
Abstract
Background:
Studies examining the evolution of shoulder and elbow range of motion (ROM) in baseball pitchers over a single season have yielded inconsistent results.
Purpose:
To evaluate shoulder and elbow ROM in Major League Baseball (MLB) pitchers over a single season and to assess for correlations between these changes and measures of a pitcher’s workload.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Bilateral shoulder ROM (internal rotation [IR], external rotation [ER], and total range of motion [TROM]) was assessed in 92 MLB pitchers pre- and postseason. Shoulder forward flexion (FF) was measured in 64 pitchers, horizontal adduction (HA) was measured in 87 pitchers, and elbow ROM was measured in 86 pitchers. Data collected included demographics (age, height, weight, and body mass index) and measures of workload for pitchers (pitches thrown, innings pitched, and mean fastball velocity). Pitchers were not specifically excluded if they had an injury during the season but had recovered and were actively pitching at the time of postseason measurements. The change in motion from pre- to postseason was measured and the associations with player demographics and workload were calculated by use of the Pearson correlation coefficient.
Results:
On average, pitchers demonstrated an increase in dominant shoulder ER from 118.8° to 125.4° (P < .001) and TROM from 173.1° to 181.7° (P < .001). HA was increased by an average of 15.7° (P < .001). The average shoulder IR (P = .189), FF (P = .432), and elbow ROM (flexion, P = .549; extension, P = .185) remained similar over the span of the season. Average glenohumeral IR deficit did not increase. Pitcher demographics and measures of throwing workload (total pitches thrown, innings pitched, mean fastball velocity) were not significantly correlated with changes in shoulder or elbow ROM.
Conclusion:
Significant increases in dominant shoulder ER, TROM, and HA were identified in MLB pitchers over the course of a single baseball season. These ROM changes were not correlated with measures of pitching workload.
Injury rates in professional baseball players are increasing, with nearly half of injuries occurring in the shoulder and elbow. 3,4,14 In particular, shoulder and elbow injuries, including injuries to the labrum, rotator cuff, and ulnar collateral ligament of the elbow, are common in professional pitchers. 9,10,14 However, predictors of these injuries are not well defined. Possible risk factors for these injuries that have been investigated include hip range of motion (ROM) deficits, parameters for workload such as pitch count and innings pitched, pitch velocity, and throwing mechanics. 9,10,22,26 Likewise, alterations in shoulder and elbow ROM have been linked to shoulder and elbow injuries in baseball players. 2,13,16,17,19 –21,24 As a result, several authors have sought to evaluate the evolution of shoulder and elbow ROM over a single baseball season; however, these findings have been inconsistent. 5,7,15 Studies have reported similar glenohumeral ROM measurements between spring training and the end of a collegiate baseball season. 5 Freehill at al 7 reported that internal rotation (IR) and total ROM significantly increased across a season in professional starting pitchers, whereas changes in external rotation (ER), IR and total ROM among all pitchers studied were not statistically significant. Furthermore, Reinold et al 15 reported a significant decrease in shoulder IR (–9.5°), total motion (–10.7°), and elbow extension (–3.2°) that occurred immediately after pitching in the dominant arm, and these changes persisted 24 hours after pitching. Therefore, much remains to be elucidated regarding changes in ROM over the course of a baseball season.
If shoulder and elbow ROM do change over a season, it is important to know whether measures of pitching workload can predict these changes. This may allow early identification of pitchers possibly at risk for developing shoulder and elbow injury and can alert the medical teams caring for these athletes to use early intervention strategies, such as workload alterations and/or stretching programs. The purpose of this study was to (1) compare the pre- and postseason shoulder and elbow ROM in a group of Major League Baseball (MLB) pitchers and (2) determine whether any observed changes in ROM of the shoulder or elbow across a season correlated with measures of pitching workload.
Methods
This study was approved by the institutional review board of our institution. A comprehensive physical examination was performed on all pitchers invited to Major League spring training for a single MLB organization over the course of 6 seasons (2010-2015). Among other measures, the examination consisted of an assessment of bilateral shoulder and elbow ROM. The player’s ROM was assessed again at the end of the season. Only pitchers who were playing without restriction, were free from injury at the time of examination, and were available for both pre- and postseason measurements were included in the study. Pitchers who were not able to pitch because of injury at the time of pre- and postseason measurements were excluded. Player demographics recorded at the time of the examination included handedness, age, height, weight, and body mass index (BMI).
Assessing Shoulder and Elbow ROM
A pitcher’s ROM was measured during spring training and at the end of the season. Goniometric measurements were obtained bilaterally for shoulder forward flexion (FF), ER at 90° of abduction, IR at 90° of abduction, and horizontal adduction (HA). All shoulder measurements were performed with the pitcher lying passively in the supine position; the same 2 physical therapists (J.M.Z., D.P.) performed all measurements, one manually moving the upper extremity to the point of initial tissue resistance and the other performing goniometric measurements using a standardized Jamar goniometer 1 (Appendix Figure A1). The flexion measurement was performed with the stationary arm of the goniometer parallel to the table and the moving arm positioned along the humerus in line with the lateral epicondyle and the axis of rotation with the central aspect of the humeral head. Measurements of shoulder flexion ROM were composite in nature, taking into account functional movement from both the glenohumeral and scapulothoracic joints. Therefore, minimal scapular stabilization was instituted, and ideal measurements were considered to be 180° of motion. ER and IR were assessed with the pitcher’s shoulder in 90° of abduction and the elbow flexed 90°. The stationary arm of the goniometer was positioned parallel to the table and the moving arm was placed along the ulnar shaft in line with the ulnar styloid, with the axis of rotation centered at the olecranon process. A small bolster was placed under the humerus to keep the center of rotation in line with the frontal plane of the body, preventing the humerus from moving posteriorly.
Measurements were taken by one therapist (J.M.Z. or D.P.) using a C-shaped hand placement (thumb anterior to coracoid and fingers posterior to scapula) over the coracoid process to minimize excessive movement of the scapula during the measurement. 25 HA was measured from above the player’s head with the player supine. The stationary arm of the goniometer was placed parallel to the table, while the moving arm was placed along the shaft of the humerus in line with the lateral epicondyle and the axis of rotation centered at the mid-humeral head. Measurements were taken while one therapist stabilized the player’s scapula with one hand and used the other hand to move the player’s arm across his body into the motion of HA to the point of initial tissue resistance. HA has been used as a means of posterior capsule assessment in which loss could significantly affect ROM. 8,18
Elbow ROM was measured with the player in the seated position and the shoulder flexed 90°. The player was asked to actively extend the elbow with the forearm supinated and to subsequently fully flex the elbow. Measurements were taken at the 2 end ranges by the same physical therapist. The stationary arm of the goniometer was placed parallel to the floor in line with the shaft of the humerus and in line with the center of the humeral head, with the moving arm positioned along the midline of the central aspect of the radial/ulnar shafts and the axis of rotation at the lateral epicondyle (Appendix Figure A2).
Measures of Workload
For all pitchers, 3 different measures of workload were calculated. These included total pitches thrown over the course of the season, number of innings thrown, and mean fastball velocity in miles per hour. Mean fastball velocity was chosen as a metric because the fastball generates the greatest amount of shoulder and elbow torque. 6 Only pitches thrown in official games were used in these measures. This did not include throwing activity that occurred during spring training, in the bullpen, during practice sessions, or as a part of normal warm-up in preparation for live game throwing.
Intervention Protocol
ROM data were analyzed following spring training to assess the need for treatment interventions above and beyond normal maintenance programs. An intervention strategy was used if the dominant shoulder total ROM (TROM) deficit was 10% or greater compared with the nondominant shoulder and also if glenohumeral IR deficit (GIRD) was identified, if the HA ROM deficit was 10% or greater, or if shoulder flexion of the dominant shoulder was less than that of the nondominant shoulder by more than 5°. Elbow ROM measurements were used to establish norms for the players and served as a baseline. Elbow intervention strategies were initiated if the ROM deficit was greater than 10° and symptoms were suspected to correlate with the ROM loss. If pitchers exhibited any of these criteria, then a structured stretching and modality program was initiated. The intervention used for each ROM deficit is described in Table 1.
Strategies Used to Improve or Maintain Shoulder Range of Motion a

a ART, active release techniques; DMS, deep muscle stimulator; IASTM, instrument assisted soft tissue mobilization; IR, internal rotation; TROM, total range of motion.
Statistical Analysis
Where appropriate, results are reported by descriptive statistics such as number, mean ± standard deviation, range, and median. Pairwise comparisons between normally distributed continuous variables (ie, mean pre- vs postseason ROM) were performed via Student t test. These results are reported with mean differences (MDs), 95% CIs, and corresponding P values. To assess the relationship of shoulder and elbow motion to workload, Pearson correlation coefficients were calculated for each relationship. These results are reported with their corresponding R and P values. For all comparisons, P < .05 was considered to represent statisticaly significant differences.
Results
Overall Demographics
A total of 92 pitchers met the inclusion criteria and had pre- and postseason IR, ER, GIRD, and TROM measurements; 87 pitchers had pre- and postseason HA measurements, whereas 64 pitchers had pre- and postseason FF measurements. Elbow ROM was measured in 86 pitchers. The mean demographic data were as follows: age 28.3 ± 5.0 years, height 189.3 ± 5.7 cm, weight 97.1 ± 10.5 kg, and BMI 27.1 ± 3.0. Additional demographic data are provided in Table 2. Pitchers threw an average of 1318 ± 947 pitches and 102 ± 56 innings over the course of the season. Mean fastball velocity was 91.9 ± 2.9 mph (range, 83-97.9 mph) (Table 2).
Basic Demographics and Measures of Workload for Pitchers

Changes in Shoulder and Elbow ROM Over the Course of the Season
Assessment of the change of ROM over the course of the season in pitchers showed that dominant shoulder ER increased 6.6°, from 118.8° to 125.4° (MD, 6.6; 95% CI, 3.83°-9.37°; P < .001). A corresponding increase was found in TROM, from 173.1° to 181.7° (MD, 8.6°; 95% CI, 4.48°-12.72°; P < .001) as shoulder IR did not significantly change. HA also improved significantly, from 97.3° to 113.0° (MD, 15.7°; 95% CI, 12.73°-18.67°; P < .001) (Table 3). Significant differences in elbow flexion, extension, or TROM were not observed (Table 3).
Changes in Shoulder and Elbow Range of Motion Over the Course of the Season for Professional Baseball Players a
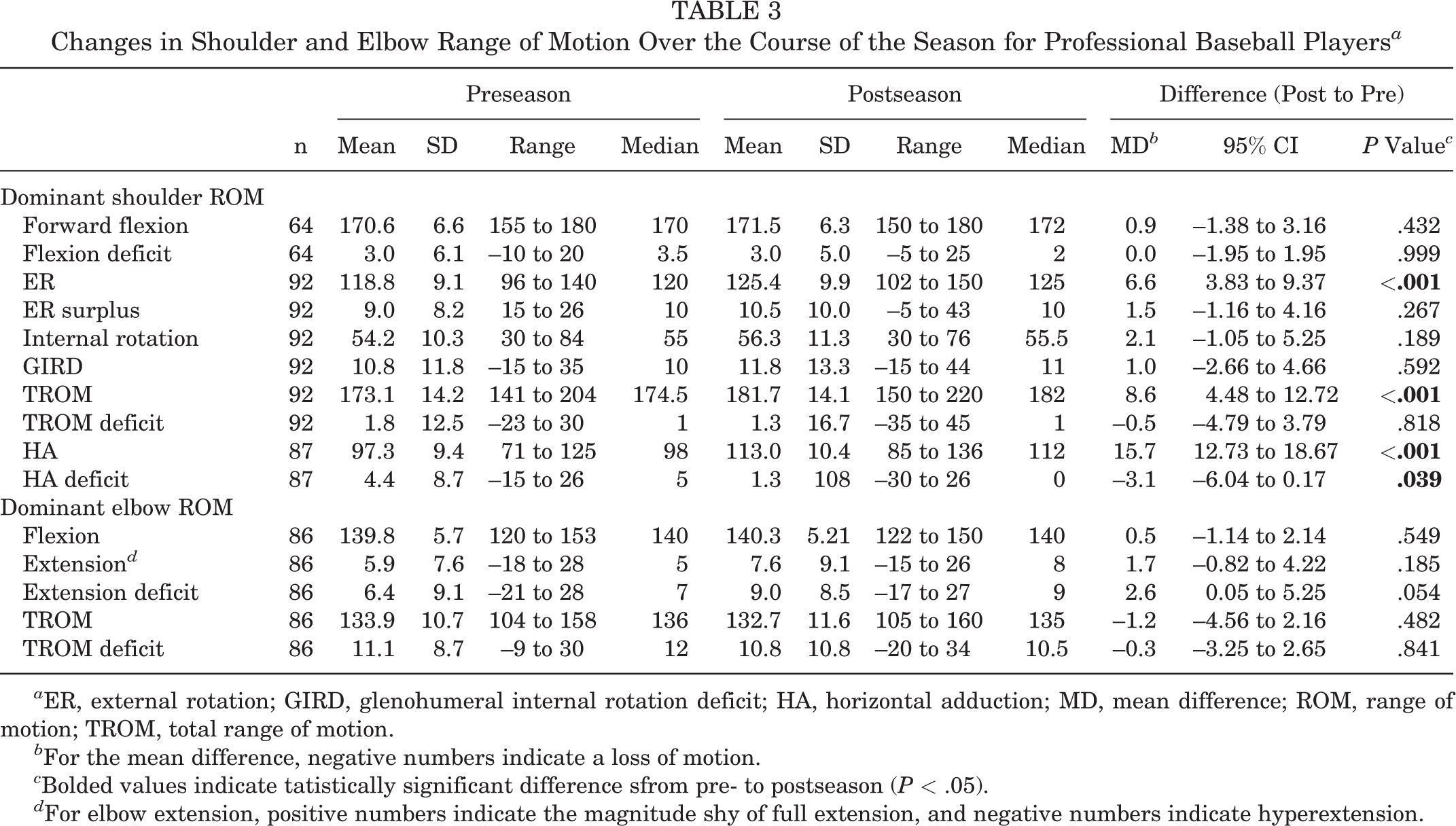
a ER, external rotation; GIRD, glenohumeral internal rotation deficit; HA, horizontal adduction; MD, mean difference; ROM, range of motion; TROM, total range of motion.
b For the mean difference, negative numbers indicate a loss of motion.
c Bolded values indicate tatistically significant difference sfrom pre- to postseason (P < .05).
d For elbow extension, positive numbers indicate the magnitude shy of full extension, and negative numbers indicate hyperextension.
Relationship of Changes in Shoulder and Elbow ROM to Workload
For the pitchers, no significant correlations were found between any of the demographic parameters studied (age, height, weight, and BMI) and change in shoulder or elbow ROM. No significant correlations were found between any of the studied measures of workload and ROM change (P > .05 for all) (Table 4). More specifically, more pitches thrown or innings pitched did not correlate with a loss of shoulder or elbow ROM over a season. Furthermore, throwing fewer pitches or innings did not translate into increased ROM.
Correlation Coefficients Between Pitcher Demographics/Workload and Change in Range of Motion a
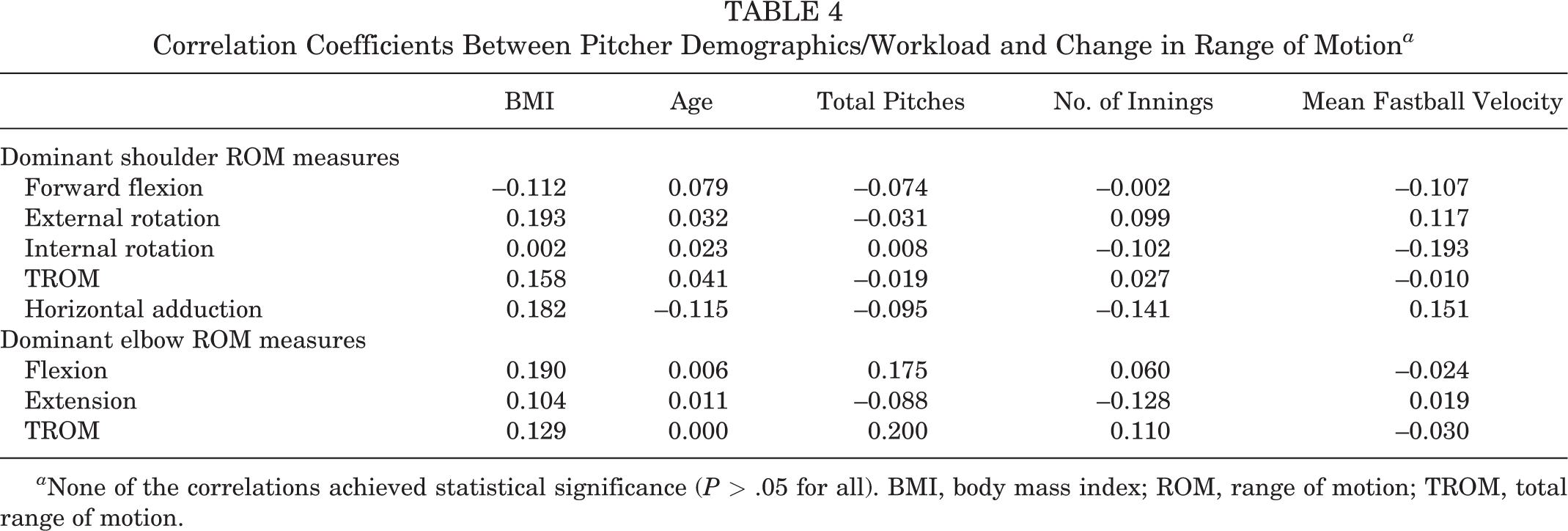
a None of the correlations achieved statistical significance (P > .05 for all). BMI, body mass index; ROM, range of motion; TROM, total range of motion.
Data on intervention strategies beyond normal maintenance were not available.
Discussion
Shoulder and elbow ROM deficits have been shown to correlate with shoulder and elbow injury in baseball players. 2,13,16,19 –21 However, shoulder and elbow ROM changes in pitchers over a baseball season are still poorly understood. 5,23 Accordingly, the purpose of this study was to investigate such in MLB pitchers from pre- to postseason and determine whether these changes were associated with measures of pitching workload during the season. No changes in elbow flexion, extension, or TROM were identified in this study. However, pitchers gained a total of 6.6° of shoulder ER and 8.6° of shoulder TROM between the beginning and end of the season. They also increased shoulder HA by an average of 15.7°, while GIRD remained unchanged. Measures of workload or player demographic data were not significantly associated with the changes in ROM in this cohort of pitchers.
Our study results are similar to those of a study performed over a shorter season in collegiate baseball pitchers (typically there are 60 games in college baseball versus 162 in MLB). 5 Dwelly et al 5 evaluated the changes in ROM over a season in 48 National Collegiate Athletic Association (NCAA) Division I and II pitchers and reported gains in ER and TROM in both shoulders. No change in GIRD was documented. This may suggest that pitchers are at greater risk of shoulder and elbow injury early during the season and spring training before full TROM is achieved. Accordingly, consideration could be given to reducing workload until symmetric ROM profiles are achieved or instituting an off-season stretching program to optimize ROM profiles earlier in the season. The observed gains in ER and TROM over the season in the current study may be due to several factors. Perhaps pitchers actually lose their ideal ROM during the offseason and regain motion over spring training though stretching and throwing protocols. Alternatively, perhaps a structured stretching and modalities program (see Table 1) aimed at early identification of players with decreased ROM can effectively improve the ROM of pitchers throughout a baseball season. More studies are required to assess the change in ROM from the end of a season to the start of spring training as well as to evaluate intervention strategies that may help increase and maintain ROM.
Our data differ from the findings of other studies in the literature. 7,15,19 A study of MLB pitchers demonstrated no significant differences overall in shoulder ROM over a season. However, starting pitchers demonstrated significantly increased IR and TROM compared with relief pitchers. 7 Another study examined 33 asymptomatic professional pitchers over 2 spring trainings and reported increased IR and decreased HA in the dominant shoulder, while nondominant shoulder ROM remained the same. 15 The differences in ROM seen between these different cohorts of pitchers may be due to several factors. Differences in levels of competition, demographics, ROM measurement and stabilization techniques, and timing of data collection (eg, preseason to postseason, preseason to preseason, immediately after pitching) may have implications on the ROM data collected. Furthermore, all of the studies had relatively small sample sizes compared with this study.
The implication of workload and its influence on injury risk has been extensively discussed in the literature. 11,12,22,26 The relationship between parameters of workload and ROM over a baseball season has been studied in the hip in collegiate baseball players but, to our knowledge, has not been examined in the shoulder or elbow. This study did not demonstrate a correlation between innings pitched, total number of pitches thrown, or mean fastball velocity and ROM changes over a season. These findings are similar to those of Zeppieri et al, 26 who examined the hips of collegiate pitchers. These investigators demonstrated a decrease in trail and lead hip ER, trail and lead hip total rotational ROM, and trail and lead hip abduction strength over a baseball season, but these changes did not correlate with measures of pitching workload. Reinold et al 15 reported a decrease in shoulder IR, TROM, and elbow extension immediately after pitching that persisted over 24 hours. The findings in our study suggest that these motion deficits are recoverable.
Several limitations of the current study merit discussion. Although this study had a greater number of participants compared with previous studies, the sample size was still relatively small and may have been underpowered to detect small relationships between workload and motion changes. Additionally, the true workload of professional baseball players is very difficult to measure precisely. The measures examined in this study only approximate the true workload of the pitcher. For example, pitchers generally throw differing numbers of bullpen sessions and differing numbers of warm-up pitches depending on whether they are starting pitchers or relief pitchers. Potential confounding variables, including history of prior shoulder or elbow injury or surgery as well as interventions beyond normal maintenance, were not accounted for because these data were not available. Similarly, our study was not able to account for any pitches thrown outside of an MLB game. Individual pitching mechanics of the athlete likely contribute to workload experienced for each throw, inning, or game. Interrater reliability was not assessed for the methods used to quantify shoulder and elbow ROM, as this was not logistically practical in the setting of pre- and postseason player examinations. To overcome this, we took a number of steps to maximize accuracy and reliability of the measures, such as using previously validated measurement techniques, 25 involving 2 examiners (one to position the limb and the other to make the measurement), using the same 2 examiners for all measures, and video recording all measurements to ensure maintenance of proper technique.
Conclusion
Significant increases in dominant shoulder ER, TROM, and HA were found from the beginning to end of a baseball season in this cohort of MLB pitchers. Because pitchers with restricted ROM profiles early in the season may be at increased risk for injury, a structured intervention program implemented early in the season may help to achieve these gains in motion. Observed changes in dominant shoulder ROM over the course of a season were not correlated with measures of pitching workload. Further studies using more accurate measures of workload may be warranted.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.H.M. has received educational support from Arthrex, fellowship support from Smith & Nephew, and hospitality payments from Encore Medical and Arthrex. D.W. has received fellowship support from Smith & Nephew. C.L.C. has received educational support from Arthrex and Zimmer Biomet, fellowship support from Smith & Nephew, and hospitality payments from Arthrex and Stryker. J.S.D. has received nonconsulting compensation from Arthrex; is a consultant for Arthrex, Trice Medical, Merck Sharp and Dohme, DePuy, Wright Medical, and Linvatec; receives royalties from Linvatec; and has received hospitality payments from Arthrex and Horizon Pharma. S.H.C. has received nonconsulting compensation from Smith & Nephew and is a consultant for Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Mayo Clinic Institutional Review Board.