
Abstract
Background:
Patients with public insurance often face barriers to obtaining prompt orthopaedic care. For patients with recurrent traumatic anterior shoulder instability, delayed care may be associated with increasing bone loss and subsequently more extensive surgical procedures.
Purpose/Hypothesis:
The purpose of this study was to evaluate whether differences exist in patients undergoing treatment for shoulder instability between those with Medicaid versus non-Medicaid insurance. We hypothesized that at the time of surgery, Medicaid patients would have experienced greater delays in care, would have a more extensive history of instability, would have more bone loss, and would require more extensive surgical procedures than other patients.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients were identified who underwent surgical stabilization for traumatic anterior shoulder instability between January 1, 2011, and December 1, 2015, at a single sports medicine practice. Clinic, billing, and operative records were reviewed for each patient to determine age, sex, insurance type, total number of instability episodes, time from first instability episode to surgery, intraoperative findings, and procedure performed. Glenoid bone loss was quantified by use of preoperative imaging studies.
Results:
During this time period, 206 patients (55 Medicaid, 131 private insurance, 11 Tricare, 9 workers’ compensation) underwent surgical stabilization for traumatic anterior shoulder instability. Average wait time from initial injury to surgery was 1640 days (95% CI, 1155-2125 days) for Medicaid patients compared with 1237 days (95% CI, 834-1639 days) for others (P = .005). Medicaid patients were more likely to have sustained 5 or more instability events at the time of surgery (OR, 3.3; 95% CI, 1.64-6.69; P = .001), had a higher risk of having 15% or more glenoid bone loss on preoperative imaging (OR, 3.5; 95% CI, 1.3-10.0; P = .01), and had a higher risk of requiring Latarjet or other open stabilization procedures as opposed to an arthroscopic repair (OR, 3.0; 95% CI, 1.5-6.2; P = .002) when compared with other patients.
Conclusion:
Among patients undergoing surgery for traumatic anterior shoulder instability, patients with Medicaid had significantly more delayed care. Correspondingly, they reported a more extensive history of instability, were more likely to have severe bone loss, and required more invasive stabilization procedures.
Acute traumatic anterior shoulder dislocations are relatively common, with a reported incidence of 1.7% in the general population. 25 These injuries are typically associated with detachment of the anterior-inferior labrum (Bankart lesions), bony Hill-Sachs lesions of the humeral head, superior labral tear from anterior to posterior (SLAP) lesions, and glenoid rim fractures. The chance of recurrence after a single dislocation is high, especially in young and active individuals. 26,33,38 Recurrent instability events put patients at increasing risk for glenoid and humeral bone loss, worsening instability, and more severe intra-articular injury. 10,13 With progressive bone loss, more extensive stabilization procedures, sometimes including bone augmentation, become necessary to prevent recurrence. 7,12,20 For these reasons, many authors have recommended early surgical intervention for patients with traumatic anterior shoulder instability who are at high risk for recurrence. 4
Previous authors have found that insurance coverage affects timeliness of care for patients with anterior cruciate ligament injuries and meniscal tears, noting that patients with private insurance undergo surgery more expeditiously than those without. 2,21,30 In 2015, 9.1% of all Americans were uninsured and 19.6% had Medicaid. 3 With a limited number of providers accepting Medicaid, patients enrolled in Medicaid as well as those without insurance may have difficulty obtaining office visits and scheduling elective surgery. 2,5,8,11,21,23,30,36 The impact of insurance coverage on access to care for patients with traumatic anterior shoulder instability has not been previously investigated.
The purpose of this study was to evaluate whether differences exist in patients undergoing treatment for traumatic anterior shoulder instability between those with Medicaid versus non-Medicaid insurance. We hypothesized that at the time of surgery, Medicaid patients would have experienced greater delays in care, would have a more extensive history of instability, would have more bone loss and chondral damage, and would require more extensive surgical procedures.
Methods
This institutional review board–approved study was a retrospective review of prospectively collected data from patients undergoing surgery for traumatic anterior shoulder instability at a single university-based sports medicine practice. New patients to the practice are not screened for insurance prior to being seen; they are scheduled on a first-come, first-served basis. Data were collected for each of the 5 surgeons within the practice. Each of these 5 surgeons is sports medicine fellowship trained and is highly familiar with both arthroscopic and open techniques of shoulder stabilization surgery. All first-time dislocators undergo a full discussion of the risks and benefits of nonoperative treatment at the initial visit, with all surgeons in the study generally recommending surgical treatment for young (<20 years), highly active patients.
Patients were identified by a Current Procedural Terminology (CPT) code search for procedures performed: 23455 (capsulorrhaphy, anterior, with labral repair [eg, Bankart procedure]), 23460 (capsulorrhaphy, anterior, any type; with bone block), 23462 (capsulorrhaphy, anterior, any type; with coracoid process transfer), and 29806 (arthroscopy, shoulder, surgical, capsulorrhaphy). Patients were included in the series if they underwent surgical treatment of traumatic anterior shoulder instability between January 1, 2011, and December 1, 2015. Patients were excluded if they had a history of prior shoulder surgery, had no history of shoulder trauma, had no history of a known shoulder instability event, had a primary diagnosis of posterior shoulder instability, had a primary diagnosis of atraumatic multidirectional instability, had unclear insurance coverage, or were prisoners.
Chart Review
Clinic notes were comprehensively reviewed for each patient to determine age at surgery, sex, the total number of instability episodes experienced, the number of days passed from the first instability episode to the visit with the orthopaedic surgeon, the number of days passed from the first instability episode to surgery, and the mechanism of the first instability episode (sports related or non–sports related). Subluxations and dislocations were both considered instability events.
Operative records were reviewed for each patient to determine intraoperative findings and procedures performed. Based on these records, labral tears were classified into the following categories: anterior labral tears; posterior labral tears; SLAP tears; anterior and posterior labral tears; anterior labral tears and SLAP tears; anterior, posterior, and SLAP tears; and 360° labral tears. As described by Lo and Burkhart, 19 in a right shoulder, anterior labral lesions were defined as involving the 2- to 6-o’clock positions, posterior labral lesions were defined as involving the 6- to 10-o’clock positions, and SLAP lesions were defined as involving the 10- to 2-o’clock positions. Labral injuries extending into adjacent regions were considered distinct only if they involved at least two-thirds of that region. 19 Where noted, the presence of chondral injuries of the glenoid and/or humerus was recorded.
Billing records were reviewed for each patient to determine insurance coverage. Based on coverage, patients were categorized into 4 groups: Medicaid, private insurance, Tricare (health care program for beneficiaries of the US Department of Defense), and workers’ compensation.
Image Review
Preoperative cross-sectional images were reviewed by a single sports medicine fellowship–trained orthopaedic surgeon (R.A.A.) to quantify glenoid and humeral bone loss. Computed tomography (CT) scans with 3-dimensional (3D) reconstructions were used to perform measurements wherever possible. If only magnetic resonance images (MRIs) were available, they were used instead. 17 Glenoid bone loss was measured through use of the perfect circle method originally described by Huysmans et al. 14 An en face view of the glenoid was used to fit a circle to the glenoid, lining up with the posteroinferior glenoid rim, and bone loss was calculated as the diameter of the glenoid defect divided by the diameter of the circle. Humeral bone loss was measured as described by Kodali et al 16 as the maximal width and depth of a Hill-Sachs defect on axial and coronal sections. Patients with 15% or more glenoid bone loss were then identified for analysis. Although critical bone loss has typically been described between 20% and 25%, 18 more recent literature has demonstrated that as little as 13.5% of bone loss in higher demand patients can lead to failure of an arthroscopic Bankart repair. 27
Statistical Analysis
Descriptive statistics were calculated as mean and 95% CI or frequency and proportion where appropriate. Differences in wait time from initial injury to first office visit and to surgery and differences in glenoid bone loss were compared by use of Wilcoxon rank-sum tests owing to skewedness of the data. For patients with Medicaid versus other insurance carriers, categorical differences involving only 2 categories were compared by use of chi-square tests. To examine the number of instability events, the chi-square test for trend was used. P values of less than .05 were considered statistically significant. Odds ratios (ORs) were used to compute the relative odds of various outcome measures based on insurance. All statistical analysis was performed by use of Stata 12 (StataCorp).
Results
Our search identified 206 surgical stabilization procedures performed between January 1, 2011, and December 1, 2015, that met the study inclusion criteria. Of these patients, 55 had Medicaid, 131 had private insurance, 11 had Tricare, and 9 had workers’ compensation. Demographic information is given in Table 1. Overall, 110 patients reported that their first instability event was sports related. In 26 cases, details of the initial injury mechanism could not be ascertained from the chart review. Of the remaining patients, initial injury mechanisms were as follows: 25 falls, 7 motor vehicle collisions, 6 weight-training injuries, 6 seizures, 5 fights, 4 heavy lifting injuries, 3 motorcycle accidents, 3 white water recreation injuries, 3 injuries while rough-housing, 2 assaults, 2 climbing injuries, 1 CrossFit injury, 1 trampoline injury, 1 injury diving off a boat, and 1 injury during a military drill.
Demographic Data for Patients Undergoing Surgery for Traumatic Anterior Shoulder Instability Based on Insurance Type

Although a large amount of variability was found in wait times, delays from injury to office visit and to surgery were significantly longer for Medicaid patients than for other patients. The average wait time to first office visit was 1538 days (95% CI, 1052-2024 days) for Medicaid patients compared with 1122 days (95% CI, 730-1514 days) for others (P = .002), and the average wait time to surgery was 1640 days (95% CI, 1155-2125 days) for Medicaid patients compared with 1237 days (95% CI, 834-1639 days) for others (P = .005). For patients for whom the initial injury date was known, only 14 of 49 (29%) Medicaid patients had surgery within the first year of their initial instability event compared with 74 of 135 (55%) other patients (OR, 0.3; 95% CI, 0.2-0.7; P = .002), reflecting the longer time that Medicaid patients waited to be seen. The mean time from initial office visit to surgery was 102 days (95% CI, 13-191 days) for patients with Medicaid and 115 days (95% CI, 57-173 days) for patients with other insurance (P = .294). This difference remained nonsignificant when Tricare patients were separated from the analysis.
Patients with Medicaid also reported having had more shoulder instability events prior to surgery than patients with other insurance (Table 2). The number of instability events that occurred prior to surgery was recorded for 47 of 55 patients with Medicaid, 101 of 131 patients with private insurance, 10 of 11 patients with Tricare, and 6 of 9 patients with workers’ compensation. Of these patients, 28 of 47 (60%) patients with Medicaid had sustained 5 or more shoulder instability events prior to surgery, compared with 36 of 117 (30%) patients with other insurance (OR, 3.3; 95% CI, 1.6-6.7; P = .001). Patients with Medicaid were also more likely to report instability events during sleep, an indication of significant bone loss; 15 of 55 (27%) Medicaid patients reported instability events occurring during sleep compared with 9 of 151 (6%) other patients (OR, 5.9; 95% CI, 2.4-14.5; P < .001).
Number of Instability Events at the Time of Surgery Based on Insurance Type a
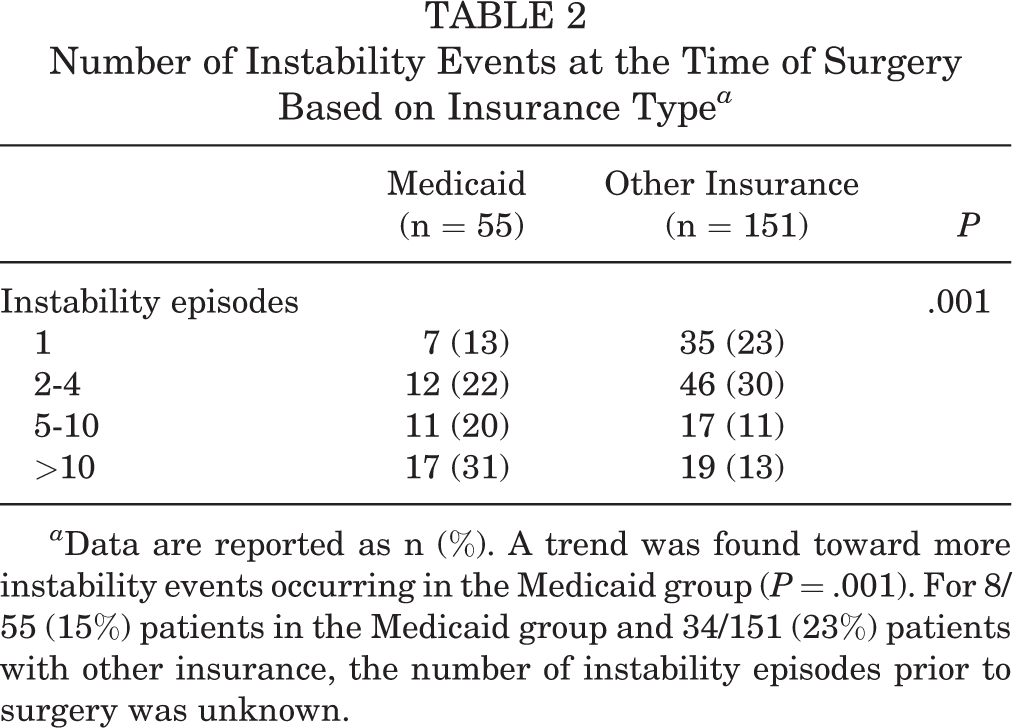
a Data are reported as n (%). A trend was found toward more instability events occurring in the Medicaid group (P = .001). For 8/55 (15%) patients in the Medicaid group and 34/151 (23%) patients with other insurance, the number of instability episodes prior to surgery was unknown.
Preoperative MRI and/or CT scans were available for quantification of bone loss in 42 of 55 patients with Medicaid, 69 of 131 patients with private insurance, 7 of 11 patients with Tricare, and 1 of 9 patients with workers’ compensation. The average preoperative glenoid bone loss was 8.3% (95% CI, 4.8%-11.9%) in patients with Medicaid compared with 4.9% (95% CI, 3.4%-6.3%) in other patients (P = .224) (Table 3). More Medicaid patients had substantial bone loss compared with patients with other insurance. Whereas 11 of 42 (26%) Medicaid patients had 15% or more glenoid bone loss preoperatively, this was true for only 7 of 77 (9%) other patients (OR, 3.5; 95% CI, 1.3-10.0; P = .01). The distributions of labral tear types among patients with Medicaid, private insurance, Tricare, and workers’ compensation were similar (Table 4). Significant chondral defects were present in 13 of 55 (24%) patients with Medicaid and 26 of 151 (17%) other patients (OR, 1.5; 95% CI, 0.7-3.2; P = .30).
Glenoid and Humeral Bone Loss as Measured on Preoperative CT or MRI a

a Data are reported as mean (95% CI). CT, computed tomography; MRI, magnetic resonance imaging.
Labral Tears Based on Operative Records a

a Data are reported as n (%). SLAP, superior labral tear from anterior to posterior.
All 5 surgeons shared the widely accepted approach to surgical decision making for shoulder instability, in which the decision to perform an open Bankart repair or a Latarjet procedure is based on a number of demographic and pathoanatomic factors known to increase postoperative recurrence rates after arthroscopic repair. These include greater than 20% bone loss, an engaging Hill-Sachs lesion with an inverted pear glenoid, bipolar lesions (>15% glenoid bone loss with a Hill-Sachs defect), and young male collision athletes. 1,6,24,32 Overall, 18 of 55 (33%) patients in the Medicaid group underwent Latarjet procedure or other open stabilization surgery compared with 21 of 151 (14%) patients with other insurance (OR, 3.0; 95% CI, 1.5-6.2; P = .002). Among Medicaid patients, we documented 36 arthroscopic labral repairs, 13 Latarjet procedures, 4 open Bankart repairs, 1 arthroscopic capsulorrhaphy, and 1 open glenoid augmentation with tibial plafond allograft and humeral head resurfacing. Among privately insured patients, there were 107 arthroscopic labral repairs, 10 open Bankart repairs, 9 Latarjet procedures, 4 arthroscopic capsulorrhaphies, and 1 open capsulorrhaphy. Among Tricare patients, we noted 10 arthroscopic labral repairs and 1 Latarjet procedure. All workers’ compensation patients underwent arthroscopic labral repair.
Discussion
These results support the hypothesis that among patients undergoing surgery for traumatic anterior shoulder instability, Medicaid insurance coverage is associated with greater delays to presentation and surgery, more significant bone loss, and more invasive surgical stabilization procedures than other types of insurance. No significant correlation was found between insurance type and chondral damage.
Patients with Medicaid insurance were found to have significantly increased lag times from initial dislocation to initial office consultation and surgery. These findings are similar to those previously reported for patients with anterior cruciate ligament and meniscal injuries, where Baraga et al 2 and other studies 8,21,23,30 have described delays in both diagnosis and surgical treatment of patients without private insurance. It is not known whether the patients in this study who experienced significant delays between their first instability event and evaluation at our institution attempted to obtain care elsewhere during this interval and, if so, whether they were successful in doing so. Although purely speculative given the retrospective nature of the study, this delay in care may be due to patients’ reluctance to seek physician care or a lack of awareness regarding which type of specialist to see. Previous studies have suggested that such delays may be attributable to some patients’ reluctance to see a physician, the lack of practices willing to care for patients with Medicaid, or practices offering a limited number of clinic time slots to patients with Medicaid. 15,23,28,29 Wiznia et al 37 found that patients with Medicaid were significantly more likely to be denied an appointment because of a lack of referral from a primary care physician. This lack of established primary care could have delayed patients in finding providers who accept their insurance and may underline an overall distrust that patients of lower socioeconomic status have in the health care system. 22 As well, previous epidemiologic data have suggested that patients of lower socioeconomic status may interpret their symptoms as not worrisome, therefore not even attempting to seek care. 34 Last, the financial loss associated with missing work may have swayed patients to not search for a provider.
In our practice, as a state institution, patients are scheduled for office consultation on a first-come, first-served basis, regardless of insurance type. With this policy, we found a somewhat similar incidence of patients arriving after initial dislocation, with roughly 10% more often in the “other insurances” group compared with Medicaid patients. Similarly, surgeries are scheduled based only on patient acuity and surgeon and patient availability. Interestingly, the time from initial office visit at our institution to surgery was actually shorter in the Medicaid group than in other patients, but this was not found to be statistically significant. This finding may reflect, at least in part, the increased severity of injury seen in this population and suggests that differences in care were not due to lack of follow-through on the part of patients with Medicaid.
In addition, the present study found that patients with Medicaid had sustained significantly more instability episodes at the time of surgery compared with other patients. The incidence of primary and recurrent anterior shoulder dislocations treated at emergency departments in the United States has been reported as 26.9 per 100,000 person-years. 39 Numerous factors have been investigated as prognostic factors for recurrence, including male sex and younger age. 35 Sex and age were similarly distributed among patients with Medicaid and other insurance in this study.
Recurrent traumatic anterior shoulder instability has been associated with an increasing risk of significant glenoid bone loss. 10,31 In this study, patients with Medicaid experienced more instability events and greater delays in care and correspondingly had a higher incidence of severe bone loss than other patients. These significant glenoid defects have been associated with failure of arthroscopic stabilization procedures and are widely considered to be an indication for open stabilization procedures with or without bone graft. 6,9 Because of this, a higher proportion of Medicaid patients in this study required more extensive stabilization procedures. All 5 surgeons in our practice share a similar philosophy, recommending open as opposed to arthroscopic surgery to patients with recurrent traumatic shoulder instability and significant glenoid bone loss. Together, these data suggest that the delay in care seen in patients with Medicaid results in greater short-term morbidity, although the long-term effects are unknown.
This study has several limitations. Information regarding timing and number of instability episodes was based on patient report at preoperative visits. Recall bias may have occurred, as patients may have over- or underestimated the time passed since their initial instability event and the number of recurrent instability events they experienced. Although all 5 surgeons in the study routinely obtain cross-sectional imaging prior to performing shoulder stabilization surgery, not all patients’ preoperative imaging was available to us for review at the time of the study. This was likely attributable to patients with other insurance coverage obtaining MRIs ordered from outside providers, whereas the majority of Medicaid patients had imaging ordered by our institution after their initial visit.
In addition, patients were not randomized, and given the small sample population, the patient groups may be inherently different. Previously reported significant risk factors for recurrent anterior shoulder dislocation include male sex and young age; however, sex and age were not significantly different between groups. Patients were recruited from a single university-based practice in a single geographic location that treats a large proportion of Medicaid patients and thus may not reflect other orthopaedic practices. This study included only patients who underwent shoulder stabilization procedures and did not capture those who were unwilling or unable to undergo surgical treatment. Finally, the study encompassed the practices of 5 sports medicine–trained orthopaedic surgeons. Although this factor increased the generalizability of our findings to the overall population, these surgeons’ surgical decision making may have varied slightly from one another. However, the risk factors for recurrence after arthroscopic surgery for shoulder instability have been well described in the literature. 18 All surgeons in this study felt very comfortable with both arthroscopic and open shoulder stabilization surgery and ascribed to the same widely accepted philosophy of offering arthroscopic repair to patients at minimal risk for recurrence following arthroscopic repair and of recommending open surgery to patients with recurrent instability and significant risk factors for recurrence following arthroscopic repair.
Conclusion
Among patients undergoing surgery for traumatic anterior shoulder instability, those with Medicaid had significantly more delayed care. Correspondingly, they reported a more extensive history of instability, were more likely to have severe bone loss, and required more invasive stabilization procedures. To our knowledge, this is the first study examining insurance type as it pertains to the treatment of patients with shoulder instability. These results suggest that socioeconomic factors may substantially affect patients with shoulder instability.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.A.W. has received educational support from Smith & Nephew and hospitality payments from Axogen. R.A.A. has received grants from Arthrex and Depuy Mitek and consulting fees from Biomet, Biorez, and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the UConn Health Institutional Review Board (No. 16-117-3).