
Abstract
Background:
It is estimated that 28% of patients are dissatisfied after anterior cruciate ligament (ACL) reconstruction, in part because they do not understand the procedure well enough.
Purpose:
To assess the postoperative comprehension, satisfaction, and functional outcomes of 2 patient groups: 1 undergoing a standard surgical procedure (standard group) and 1 involved in their surgery (participation group).
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Over a 4-month period, 62 patients were included: 31 in the standard group and 31 in the participation group. The preoperative information, surgical technique, anesthesia, and postoperative course were identical in both groups. Patients in the participation group were allowed to watch the arthroscopic portion of their surgery live on a video screen, and standardized information was given to these patients during the arthroscopic phase. Self-administered questionnaires were given to assess comprehension (Matava score), satisfaction (visual analog scale [VAS] for satisfaction, Net Promoter Score [NPS], and Evaluation du Vécu de l’Anesthésie LocoRégionale [EVAN-LR]), and outcomes (International Knee Documentation Committee [IKDC] form and Anterior Cruciate Ligament–Return to Sport after Injury [ACL-RSI] scale) between groups.
Results:
Postoperative comprehension was significantly improved in the participation group, as the Matava score increased by a mean of 7.1 ± 5.3 points versus 2.7 ± 5.6 points in the standard group (P = .0024). The mean VAS satisfaction score immediately after surgery was 9.8 ± 0.6 in the participation group versus 8.9 ± 1.9 in the standard group (P = .0033); this difference was still present at 1 year postoperatively (9.8 ± 0.6 vs 9.1 ± 1.7, respectively; P = .0145). The NPS was 96.8% in the participation group versus 64.5% in the standard group (P = .0057) in the immediate postoperative period and 100.0% in the participation group versus 71.0% in the standard group at 1 year postoperatively (P = .0046). The mean total EVAN-LR score was 89.1 ± 6.5 in the participation group and 84.6 ± 9.9 in the standard group (P = .0416). At 1 year postoperatively, the mean IKDC score was 86.0 ± 7.5 in the participation group versus 80.0 ± 7.4 in the standard group (P = .0023). The mean ACL-RSI score was 80.9 ± 7.7 in the participation group versus 74.3 ± 8.4 in the standard group (P = .0019).
Conclusion:
Involving patients in their ACL reconstruction surgery improves their understanding of the procedure and their satisfaction with their care, which results in better outcomes at 1 year postoperatively.
The anterior cruciate ligament (ACL) is a major contributor to knee stability and function. It prevents the tibia from sliding too far forward relative to the femur and from rotating too much internally. It is also one of the most frequently injured knee ligaments, with well-known consequences: instability contributes to osteoarthritis development in 50% of patients 10 to 20 years after the injury. 22
Arthroscopic ACL reconstruction is a common orthopaedic surgery procedure. It is intended for active patients who want to resume a high activity level. 26 While the outcomes are highly satisfactory in terms of returning to sports and recovering full function, 28% of patients are dissatisfied with this surgery in terms of their knee function. 1 It has been suggested that psychological factors related to how patients perceive their knee function have a large impact. For example, the fear of reinjuring their knee or a lack of confidence in the function of the repaired knee prevents patients from attaining their goals (such as returning to preinjury levels) and leads to dissatisfaction. 1 This high rate of patient dissatisfaction can partly be attributed to the gap between functional outcomes and patient expectations. 23 This brings into question whether patients truly understand the fine points of the surgical procedure (ie, modalities of surgery, postoperative convalescence period, duration of rehabilitation) 1 because the most dissatisfied patients are the ones who did not understand what their postoperative abilities and limitations would be.
Satisfaction is a multifactorial phenomenon determined by elements beyond mere physical function. 28 Better understanding of the diagnostic processes and goals of surgery, which can be achieved through a better information method, improves satisfaction-related outcomes. 28 This has been observed when an information video is provided to patients before ACL surgery 32 and other types of surgery. 39
Appropriate information given by the physician plays a key role in patient satisfaction and comprehension. 12,18 This is especially true in an era in which patients are increasingly well informed through their own research. For example, studies have shown that although the choice of graft is primarily influenced by the surgeon’s recommendations, the patient’s own research (especially on health-related websites) comes into play. 8
Newer regional anesthesia methods allow patients to be fully conscious during the entire surgical procedure. 9,16 Also, because knee arthroscopic surgery involves a camera and video screen, a patient could theoretically see what is happening during the arthroscopic portion of the surgical procedure in real time and receive information about the various steps. This allows the patient to participate and be engaged in the surgical procedure. Participation consists of looking at the arthroscopic screen during surgery while providing the patient with standardized information. We found no published studies evaluating the comprehension and satisfaction of patients who were involved in their ACL reconstruction surgery in such a manner.
We hypothesized that allowing patients to participate in their own surgery would lead to better understanding of the procedure and ultimately greater satisfaction and better functional outcomes. The goal of this study was to assess patient comprehension, satisfaction, and outcomes based on patient participation in the surgical procedure.
Methods
This was a prospective, single-center, nonrandomized, sequential pilot study. Our hospital’s research ethics committee approved this study.
Patients
Between December 2016 and March 2017, a total of 101 patients underwent ACL reconstruction at our hospital. To be included in our study, patients had to be at least 18 years of age, have an isolated ACL injury in 1 knee, undergo arthroscopic reconstruction, and speak and understand French. Patients were excluded if they were undergoing additional procedures, had a meniscal injury requiring resection or suture repair, declined to participate in the study, received a type of anesthesia in which the patient was unconscious, were under guardianship or were a ward of the court, did not have at least 1 year of follow-up, or were pregnant or breastfeeding.
This resulted in 62 patients being included in the study: 31 in the standard group and 31 in the participation group (Figure 1). Patients were enrolled consecutively: the standard group from December 2016 to January 2017 and the participation group from January 2017 to March 2017. In the standard group, patients underwent surgery in the usual manner, without looking at the arthroscopic video screen during the procedure. In the participation group, patients were allowed to look at the arthroscopic video screen during their surgery and received standardized information about the management of the procedure. Patients in both groups received the same preoperative information, which was provided by a single surgeon in a standardized manner. The 2 groups received the same type of anesthesia (spinal with no sedation), underwent surgery using the same reconstruction technique by the same surgeon (E.C.), and underwent the same rehabilitation protocol. The only difference between the 2 groups was whether the patient participated in the surgical procedure while having access to the arthroscopic screen and standardized information.
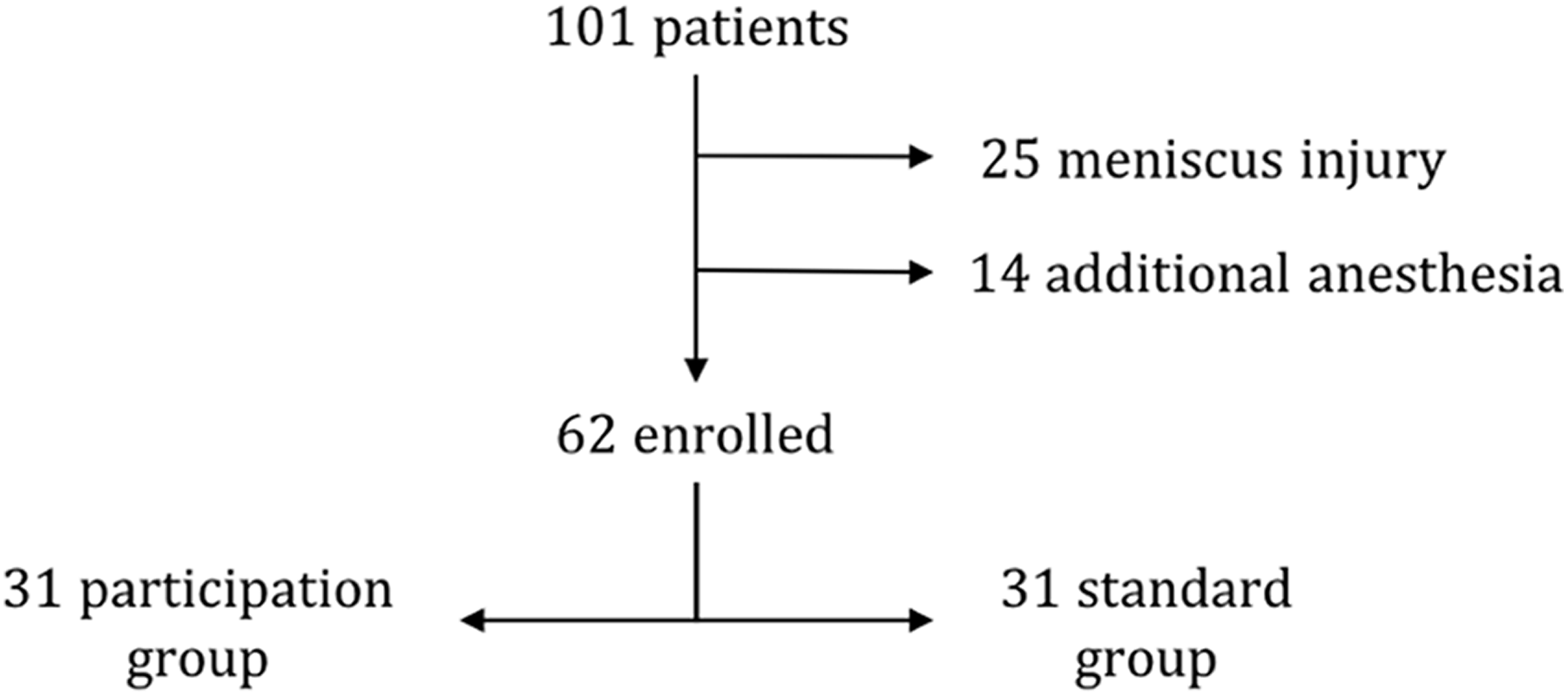
Study flowchart.
Surgical Technique
Patients in the standard group underwent ACL reconstruction using a quadriceps tendon graft, 5 as described below. An inside-out femoral tunnel was drilled with the same diameter as the graft through an anteromedial portal using Arthrex instrumentation. The tibial tunnel was created using a 55° instrument and then drilled with a cannulated reamer. The femoral end and then the tibial end of the graft were secured using a 23 mm–long BioComposite Interference Screw (Arthrex). The bone block was fixed inside the tibial tunnel.
Patients in the participation group underwent the same surgical treatment as patients in the standard group. The only difference was that the former group was allowed to look at the arthroscopic video screen to follow their surgery in real time during the arthroscopic phase (Figure 2). All patients in the participation group also received standardized information during the actual arthroscopic procedure.

Arthroscopic video screen is visible to the patient who is conscious and aware.
Perioperative Information
The patients in both groups were given the same information sheet and the same diagram preoperatively that explained the surgical procedure. All patients in the participation group received additional information during surgery. This information was standardized, identical for all patients, and always delivered in the same order: Knee anatomy: the surgeon showed the patient the joint surfaces of the femur and tibia, the medial and lateral menisci, and the ACL and posterior cruciate ligament. Injured ACL: the surgeon showed the patient his/her torn ACL. Tunnel preparation: the surgeon showed the patient the location of the tibial and femoral bone tunnels, and the tunnels were then drilled. Ligament reconstruction: the surgeon showed the patient the “new” ACL and used a hook to demonstrate tension on the structure.
If patients had questions, they could ask the surgeon, who would answer using the arthroscopic screen as needed. If patients in the standard group had questions, they could ask them during surgery. These patients received spinal anesthesia but could not see the arthroscopic screen; in the end, none of them asked questions during surgery.
Anesthesia
The anesthesia protocol required that the patient be conscious and aware to receive and understand the intraoperative information. Hence, all patients received appropriate spinal anesthesia. Patients who required additional anesthesia affecting their level of consciousness were excluded (14 patients: 8 [21%] in the standard group and 6 [16%] in the participation group; P = .6290). In every case, additional anesthesia was required for pain control and not because the patient was uncomfortable watching the surgical procedure.
Rehabilitation
All patients underwent the same postoperative rehabilitation protocol. Full weightbearing on the operated leg was allowed immediately after surgery. The patients wore a cryotherapy brace for 1 week. They started physical therapy on the day after surgery. They had follow-up visits with their surgeon at 6 weeks and 6 months. They were also reviewed by a sports medicine physician at 3, 4.5, and 9 months.
An isokinetic and functional analysis was performed at 6 months and repeated later on as needed. This was our main criterion to allow patients to return to their sports activities. The following target dates were adjusted based on the results of the above tests. Cycling and swimming were allowed between 1 and 1.5 months. Simple running was allowed at 3 months. Weightbearing sports were allowed at 6 months, on average, but without contact. Contact sports were allowed between 8 and 9 months after surgery, on average.
Study Endpoints
Patients filled out various self-administered questionnaires the day before the procedure and again the first day after surgery. The preoperative questionnaire consisted of a set of questions to evaluate the patient’s knowledge about ACL reconstruction. 26 The postoperative questionnaire included the same one filled out before surgery to evaluate comprehension and 3 additional satisfaction-related surveys: visual analog scale (VAS) for satisfaction, 35 Net Promoter Score (NPS), 13 and Evaluation du Vécu de l’Anesthésie LocoRégionale (EVAN-LR). 27 All patients were reviewed in person after a minimum follow-up of 1 year. Satisfaction was measured again using the VAS and NPS. Outcomes (patient-reported outcome measure [PROM] scores) were also determined at this time point.
Primary Endpoint: Comprehension
The comprehension questionnaire completed the day before the procedure and again the first day after surgery was based on the one described by Matava et al. 26 It had single-choice or multiple-choice questions ranging from general ones such as “Where is the ACL located?” to more specific ones such as “What is the retear rate after ACL reconstruction surgery?” The percentage of correct answers was calculated from 0% to 100%. This questionnaire has been validated in the literature for the comprehension of perioperative care inherent to ACL reconstruction.
We used 2 tools to measure confounding factors affecting comprehension during the preoperative phase. The validated Tampa Scale for Kinesiophobia 11 was used to assess patients’ fears relative to the retear risk. A higher score indicates that a patient has a greater fear of retearing the reconstructed ACL. The Knee Self-Efficacy Scale (K-SES) 37 is a validated survey in which patients report how certain they are about performing the task right now, despite knee pain/discomfort. In the second part of this survey, the patients report how certain they feel about their future capabilities. A higher score in the first part indicates that the patient is confident about the knee’s present physical performance/function. A higher score in the second part indicates that the patient has confidence in the future physical performance/prognosis of his/her knee. This allowed us to identify patients who lacked confidence in their ability to regain full function of their knee in the future or conversely identify those with disproportionally high expectations of surgery and its potential outcomes. These are self-administered measures validated in the context of ACL injuries that were completed the day before surgery.
Secondary Endpoint: Satisfaction 24 and PROMs
Satisfaction was evaluated the day before and the day after surgery using 3 validated measures: the VAS, 35 the NPS, 14 and the EVAN-LR. 27
VAS Satisfaction. 34,35
Patients were asked to rate how much they were satisfied with their care on a scale from 0 to 10. They were told that a score of “0” meant extremely dissatisfied and that a score of “10” meant extremely satisfied.
Net Promoter Score. 14,19
This tool is used in the marketing field to determine how satisfied a customer is with a product. 30 A parallel can be drawn with the medical field as a whole to evaluate a patient’s satisfaction with his/her medical care. In our study, patients were asked about their willingness to advise a relative to undergo the same operation on a scale from 0 to 10. Based on their score, patients were divided into promoters (9 or 10), passives (7 or 8), and detractors (≤6). The NPS is determined as follows: NPS = % promoters – % detractors.
EVAN-LR. 6,27
This measure is used to determine the satisfaction of patients receiving regional anesthesia. Based on their expectations, patients assigned a grade ranging from 1 (not as good as I expected) to 5 (much better than I expected) to 19 items over 5 dimensions: care provided by team, preoperative information, discomfort, wait before appointment, and pain. All dimension scores were linearly transformed to a 0-to-100 scale, with “100” indicating the best possible level of satisfaction and “0” the worst. A higher score indicates greater satisfaction with the care.
Patient-Reported Outcome Measures
PROM scores were determined at the 1-year follow-up visit using questionnaires given to the patients: Knee injury and Osteoarthritis Outcome Score (KOOS), 31,33 Lysholm score, 36 International Knee Documentation Committee (IKDC) subjective form, 15,17 and Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale. 38
Statistical Analysis
Based on recommendations 20 for pilot studies (initial evaluation of a patient’s comprehension and satisfaction depending on whether he/she was involved in his/her ACL reconstruction surgery), 31 patients were enrolled in each study group. Before the statistical analysis was initiated, missing, irregular, or inconsistent data were identified. Once these were corrected, the database was locked. The analysis was conducted on the locked database. The patients’ characteristics in each group at enrollment were summarized with descriptive statistics appropriate for the type of variable. These descriptive statistics included the number of nonmissing observations and the mean ± SD for continuous variables as well as the number of nonmissing observations and the frequency (%) for categorical variables. Continuous variables were compared using the Student t test or Mann-Whitney test, if necessary. Categorical variables were compared using the chi-square test or Fisher exact test, if necessary. Because the preoperative comprehension (Matava) scores differed between groups, analyses of the postoperative improvement in the comprehension score were adjusted with linear regression based on the preoperative score. All the reported P values are for 2-tailed tests, and a 5% threshold was used for significant differences. Statistical analyses were carried out with STATA 14.1 software (StataCorp).
Results
Comparability of 2 Groups at Enrollment
The 2 groups were comparable at enrollment in terms of sex, age, body mass index, time between injury and surgery, Tampa Scale for Kinesiophobia score, K-SES score (current, future, total), and education level (Table 1).
Patient Characteristics at Enrollment a
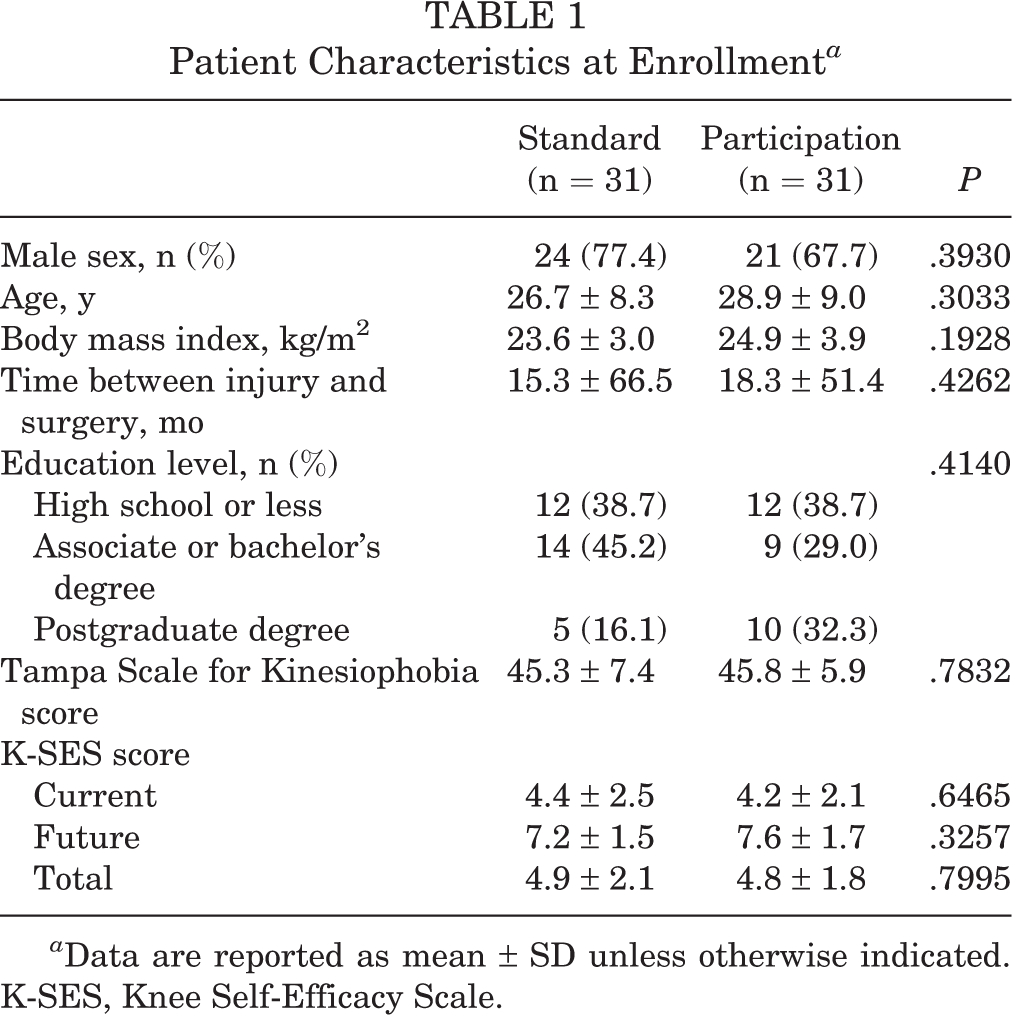
a Data are reported as mean ± SD unless otherwise indicated. K-SES, Knee Self-Efficacy Scale.
Comprehension
The preoperative Matava score in the standard group averaged 53.1 ± 16.3 and that of the participation group averaged 64.1 ± 11.2 (P = .0053). The postoperative score averaged 55.8 ± 13.9 for the standard group and 71.1 ± 10.3 for the participation group (P < .0001) (Table 2). Patients in the standard group improved their score by a mean of 2.7 ± 5.6 points, while those in the participation group improved their score by a mean of 7.1 ± 5.3 points (P = .0024). After adjusting the analysis based on the preoperative score, the postoperative score improved more in the participation group, with a mean improvement of 2.6 points in the standard group and 8.0 points in the participation group (P < .0010). These results indicate that a patient viewing the screen during surgery improves his/her comprehension.
Matava Scores a
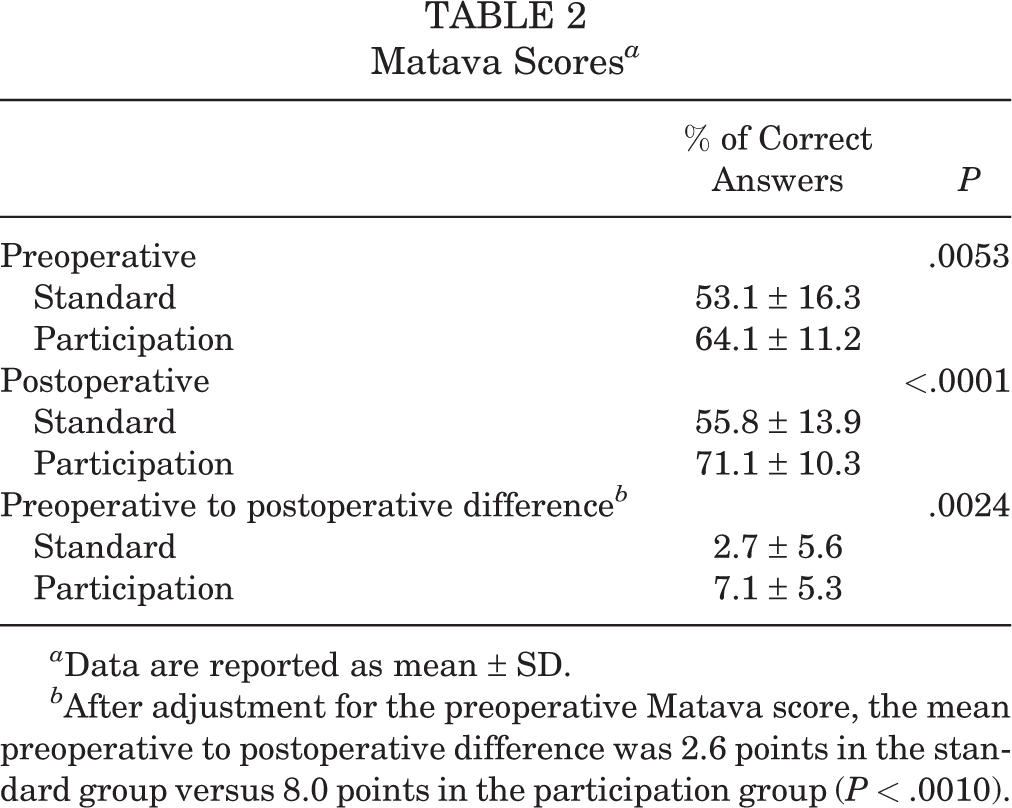
a Data are reported as mean ± SD.
b After adjustment for the preoperative Matava score, the mean preoperative to postoperative difference was 2.6 points in the standard group versus 8.0 points in the participation group (P < .0010).
VAS Satisfaction
The mean VAS satisfaction score immediately postoperatively was 8.9 ± 1.9 in the standard group and 9.8 ± 0.6 in the participation group (P = .0033). These results indicate that a patient’s involvement in the surgical procedure improves satisfaction. After a minimum follow-up of 1 year, the mean VAS satisfaction score was still higher in the participation group versus the standard group (9.8 ± 0.6 vs 9.1 ± 1.7, respectively; P = .0145).
Net Promoter Score
In the standard group, there were 21 (67.7%) promoters, 9 (29.0%) passives, and 1 (3.2%) detractor, which resulted in an NPS of 64.5% in the immediate postoperative period. In the participation group, there were 30 (96.8%) promoters, 1 (3.2%) passive, and 0 (0.0%) detractors, which resulted in an NPS of 96.8% in the immediate postoperative period (P = .0057). The mean postoperative NPS was 9.5 ± 0.6 in the participation group and 8.5 ± 1.7 in the standard group (P < .0050). After a minimum follow-up of 1 year, the NPS was still higher in the participation group versus the standard group (100.0% vs 71.0%, respectively; P = .0046).
EVAN-LR
The mean postoperative total EVAN-LR score was 84.6 ± 9.9 in the standard group and 89.1 ± 6.5 in the participation group (P = .0416). The patients in the participation group had significantly higher satisfaction scores in the discomfort and pain dimensions (Table 3).
Postoperative EVAN-LR Scores a

a Data are reported as mean ± SD. EVAN-LR, Evaluation du Vécu de l’Anesthésie LocoRégionale.
Functional Outcomes
After a minimum follow-up of 1 year, there was no difference between the participation and standard groups for the KOOS (Table 4) and Lysholm scores (84.7 ± 6.0 vs 87.3 ± 6.2, respectively; P = .102).
Postoperative KOOS Scores a

a Data are reported as mean ± SD. KOOS, Knee injury and Osteoarthritis Outcome Score.
IKDC Subjective Form
After a minimum follow-up of 1 year, the IKDC subjective score was higher in the participation group than the standard group (86.0 ± 7.5 vs 80.0 ± 7.4, respectively; P = .0023).
ACL-RSI Scale
After a minimum follow-up of 1 year, the mean ACL-RSI score of 80.9 ± 7.7 in the participation group was higher than the mean score of 74.3 ± 8.4 in the standard group (P = .0019). These results indicate that a patient’s involvement in the surgical procedure increases his/her confidence in his/her knee and how it will perform.
Discussion
We found a significant difference in comprehension and satisfaction between the 2 study groups. The participation group had a significantly better understanding of the procedure and of their perioperative care after being allowed to watch the arthroscopic screen and receiving additional intraoperative information. Patient engagement during ACL reconstruction surgery significantly improved their comprehension, satisfaction, and outcomes at 1 year for the IKDC form and ACL-RSI scale but not for the Lysholm score or the KOOS.
Matava et al 26 developed a questionnaire to evaluate patients’ knowledge about ACL reconstruction and identify the most confusing or less well-understood aspects. The aim was to evaluate the patients’ perception of the surgical procedure. They found that 32% of patients believed that surgery involved simply suturing the torn ACL, 67% believed that it was impossible to walk normally with a torn ACL, and nearly 50% of patients believed that the ACL could heal itself without surgery. A snapshot of these sometimes erroneous beliefs from a cohort of more than 200 patients reinforced our idea that information in any form is vital for patients to properly understand the stakes of this surgery. Also, because this information improves comprehension, patients appear to ultimately be more satisfied with the care that they receive.
Although the participation group had a higher preoperative comprehension score than the standard group, the former group still benefited from the intraoperative information provided to them and the ability to see their surgery in real time. The participation group had a significant increase (P = .0024) in the number of correct answers in the Matava score (mean, +7.1 vs +2.7 in the standard group), even when the score was adjusted to the score at enrollment (mean, +8.0 vs +2.6 in the standard group; P < .0010). Our study showed that for general questions related to ACL reconstruction, the patients in the participation group improved their score more than the patients in the standard group. Repeating the information is beneficial for comprehension, and the patients in the participation group benefited from this. We did not study learning and information behaviors in our patients, but it is possible that some of them have a visual memory that helped them to better understand the surgical procedure. Patients in both groups received the same preoperative information and knew that they were participating in a study on surgery comprehension. In our opinion, the fact that some patients were in the participation group did not encourage them more to read the preoperative information.
The difference in the preoperative Matava scores is because 1 patient in the standard group had a very low preoperative score (10% correct answers). This resulted in a low mean score for the standard group. This patient had a 10-point improvement on the comprehension score, which was greater than the observed mean difference. This indicates that this patient also reduced the impact of participation. He gave wrong answers to simple questions, which he saw during the provision of care (eg, wearing of brace). This is confirmed by the larger improvement in the postoperative Matava score by the participation group after adjusting for the preoperative score.
Satisfaction was significantly higher in patients who were involved in their surgery. The mean VAS satisfaction score was significantly greater in the participation group immediately postoperatively (9.8 ± 0.6 vs 8.9 ± 1.9, respectively; P = .0033) and after the minimum 1-year follow-up (9.8 ± 0.6 vs 9.1 ± 1.7, respectively; P = .0145) compared with the standard group. This tool, which is easy to use and easy for patients to understand, is typically employed in the self-assessment of pain. It can also be used to classify various factors, such as satisfaction about a procedure, on a graduated scale. 20
The NPS was also significantly better in the participation group immediately postoperatively (96.8% vs 64.5%, respectively; P = .0057) and after the 1-year follow-up (100.0% vs 71.0%, respectively; P = .0046) compared with the standard group. The NPS is used in the marketing field to gauge overall customer satisfaction with certain new products or services. 30 We decided to use it to assess our patients’ opinion of the new intervention, that is, being involved in the surgical procedure by watching surgery in real time. The NPS has been validated for the assessment of medical care by Hamilton et al. 14
The EVAN-LR is used to assess the satisfaction of patients receiving regional anesthesia. 27 We used it to assess patient satisfaction on certain dimensions when they received the same type of anesthesia. The mean score was significantly higher in the participation group than in the standard group (89.1 ± 6.5 vs 84.6 ± 9.9, respectively; P = .0416). Being allowed to watch the arthroscopic procedure did not make the patients uncomfortable. On the contrary, for the discomfort dimension, the mean satisfaction score was 89.5 ± 7.1 for the participation group versus 80.3 ± 14.6 for the standard group (P = .0189). Similarly, for the pain dimension, the mean satisfaction score was higher in the participation group than in the standard group (85.8 ± 13.2 vs 75.2 ± 19.2, respectively; P = .0269). The pain and discomfort dimension scores were collected during a period from surgery to a few hours postoperatively. We believe that the patients who were able to watch the arthroscopic phase felt less discomfort and pain during this period because they were busy watching the screen and thinking about their surgery.
Fourteen patients were excluded from the study because they felt pain at the time of the incision, which forced us to provide additional anesthesia. There was no difference in the proportion of patients excluded in each group (P = .6290).
Being able to watch the arthroscopic video screen and receiving additional information during surgery led to greater patient satisfaction with the surgical procedure overall. In our opinion, this study is unique because this type of intervention has not been described in the literature. Rossi et al 32 provided patients with a preoperative information video, which significantly improved their comprehension compared with that of patients who received traditional oral information only (78.5% correct answers in questionnaire vs 65.4%; P = .0001). Conversely, they found no difference in terms of satisfaction with the information received. To our knowledge, no other study has documented the effects of patients being allowed to watch their ACL reconstruction surgery in real time. This active patient participation also allowed the surgeon to deliver additional standardized information to each patient. This information was the same for all patients and in all stages of the treatment: during the surgical consultation, during the preoperative visit at which point a consent form was given to patients summarizing the goals of the study, and of course, during surgery.
We designed this study with direct patient participation in mind. Another option would have been to show patients a video of their surgery after it had been completed. However, we believe that the real-time aspect of our approach allows us to keep the patient’s attention, who is participating in the surgical procedure instead of being a passive spectator. Along with providing information, we believe that this type of care reassures the patient that the treatment has been conducted properly.
Fink et al 10 showed that the duration of the information session was the strongest predictor of comprehension. They also showed that adding other aids to repeat the information leads to better comprehension. Comprehension comes into play at several levels: during the first surgical consultation, the surgeon takes the time to explain the ins and outs of the injury, surgical procedure, and postoperative care to the patient. By allowing the patient to see the arthroscopic phase of surgery, the information is repeated, which ultimately leads to better understanding of the procedure and postoperative course. Also, the use of a video helps to improve patient compliance during scientific research and participation in an ongoing study. 39
McGaughey 28 showed that patients were less satisfied when they received fragmented or incomplete information. In that study, patients felt that they were well informed about the injury and surgical procedure but had not received enough information about the potential complications and postoperative course. To ensure that patients are as satisfied as possible, surgeons should discuss all elements of care.
Yet, satisfaction has several biases, and it is difficult to determine a patient’s satisfaction with the surgical procedure because various other factors come into play (kindness of hospital staff, infrastructure, expectation before surgery, etc). 4,7 We feel that known and measurable confounding factors were controlled in this pilot study. The next step will be a randomized study involving more patients to fully control the confounding factors.
Our research is driven by the fact that we believe that it is vital for patients to be satisfied because their satisfaction level may affect their outcomes. 2 In fact, patients who were involved in their surgery had a higher IKDC subjective score than those who were not (86.0 ± 7.5 vs 80.0 ± 7.4, respectively; P = .0023). The IKDC subjective form 15,17 is used to evaluate how a patient feels about his/her knee’s function and symptoms. The ACL-RSI score was also better in the participation group than the standard group (80.9 ± 7.7 vs 74.3 ± 8.4, respectively; P = .0019). Müller et al 29 have shown that this scale predicts the return to sports. Also, as shown by Webster et al, 38 return to sports is related to psychological factors, which are evaluated by the ACL-RSI scale. The latter identifies which patients will have a harder time returning to sports. The French version of this scale has also been validated. 3
The study findings suggest that involving patients in their surgery not only improves their comprehension but also their satisfaction. By participating in their surgery, patients had a positive attitude relative to their treatment course, which also led to better outcomes.
We found statistically better IKDC and ACL-RSI scores in the participation group. In their article, Irrgang et al 17 reported a 9-point difference in IKDC scores as relevant. However, they had mean scores of 71.3 and 71.7, whereas in our study, the scores were 80 or higher in both groups. For the KOOS, an 8-point threshold can be used to conclude that there is a difference between the 2 groups. 25 We did not reach this threshold between the groups in our study.
Unlike the IKDC form, there is no threshold value for the ACL-RSI scale. It is difficult to determine if a statistically significant difference is also clinically significant. We found higher ACL-RSI scores in the participation group versus the standard group (P = .0019). The difference found in our study was greater than the one reported by Thomeé et al, 37 who concluded that there was a clinically significant difference based on the ACL-RSI scale in their study.
Several authors have found that return to sports was improved in patients with a good attitude toward resuming their activity. 1,21,38 This good psychological response is evidenced by improvements in the ACL-RSI score and IKDC subjective score. In our study, explaining the procedure to patients while they watched the arthroscopic screen led to greater satisfaction and better understanding of the treatment pathway. Over time, this better understanding and greater satisfaction contribute to the development of positive attitudes that lead to better functional outcomes.
Our study has certain limitations. First, excluding patients who required additional anesthesia for pain control was necessary because the different types of anesthesia would have affected the patients’ consciousness and introduced a bias. The proportion of patients excluded in each group was not significantly different (P = .6290). Second, our study was not randomized, as it was designed to be a pilot study, which is the first step in our research pathway. Third, although there was a difference in the education level between the 2 groups, this difference was not statistically significant. A larger study will be needed to confirm the results of our pilot study and more accurately measure the expected effects of patient participation.
Conclusion
Active patient participation during surgery, in which the patient can see the arthroscopic procedure in real time and is provided with additional information intraoperatively, increases understanding of the procedure and leads to greater satisfaction and potentially better outcomes.
Footnotes
Acknowledgment
The authors are grateful to Joanne Archambault, PhD, for English-language assistance.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C. is a paid consultant for Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hôpitaux de Toulouse (No. 01-0447).