
Abstract
Background:
Arthroscopic posterior shoulder stabilization can be performed with patients in the beach-chair (BC) and the lateral decubitus (LD) positions; however, the impact of patient positioning on clinical outcomes has not been evaluated.
Purpose:
To compare clinical outcomes and recurrence rates after arthroscopic posterior shoulder stabilization performed in the BC and LD positions.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review using PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines was performed by searching PubMed, Embase, and the Cochrane Library for studies reporting the clinical outcomes of patients undergoing arthroscopic posterior shoulder stabilization in either the BC or LD position. All English-language studies from 1990 to 2017 reporting clinical outcomes after arthroscopic posterior shoulder stabilization with a minimum 2-year follow-up were reviewed by 2 independent reviewers. Data on the recurrent instability rate, return to activity or sport, range of motion, and patient-reported outcome scores were collected. Study methodological quality was evaluated using the Modified Coleman Methodology Score (MCMS) and Quality Appraisal Tool (QAT).
Results:
A total of 15 studies (11 LD, 4 BC) with 731 shoulders met the inclusion criteria, including 626 shoulders in the LD position (mean patient age, 23.9 ± 4.1 years; mean follow-up, 37.5 ± 10.0 months) and 105 shoulders in the BC position (mean patient age, 27.8 ± 2.2 years; mean follow-up, 37.9 ± 16.6 months). There was no significant difference in the overall mean recurrent instability rate between the LD and BC groups (4.9% ± 3.6% vs 4.4% ± 5.1%, respectively; P = .83), with similar results in a subanalysis of studies utilizing only suture anchor fixation (4.9% ± 3.6% vs 3.2% ± 5.6%, respectively; P = .54). There was no significant difference in the return-to-sport rate between the BC and LD groups (96.2% ± 5.4% vs 88.6% ± 9.1%, respectively; P = .30). Range of motion and other patient-reported outcome scores were not provided consistently across studies to allow for statistical comparisons.
Conclusion:
Low rates of recurrent shoulder instability and high rates of return to sport can be achieved after arthroscopic posterior shoulder stabilization in either the LD or the BC position. Additional long-term randomized trials comparing these positions are needed to better understand the potential advantages and disadvantages of surgical positioning for posterior shoulder stabilization.
While constituting only 2% to 10% of all cases of instability, posterior instability has become increasingly recognized. 1,3 –7,20,22,25 –30,38 Posterior shoulder instability results from either repetitive microtrauma/overuse or a traumatic subluxation or dislocation injury, often from a contact sport or traumatic fall. 13,18,19,23,25,29,34 Posterior shoulder instability is most often managed via arthroscopic stabilization using suture anchors, addressing posterior capsulolabral abnormalities. 7,13,28,30 Improved clinical outcomes and high rates of return to sport have been reported in patients after arthroscopic capsulolabral repair for the treatment of posterior instability. 7
Arthroscopic posterior shoulder stabilization can be performed in the beach-chair (BC) position 2,8,11,16,36 as well as the lateral decubitus (LD) position. § With appropriate indications, both techniques typically result in low complication rates. Surgeon preference often determines which position is to be used during arthroscopic surgery. 15 The LD position is thought to provide improved visualization and instrument access to the posterior and inferior aspects of the glenoid, while the BC position is thought to provide an easier setup and to better allow the option of conversion to an open procedure if necessary. 11,15 The benefits of one position over the other for arthroscopic anterior shoulder stabilization have been debated in the literature, with a suggestion of lower recurrence rates after surgery in the LD position. 11,15 However, the potential effect of patient positioning and its relation to clinical outcomes and recurrence rates has not been evaluated for patients undergoing arthroscopic posterior shoulder stabilization.
The purpose of this study was to systematically review the clinical outcomes after arthroscopic posterior shoulder stabilization in either the BC or LD position. We hypothesized that clinical outcomes would be similar in both positions and that the recurrence rate would be decreased in the LD versus BC position.
Methods
Literature Search
The methods of this study are similar to those of a previously published article comparing the BC versus LD position for arthroscopic anterior shoulder stabilization. 15 We conducted a systematic review of publicly available evidence using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines with a PRISMA checklist. Two independent reviewers (E.A.M., D.A.H.) completed the search on September 10, 2017. The following databases were used: PubMed, Embase, and Cochrane Library. An initial search using the terms “arthroscopy,” “arthroscopic,” “shoulder,” “instability,” “beach chair,” or “lateral decubitus” yielded few results (27 total results; PubMed: 13 results, Embase: 14 results, Cochrane Library, 0 results), so the search strategy was broadened to include as many potential articles as possible for inclusion. The following terms were then searched: “arthroscopy,” “arthroscopic,” “instability,” and “posterior.”
Inclusion criteria were English-language studies from 1990 to 2017 incorporating the designated search items. Studies with levels of evidence 1, 2, 3, and 4 were included. Studies were excluded if analyzing open surgery, revision surgery, and nonisolated posterior labral tears or if they did not specify the surgical technique. Additional exclusion criteria included biomechanical studies, novel technique studies, scientific meeting abstracts/proceedings, and systematic reviews/meta-analyses. Studies that included both open and arthroscopic cases but separated their results clearly by group were allowed, with only the data from the arthroscopic cases included in this analysis. In the event of disagreement on the inclusion status of a study, the final decision was made by the senior author (R.M.F.). Fifteen studies ∥ met the inclusion and exclusion criteria (Figure 1).
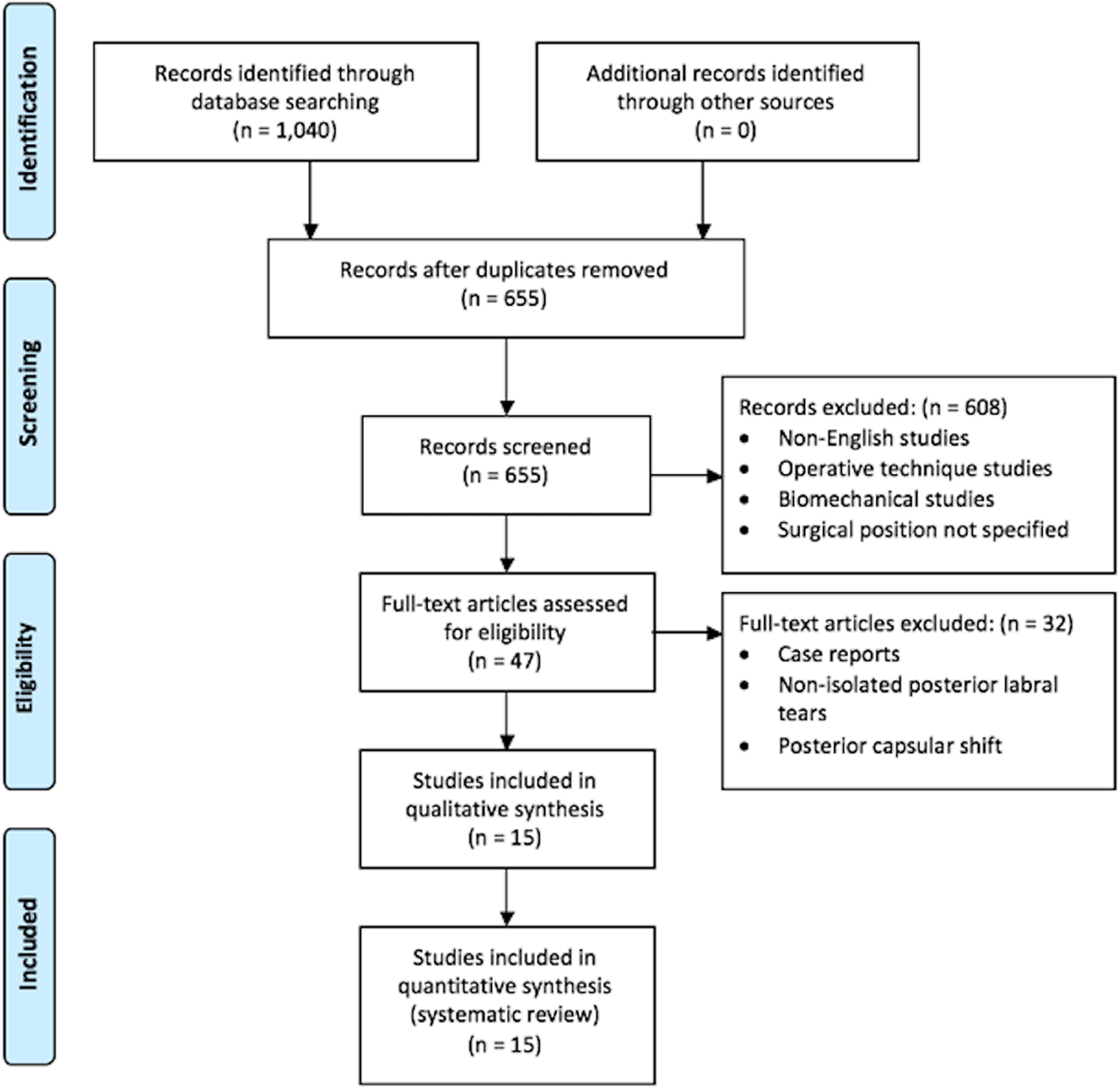
Search strategy. The authors’ electronic search strategy outlined using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Data Extraction
For the studies considered appropriate for inclusion, study data, including injury type, recurrence rates, reoperation rates, return to activity, and patient-reported outcome scores, were collected and pooled (when available).
Study Methodology Assessment
Study methodological quality was evaluated with the Modified Coleman Methodology Score (MCMS) 10 and Quality Appraisal Tool (QAT). 31 Both evaluation methods are validated tools commonly used in orthopaedic, sports medicine, and shoulder publications. 15 The MCMS is a 15-item questionnaire, with each item scored depending on the specific item in question. Scores of 85-100 are excellent, 70-84 good, 55-69 fair, and <55 poor. 10 The QAT is a 12-item questionnaire that is used to assess the quality of nonrandomized controlled trials. Each item is given a score of 0, 1, or 2, with the best possible raw score equaling 24 and with an associated assigned percentage score. 15,31
Statistical Analysis
Descriptive statistics were calculated for continuous variable data and reported as mean ± SD. A weighted mean was calculated for numerical demographic data and outcome scores based on the included studies. A chi-square test was used to determine significant differences in outcomes between the LD and BC positions.
Results
Fifteen studies, including 11 LD studies ¶ and 4 BC studies, 2,8,16,36 met inclusion criteria, with levels of evidence ranging from 2 to 4. A total of 731 shoulders were included, with 626 shoulders in the LD position (mean patient age, 23.9 ± 4.1 years; 83.9% male) and 105 shoulders in the BC position (mean patient age, 27.8 ± 2.2 years; 85.3% male). The mean patient age was significantly higher in shoulders undergoing surgery in the BC position compared with the LD position (P = .04). There were 593 shoulders available for follow-up (89.3%). The mean follow-up time was 37.5 ± 10.0 months in the LD group (range, 28-66 months) and 37.9 ± 16.6 months in the BC group (range, 28-61 months). A summary of the data from all 15 studies is presented in Table 1, and specific data from either LD or BC studies are provided in Tables 2 and 3.
Overall Results for Entire Cohort a

a BC, beach chair; LD, lateral decubitus.
Characteristics of Included Studies a

a BC, beach chair; LD, lateral decubitus; LOE, level of evidence; MCMS, Modified Coleman Methodology Score; QAT, Quality Appraisal Tool.
Specific Results for Entire Cohort a

a Data are shown as n (%) unless otherwise indicated. Recurrence and reoperation rates exclude patients lost to follow-up. BC, beach chair; LD, lateral decubitus; NA, not available.
MCMS and QAT Scores
Of the 15 studies included, 14 were retrospective cohort studies, and 1 was a prospective cohort study. There was 1 level 2 study (LD), 7 4 level 3 studies (3 LD, 1 BD), 16,17,24,38 and 10 level 4 studies (7 LD, 3 BC). 2,3,8,20 –22,28,32,35,36 The mean MCMS of all 15 studies was 58.3 ± 21.0 (maximum score, 84), indicating fair to poor methodology. The mean QAT score was 16.1 ± 5.5 (maximum score, 22). There were no significant differences between the LD and BC studies with regard to the MCMS (64.5 ± 15.4 and 53.0 ± 7.1, respectively). Similarly, there were no significant differences between the LD and BC studies with regard to the QAT score (17.1 ± 3.8 and 17.5 ± 3.0, respectively).
Country of Origin
Of the 15 studies, 10 were published from the United States (8 LD, 3,7,22,24,28,32,35,38 2 BC 2,36 ), 2 were published from Europe (1 LD, 17 1 BC 8 ), 2 were published out of Asia (2 LD 20,21 ), and 1 was published out of South America (BC 16 ).
Surgical Technique
Suture anchors were used in all 11 of the LD studies (100%), although 1 LD study 38 did not use suture anchors in every patient. Suture anchors were used in 3 2, 8,16 of the 4 BC studies (75%), and bioabsorbable tacks were used in 1 BC study (25%). 36 The number of anchors used between the 2 groups was not statistically significant, with a mean of 2.4 ± 0.5 implants in the LD group and a mean of 1.7 ± 0.5 implants in the BC group (P = .11).
Postoperative Rehabilitation
Postoperative rehabilitation was described in 9 of the 11 LD studies # and 3 of the 4 BC studies. 2,16,36 Ten of the 12 reporting studies** enacted sling immobilization for at least 3 weeks postoperatively before introducing physical therapy (range, 3-6 weeks). One LD study 32 utilized a gunslinger brace for the first 3 weeks postoperatively, whereas another LD study 35 reported sling immobilization for only 2 weeks postoperatively. All reporting BC studies utilized sling immobilization for at least 3 weeks postoperatively.
Return to sport/full activity was described in the postoperative rehabilitation protocol in 8 of the 11 LD studies 7,20,22,24,28,32,35,38 and 2 of the 4 BC studies. 2,36 Seven LD studies 7,20,22,24,29,32,35 reported that patients were allowed to return to sport/full activity after 4 20,29,32 to 6 months 7,20,22,24,32,35 if the patient had near-normal range of motion and strength compared with the contralateral side. One LD study 38 reported that return to full activity was permitted after 3 months. One BC study 2 reported that sport-specific rehabilitation was initiated after 2 to 3 months; however, a time limit was not enforced for return to full play, and 1 BC study 36 reported that patients were allowed to return to activities as tolerated at 4 to 5 months, with contact sports being allowed after 6 months.
Recurrence and Reoperation Rates
Of the LD studies, 6 studies 3,20 –22,32,38 defined recurrence as a recurrent subluxation 3,20,21,32,38 or recurrent dislocation 32 or feelings or symptoms of instability. 3,22 Three LD studies 17,28,35 defined recurrence less clearly as “recurrence of instability.” Two LD studies 7,24 described recurrence as postoperative instability as defined by a score greater than 5 on the stability scale.
Of the BC studies, 2 studies 2,8 defined recurrence as feelings or symptoms of instability. One BC study 16 did not define recurrence clearly. One BC study 36 defined recurrence as the need for revision surgery because of a failed repair.
The mean overall recurrent instability rate was reported in all 11 of the LD studies †† and all 4 of the BC studies 2,8,16,36 (Table 3). The mean overall recurrence rates were 4.9% ± 3.6% in the LD group (range, 0.0%-12.1%) compared with 4.4% ± 5.1% in the BC group (range, 0.0%-7.7%) (P = .83). On analyzing only the studies using suture anchors (excluding the single study 36 using bioabsorbable tacks), the mean overall recurrent instability rates were 4.9% ± 3.6% in the LD group compared with 3.2% ± 5.6% in the BC group (P = .54).
For patients in the LD position, reoperations were performed for the following noted reasons: recurrent instability, gross subluxation, gross dislocation, and pain. For patients in the BC position, reoperations were performed for the following noted reasons: recurrent instability, pain, and stiffness. The time to and type of reoperation procedures were not consistently described, and therefore, no comparison can be made between groups. The mean overall reoperation rates were 1.5% ± 2.8% in the LD group (range, 0.0%-7.1%) compared with 5.2% ± 6.3% in the BC group (range, 0.0%-12.9%) (P = .13). On analyzing only the studies using suture anchors (excluding the single study 36 using bioabsorbable tacks), the mean overall reoperation rates were 1.5% ± 2.8% in the LD group compared with 4.3% ± 7.4% in the BC group (P = .30).
Postoperative Return to Sport
The percentage of patients involved in sports was reported in all LD studies, with 93.1% ± 9.5% participating in sports (range, 71.4%-100.0%), as described in Table 3. The percentage of patients involved in sports was reported in 3 of 4 BC studies, 2,8,36 with 80.5% ± 18.0% participating in sports (range, 64.5%-100.0%). The return-to-sport rates, reported in 9 LD studies 3,7,17,20 –22,24,35,38 and 2 BC studies, 2,36 were 88.6% ± 9.1% (range, 72.7%-100.0%) and 96.2% ± 5.4% (range, 92.3%-100.0%), respectively (P = .30) (Table 3). Specific details on the type of activities were not universally provided in the reporting studies.
Other Outcome Measures
Other outcomes, including duration of symptoms (3 studies), 8,20,38 the University of California, Los Angeles (UCLA) score (4 studies), 3,16,20,21 the Rowe score (3 studies), 8,20,21 preoperative and postoperative pain (3 studies), 3,7,24 the American Shoulder and Elbow Surgeons score (7 studies), 3,7,20 –22,24,28 the L’Insalata score (2 studies), 24,36 the Single Assessment Numerical Evaluation score (1 study [LD position]), 28 the Oxford score (1 study [BC position]), 2 the Western Ontario Shoulder Instability Index score (2 studies [both LD position]), 3,28 and the visual analog scale for pain (4 studies), 8,20 –22 were only available in limited studies, and therefore, neither descriptive nor qualitative statistical analyses were available for these outcomes (Table 4). Data for range of motion parameters, including forward flexion and internal or external rotation, were not provided consistently or in enough studies to make statistical comparisons.
Patient-Reported Outcomes a

a “+/–” indicates that the outcome measure was/was not administered. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numerical Evaluation; UCLA, University of California, Los Angeles; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Discussion
The principal findings of this study are as follows: (1) at a mean 37.6 months after arthroscopic posterior shoulder stabilization, patients undergoing surgery in either the LD or BC position had similar outcome scores, similar return-to-sport rates, and similar recurrence rates; and (2) the mean overall recurrent instability rates were 4.9% in the LD position and 4.4% in the BC position. Importantly, as the use of bioabsorbable tacks has historically been associated with worse outcomes as compared with suture anchors, 9,33 we chose to run 2 analyses: 1 including and 1 omitting bioabsorbable tacks. Notably, no significant differences in recurrence rates between the BC and LD groups were demonstrated when only analyzing studies using suture anchors.
Arthroscopic surgery, as compared with open surgery, is thought to be beneficial because of improved visualization and decreased surgical morbidity, resulting in decreased postoperative pain. 15 More specifically, arthroscopic treatment of posterior shoulder instability has been shown to increase function and stability of the affected shoulder, ultimately leading to good to excellent clinical outcomes and high rates of return to activity. 7,25 It is essential to recognize, however, that within the same procedure, there exists a variance in arthroscopic approaches, including variability in patient positioning. Arthroscopic posterior shoulder stabilization can be performed with patients in the LD or BC position. 22 The LD position is advantageous, as it provides complete visualization and instrument access to the posterior glenoid. However, some suggest that the BC position is superior, as it enables the option of conversion to an open procedure if necessary. 11,15 Despite this, conversion to an open procedure is much less common in posterior instability, and it did not occur in any of the studies analyzed.
Patient positioning has not been commonly analyzed as a potential factor contributing to the recurrence of shoulder instability; some literature has suggested that positioning may significantly influence outcomes for some procedures. A systematic review by Frank et al 15 of 3668 arthroscopic anterior shoulder stabilization procedures performed either in the LD or the BC position found a significantly lower recurrence rate of instability in the LD position as compared with the BC position. The present study did not determine such a difference when analyzing stabilization procedures performed for posterior instability. Notably, the causes of anterior and posterior shoulder instability are different, and the underlying abnormalities to the anterior and posterior labra are also different. It may be that the advantages offered by the LD position with respect to visualization and instrumentation are not as useful in treating posterior capsulolabral tears as they are with treating anterior capsulolabral tears. It is interesting to note that of the 731 shoulders included in this analysis, 86% (626 shoulders) were stabilized in the LD position, while only 14% (105 shoulders) were stabilized in the BC position. Thus, while the overall recurrence rates were similar, it is interesting that during the past 3 decades, the vast majority of published articles on posterior shoulder stabilization describe outcomes after surgery in the LD position, implying that surgeons more often prefer the LD position for patients with posterior shoulder instability. Additionally, increased visualization of the inferior capsule when performing arthroscopic shoulder stabilization in the LD position may be advantageous in patients with 360° labral tears. 12,37 Furthermore, surgeon familiarity with the procedure and skilled technique likely contribute significantly to positive outcomes. 15
Limitations
This systematic review is not without limitations. While 731 shoulders were included in this review, not all studies evaluated the same outcome measures, and sample sizes were therefore limited for particular outcomes. As none of the studies directly compared the effect of the LD versus BC position on outcomes, the results needed to be analyzed carefully, as factors other than patient positioning may have influenced outcomes. By decreasing the sample sizes for particular outcomes through variable outcome measures, the ability to carefully interpret the results and control for additional factors diminished. Additionally, the quality of some included studies limited our conclusions. Although it was necessary to include these studies to create the most comprehensive review possible, 5 studies were considered “poor” quality. 2,3,8,16,17 It is also necessary to recognize sources of bias present in the included studies. As a majority of the included studies were retrospective cohort studies, selection bias is a principal limitation. Additionally, the variance in outcome measures increased the presence of detection bias, and the different lengths of time to follow-up contributed to transfer bias. Furthermore, there was an imbalance between the number of LD studies and the number of BC studies. The inclusion of only 4 BC studies may have decreased the statistical power. Finally, the high heterogeneity of the included studies, definitions of failure, and population made it difficult to draw strong conclusions from the available data.
Conclusion
Low rates of shoulder instability and high rates of return to sport can be achieved after arthroscopic posterior shoulder stabilization in either the LD or the BC position. This review found that based on the best available evidence, outcomes for the LD and BC positions were comparable, with neither position proving superior. Long-term randomized controlled trials comparing the LD and BC positions are needed to sufficiently understand the impact of patient positioning on clinical outcomes. At this point, however, it is appropriate for surgeon preference and experience level to determine patient positioning during this arthroscopic procedure.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C.M. has received research support from Biomet, DePuy Mitek, Smith & Nephew, and Stryker; is a consultant for Biomet and DePuy Mitek; and receives royalties from Biomet and Elsevier. A.J.S. is a consultant for Medacta; has received educational support from Gemini Mountain Medical; has received honoraria from Encore Medical; and has received hospitality payments from Encore Medical, Gemini Mountain Medical, and Stryker. J.T.B. has received research support from Stryker; is a consultant for DJO, Encore Medical, Smith & Nephew, and Stryker; has received fellowship funding from DePuy Mitek; and receives royalties from Shukla Medical. A.F.V. is a consultant for ArthroCare and Stryker, is a paid speaker/presenter for Arthrex and Ceterix, has received educational support from Smith & Nephew, and has received hospitality payments from Steris. R.M.F. has received research support from Arthrex; has received educational support from Arthrex, Medwest, and Smith & Nephew; and has received hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.