniscal tears.
Footnotes
Acknowledgment
The authors acknowledge Todd Huft, Lisa Houck, and Tom Cycotoa, CEO, of Allosource (Centennial, Colorado). Their generous donation of these specimens and use of their facilities allowed for this study. Andrew Hill, MD (musculoskeletal radiology), provided recommendations for best imaging practices for this study. The authors also honor and acknowledge the families who made the gifts of donation to the study group. Their donations have made this research possible and will contribute to the lives of other families and their children.
One or more of the authors has declared the following potential conflict of interest or source of funding: AlloSource provided the cadaveric specimens used in this study. K.G.S. has received nonconsulting fees from DePuy (contested by the author) and has received research support from Sanofi-Aventis (contested by the author). Y.-M.Y. has received educational support from Kairos Surgical and hospitality payments from Smith & Nephew. T.J.G. has received educational support from Arthrex and Liberty Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.