
Abstract
Background:
Repair of the posterior horn of the lateral meniscus using an all-inside meniscal repair device involves the risk of iatrogenic posterior neurovascular injuries. Previous studies that have evaluated this risk were based on preoperative magnetic resonance imaging (MRI) with the knee in 30° of flexion and used landmarks that are impractical in the actual operative situation.
Purpose:
To use an MRI model simulating actual knee arthroscopic conditions to (1) compare the potential risk of injuries related to the lateral border of the posterior lateral meniscus root (LMR) through the anterolateral versus anteromedial portal and (2) establish “safe” and “danger” zones to reduce the possibility of injuries to posterior neurovascular structures when performing lateral meniscal repair in relation to the lateral border of the posterior LMR.
Study Design:
Descriptive laboratory study.
Methods:
Using 29 axial MRI scans of knees in the figure-of-4 position with joint fluid dilatation at the level of the lateral meniscus, direct lines were drawn to simulate a straight all-inside meniscal repair device deployed from the anterolateral and anteromedial portals to the lateral border of the posterior LMR, extending 14 mm beyond the joint capsule. If the line passed through or touched a posterior neurovascular structure, a risk of iatrogenic injuries was noted, and measurements were made to determine the safe zone in relation to the lateral border of the posterior LMR.
Results:
Repairing the lateral meniscus through the anterolateral portal in relation to the lateral border of the posterior LMR resulted in a significantly greater risk of posterior neurovascular injuries compared with repairing through the anteromedial portal, with injury incidences of 68.97% and 10.35%, respectively (P = .001). The safe zones of lateral meniscal repair through the anterolateral and anteromedial portals were 4.15 ± 1.87 and 6.57 ± 0.98 mm, respectively, beyond the lateral border of the posterior LMR.
Conclusion:
The risk of posterior neurovascular injuries when repairing posterior lateral meniscal tissue was found to be significantly greater through the anterolateral portal compared with the anteromedial portal.
Clinical Relevance:
Surgeons can use the safe zones as defined in this study to decrease the risk of iatrogenic posterior neurovascular injuries during arthroscopic lateral meniscal repair.
An injury to the posterior horn of the lateral meniscus can occur either alone or combined with an acute anterior cruciate ligament injury, and the recommended treatment approach is meniscal repair. The most common repair method is all-inside meniscal repair, which may lead to iatrogenic posterior neurovascular injuries (popliteal artery, tibial nerve, or popliteal vein) because the neurovascular bundle containing these structures is located in the posterolateral area of the knee joint and close to the posterior capsule.7,8,12 Various studies have reported an incidence of iatrogenic popliteal injuries in arthroscopic knee surgery of up to 0.03%, including pseudoaneurysm, severe limb ischemia, and extensive bleeding.1,4,5,9,13,14
The main type of injury during this procedure is accidental penetration of a posterior neurovascular structure by the needle tip of an all-inside meniscal repair device, and various studies have identified “safe” and “danger” zones during the meniscal repair procedure. However, these studies have generally consisted of 2 types, cadaveric10,11 or magnetic resonance imaging (MRI),2,3,6 and both types had some notable limitations. All of the cadaveric studies evaluated the risk of iatrogenic posterior neurovascular injuries using midthigh to midleg knee sections, which had no natural tension in soft tissue or neurovascular structures. In addition, most of the MRI studies were based on preoperative MRI with the knee in a slightly flexed position with no joint fluid dilatation and no varus force on the knee joint, which is quite different from the standard arthroscopic figure-of-4 position with joint fluid dilatation and varus force on the knee joint. There has been only 1 study2 that evaluated safe and danger zones for avoiding posterior neurovascular injuries based on the real-life arthroscopic situation using the reference landmark of the medial edge of the popliteus tendon, but this landmark is quite distant from the posterior horn of the lateral meniscus and posterior neurovascular structures. Thus, the measurements in that study may not reflect actual operative distances, and there is uncertainty when applying the findings of that study during actual arthroscopic surgery.
The objective of this study was to evaluate the risk of injuries related to the lateral border of the posterior lateral meniscus root (LMR) through the anterolateral and anteromedial portals and establish safe and danger zones to reduce the possibility of injuries to posterior neurovascular structures when performing lateral meniscal repair in relation to the lateral border of the posterior LMR, using an MRI model simulating actual knee arthroscopic conditions.
Methods
This study used a prospective design, and the study protocol received institutional review board approval. All participants provided informed consent. It initially involved 79 patients who had been scheduled for arthroscopic knee surgery to treat an intra-articular abnormality between January 1, 2018, and December 31, 2020. Of the 79 patients, 50 were excluded because of associated medial and/or lateral collateral ligament injuries, meniscal and/or cartilage injuries, or a history of open or arthroscopic knee surgery. After each operative procedure, the joint fluid pressure of the knee was maintained at 50 mm Hg using an arthroscopic pump system, and the patient immediately underwent MRI with the knee in the figure-of-4 position with varus force and joint fluid dilatation.
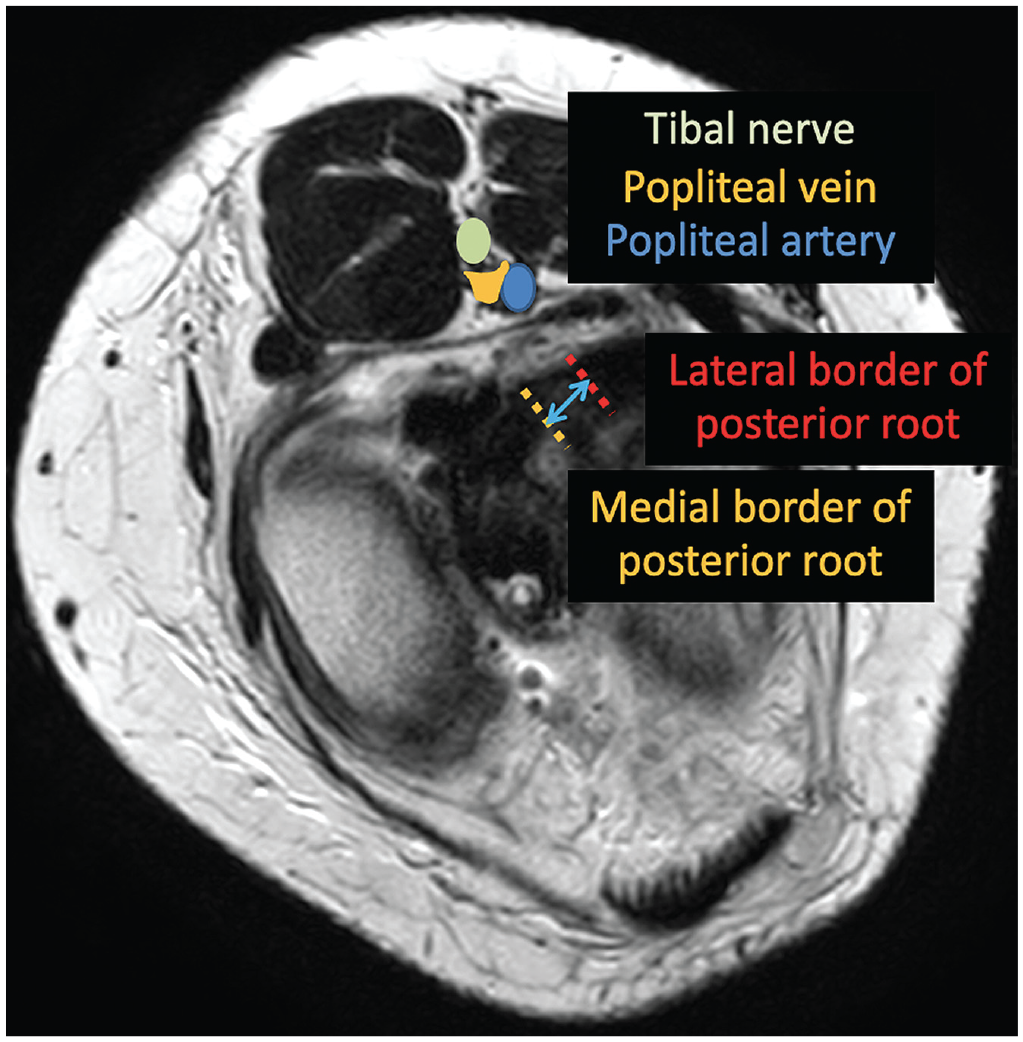
MRI scans in the axial, coronal, and sagittal views were obtained with the knee in the figure-of-4 position with varus force, simulating the actual operative position; then, an MRI scan in the axial oblique view was obtained in alignment with the tibial plateau. The imaging slides that best demonstrated the posterior root of the lateral meniscus were used as the reference images for the study measurements. The medial and lateral borders of the posterior LMR were identified from coronal MRI scans (Figure 1). The width of the posterior root where it attached to the tibia was measured on the coronal image and used for reference as the distance between the medial and lateral borders of the posterior LMR on the axial image. The most central portion of the medial border of the posterior LMR was used and measured laterally according to the posterior root width using the axial oblique image (Figure 2).

Coronal magnetic resonance imaging (MRI) was used to identify the medial and lateral borders of the posterior lateral meniscus root (LMR) (outlined in red). The width of the posterior root where it attached to the tibia (arrows) was measured and used for reference as the distance between the medial and lateral borders of the posterior LMR on axial MRI.
Axial oblique magnetic resonance imaging showing the most central portion of the medial border of the posterior lateral meniscus root was used for lateral measurements according to the posterior root width.
In the current study, we simulated a straight all-inside meniscal repair device by drawing a direct line through both the anterolateral and anteromedial portals, using the lateral and medial edges, respectively, of the patellar tendon as landmarks. A straight line (Figure 3A, blue line) was drawn from the anterolateral portal, passing the lateral border of the posterior LMR and joint capsule to a posterior neurovascular structure extending 14 mm beyond the joint capsule. The closest distance (Figure 3A, red line) was perpendicularly measured from this line to the lateral border of the posterior neurovascular structure. If this line passed through the posterior neurovascular structure, a second straight line (Figure 3B, green line) was drawn from the anterolateral portal to the lateral border of the posterior neurovascular structure, and the distance between these 2 straight lines (Figure 3B, purple line) was measured at the level of the lateral border of the posterior LMR. The measurements from the anteromedial portal to the posterior neurovascular structure were performed following the same procedure as for the anterolateral portal.

Drawings of axial views of the knee showing measurements from the anterolateral portal to the lateral border of the posterior lateral meniscus root (LMR). (A) First, a direct line (blue line) was drawn from the anterolateral portal to the lateral border of the posterior LMR, extending 14 mm beyond the joint capsule. The closest distance (red line) was measured from the direct line (blue line) to the posterior neurovascular structure. (B) A risk of iatrogenic posterior neurovascular injuries was noted if the direct line (blue line) passed through the posterior neurovascular structure. If there was a noted risk of posterior neurovascular injuries from the direct line (blue line), and a second direct line (green line) was drawn from the anterolateral portal to the lateral border of the posterior neurovascular structure. The danger zone for meniscal repair (purple line) was defined as the area between the first direct line (blue line) and the second direct line (green line), and the safe zone was defined as the area beyond the danger zone at the level of the lateral border of the posterior LMR.
All distances were measured 3 times by an experienced musculoskeletal radiologist. Intraobserver reliability was assessed using the intraclass correlation coefficient, with a period of 2 weeks between measurements.
The results are shown as descriptive statistics (means ± standard deviations) and incidence rate ratios. Statistical analysis was performed with the R program and epicalc package (Version 3.4.3; R Foundation for Statistical Computing). The statistical significance of the noted risk of iatrogenic posterior neurovascular injuries was assessed using the chi-square test of independence and associations, with P < .05 considered to be the threshold for statistical significance.
Results
Overall, 29 axial MRI scans from 26 men and 3 women were reviewed in this study. The mean age of the patients was 31.4 ± 10.7 years. The arthroscopic procedures that these patients underwent consisted of loose body removal or anterior cruciate ligament reconstruction.
Repairing the posterior horn of the lateral meniscus through the anterolateral portal was found to be significantly more dangerous than repairing through the anteromedial portal in relation to the lateral border of the posterior LMR, with injury incidences of 68.97% and 10.35%, respectively (P = .001). The safe zones when repairing through the anterolateral and anteromedial portals were 4.15 ± 1.87 mm (maximum distance, 7.23 mm) and 6.57 ± 0.98 mm (maximum distance, 7.58 mm), respectively, beyond the lateral border of the posterior LMR.
The intraclass correlation coefficient of all MRI measurements ranged from 0.884 to 1.000, indicating high intraobserver reliability.
Discussion
In this study, we compared the risk of iatrogenic posterior neurovascular injuries when performing all-inside meniscal repair through the anteromedial and anterolateral portals in relation to the lateral border of the posterior LMR. Repairing through the anterolateral portal was significantly more dangerous than through the anteromedial portal. The safe zones of repair through the anterolateral and anteromedial portals were 7.23 and 7.58 mm, respectively, beyond the lateral border of the posterior LMR. To our knowledge, there have been no previous studies evaluating the risk of posterior neurovascular injuries related to the lateral border of the posterior LMR based on the actual arthroscopic situation in which the posterior LMR is easy to identify intraoperatively. The results of our study can be applied to actual arthroscopic conditions to evaluate the risk of injuries.
Posterior neurovascular structures are located at the midlateral aspect of the posterior knee compartment and close to the posterior capsule, which may lead to a risk of iatrogenic posterior neurovascular injuries when repairing posterior lateral meniscal tissue. There have been only a few studies that evaluated and compared the risk of posterior neurovascular injuries between repair through the anteromedial portal and repair through the anterolateral portal using an all-inside meniscal repair device. Massey et al 11 and Mao et al 10 used the landmarks of the medial and/or lateral borders of the posterior meniscus root, and both of these studies found that repairing through the anteromedial portal was safer than repairing through the anterolateral portal. However, these studies used cadaveric knees dissected midthigh to midleg in a 90° flexed position, which is different from the real-life arthroscopic situation and thus makes their findings questionable because there was no soft tissue or neurovascular tension and the normal operative position is the figure-of-4 position with attendant varus force.
In an earlier MRI-based study, Gilat et al 6 used preoperative MRIS with the knees in a slightly flexed position to evaluate the risk of iatrogenic popliteal artery injuries. They found that there was a risk of iatrogenic popliteal artery injuries in repairing meniscal tissue through both the anteromedial and anterolateral portals using a simulated straight all-inside meniscal repair device related to the posterior cruciate ligament. However, in the actual operative situation, the posterior cruciate ligament is covered with synovial tissue and cannot be easily seen during arthroscopic surgery; thus, applying their results is impractical during actual surgery. In a study published in 2021, 3 our author group evaluated the risk of posterior neurovascular injuries related to the medial border of the popliteus tendon using preoperative MRIS with the knees in a slightly flexed position and found that there was a risk of injuries when repairing posterior meniscal tissue 19.01 ± 4.67 mm beyond the medial border of the popliteus tendon through the anteromedial portal and 16.53 ± 4.30 mm beyond the medial border of the popliteus tendon through the anterolateral portal. In another study, 2 1 year later, we used MRIS with the knees in the standard arthroscopic position to evaluate the safe and danger zones of repairing lateral meniscal tissue and found that the danger zone was 15.84 ± 4.52 mm beyond the medial border of the popliteus tendon through the anteromedial portal and 9.62 ± 4.60 mm beyond the medial border of the popliteus tendon through the anterolateral portal. However, even though that study 2 evaluated the risk of injuries based on the real-life arthroscopic situation, there was 1 important point of concern: the reference landmark was the medial border of the popliteus tendon, which is quite distant from the posterior meniscus root, leading to a chance of error when applying the results to the actual operative situation. To decrease this potential risk in the current study, we used the landmark of the lateral border of the posterior LMR to determine the risk of injuries as well as define the safe and danger zones, which are easier to identify and closer to the posterior lateral meniscal tissue than the landmark of the medial border of the popliteus tendon. We found that the safe zones for avoiding iatrogenic posterior neurovascular injuries during repair through the anterolateral and anteromedial portals were 7.23 and 7.58 mm, respectively, beyond the lateral border of the posterior LMR. To avoid this type of injury, the surgeon can use these results during arthroscopic meniscal repair.
Limitations
Our study had some limitations. First, the popliteus tendon passes the knee joint in an oblique direction, which can affect the measurements. This potential problem was minimized by using axial MRI slices that passed through the center of the lateral meniscus. Second, we assessed the risk of injuries and the safe and danger zones based on a simulated straight meniscal repair device, but the surgeon can use straight, curved, and/or reverse-curve repair devices, which may result in different measurements; thus, the surgeon should be careful when using our results in repairing with curved or reverse-curve devices. Third, the anteromedial and anterolateral portals were simulated at the medial and lateral borders, respectively, of the patellar tendon, and the surgeon should be careful when using our results for portals created utilizing different landmarks. Fourth, the femoral condyle and tibial spine may be obstructed when repairing through the anteromedial portal, and thus, repairs in this situation may be difficult. Fifth, we did not evaluate the effect of different patient heights or knees with different dimensions on either the incidence of iatrogenic posterior neurovascular injuries or the location of safe and danger zones.
Conclusion
There was a risk of injuries with repair of posterior lateral meniscal tissue through either the anterolateral or anteromedial portal in relation to the lateral border of the posterior LMR, with repair through the anterolateral portal having a greater simulated risk than repair through the anteromedial portal, but the surgeon can use the safe zones as defined in this study to decrease the risk of iatrogenic posterior neurovascular injuries during arthroscopic lateral meniscal repair.
Footnotes
Acknowledgements
The authors sincerely thank Dr Boonsin Tangtrakulwanich of the Department of Orthopedics, Faculty of Medicine, Prince of Songkla University; Jirawan Jayuphan of the Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, for providing statistical support; and Dave Patterson for providing editing support.
Final revision submitted May 10, 2023; accepted May 22, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Faculty of Medicine of Prince of Songkla University (No. REC 60-180-11-1 and REC 65-378-11-1).