
Abstract
Introduction:
We aimed to perform a systematic review to identify factors that may lead to poorer outcomes in arthroscopic surgery for posterior shoulder instability.
Methods:
We searched MEDLINE, Embase and the Cochrane Database of Systematic Reviews for 757 unique articles. We eventually included 22 articles. Data were analysed using Review Manager 5.3.
Results:
The presence of chondral damage was associated with poorer outcomes as reflected in a higher post-operative Quick Disabilities of theArm, Shoulder and Hand score (mean difference (MD) = 17.1; 95% confidence interval (CI) = 2.82–31.4; p = 0.02), higher WesternOntario Shoulder Instability (WOSI) index (MD = 468.0; 95% CI = 136.5–799.5; p = 0.006), lower Simple Shoulder Test score (MD = −2.40; 95% CI = −4.34 to −0.46; p = 0.02) and a lower Single Assessment Numeric Evaluation score (MD = −15.4; 95% CI = −30.6 to −0.23; p = 0.05). The presence of previous shoulder surgery was associated with poorer outcomes as depicted by a lower American Shoulder and Elbow Society (ASES) score (MD = −93.1; 95% CI = −96.9 to −89.3; p < 0.0001). The availability of workers’ compensation was associated with poorer outcomes as revealed by a lower rate of return to work (odds ratio (OR) = 0.02; 95% CI = 0.00–0.20; p = 0.0008). The presence of additional procedures while performing surgery for posterior shoulder instability was associated with poorer outcomes as reflected by lower ASES scores (MD = −6.70; 95% CI = −8.64 to −4.76; p < 0.0001), higher WOSI index (MD = 63.4; 95% CI = 33.0–93.8; p < 0.0001), lower University of California at Los Angeles (UCLA) scores (MD = −2.30; 95% CI = −2.81 to −1.79; p < 0.0001), higher pain scores (MD = 0.72; 95% CI = 0.39–1.05; p < 0.0001) and higher post-operative instability (MD = 0.80; 95% CI = 0.57–1.03; p < 0.0001).
Conclusion:
The presence of chondral damage, previous shoulder surgery, concomitant surgery and workman’s compensation was associated with poorer outcomes for arthroscopic repair of posterior shoulder instability. Further studies should be done to further validate these factors.
Introduction
Posterior instability is seen in various athletic groups such as weightlifters, baseball players, rifle shooters, football linemen and also in military personnel due to repetitive microtrauma during push-ups and bench press. 1,2,3 It is also increasingly seen in non-athletic groups such as those of older age and in certain unique groups such as wheelchair users. 4,5
Compared to anterior shoulder instability, posterior instability is relatively rare, with the incidence described to be around 2–10%. 1,6,5 Based on current literature, the outcomes with regard to the management of posterior shoulder instability are extremely varied. We believe that this may be a result of a variety of factors including the type of surgery performed as well as other factors associated with the instability itself. There are systematic reviews that assess the outcomes of arthroscopic surgery for posterior shoulder instability. 5,1,7 However, there are currently no such reviews that analyse factors that may affect the outcomes of such surgeries. As such, we aimed to perform a systematic review, based on existing literature, to analyse these factors. We hope that our findings will lead to better management of patients with posterior shoulder instability, including pre-operative decision-making and patient counselling.
Methods
A systematic review of all articles published in the English language was performed using PubMed, Embase and the Cochrane Database of Systematic Reviews. The following MeSH term was used as part of the search strategy for this review: ‘posterior’ AND (‘shoulder’ OR ‘glenoid’ OR ‘glenohumeral’ OR ‘labrum’) AND (‘instability’ OR ‘laxity’ OR ‘subluxation’ OR ‘version’) AND (‘arthroscopic’ OR ‘arthroscopy’).
All the articles with posterior instability of shoulder with arthroscopic surgery performed were included and tabulated for discussion. All the articles with other parameters like glenoid and labral factors for posterior instability were also tabulated and discussed in detail. All the articles selected had a minimum follow-up period of 2 years. For the articles describing open surgery, the outcome measures were excluded except for one article that describes the comparison of outcomes between open and arthroscopic treatment. The epidemiological factors of articles with open surgeries and other meta-analyses were also taken into consideration at various parts of the article as references. The articles in foreign language were excluded. Cadaveric and basic science studies were excluded. Case reports and studies with poor data collection techniques were also excluded.
Data analysis was conducted with Review Manager 5.3. Where papers presented raw data, unadjusted odds ratios (ORs) were calculated together with 95% confidence intervals (CIs). This was performed via Mantel-Haenszel statistics, with random effects taken into account within our analytical model. Where data from various studies could be combined, we calculated the I 2 statistic for combined studies, which quantifies the total variation among included studies, hence providing us an estimate of the heterogeneity of studies included. Where data were unable to be combined among studies, we described the findings from the studies along with their published ORs in the form of a table.
Results
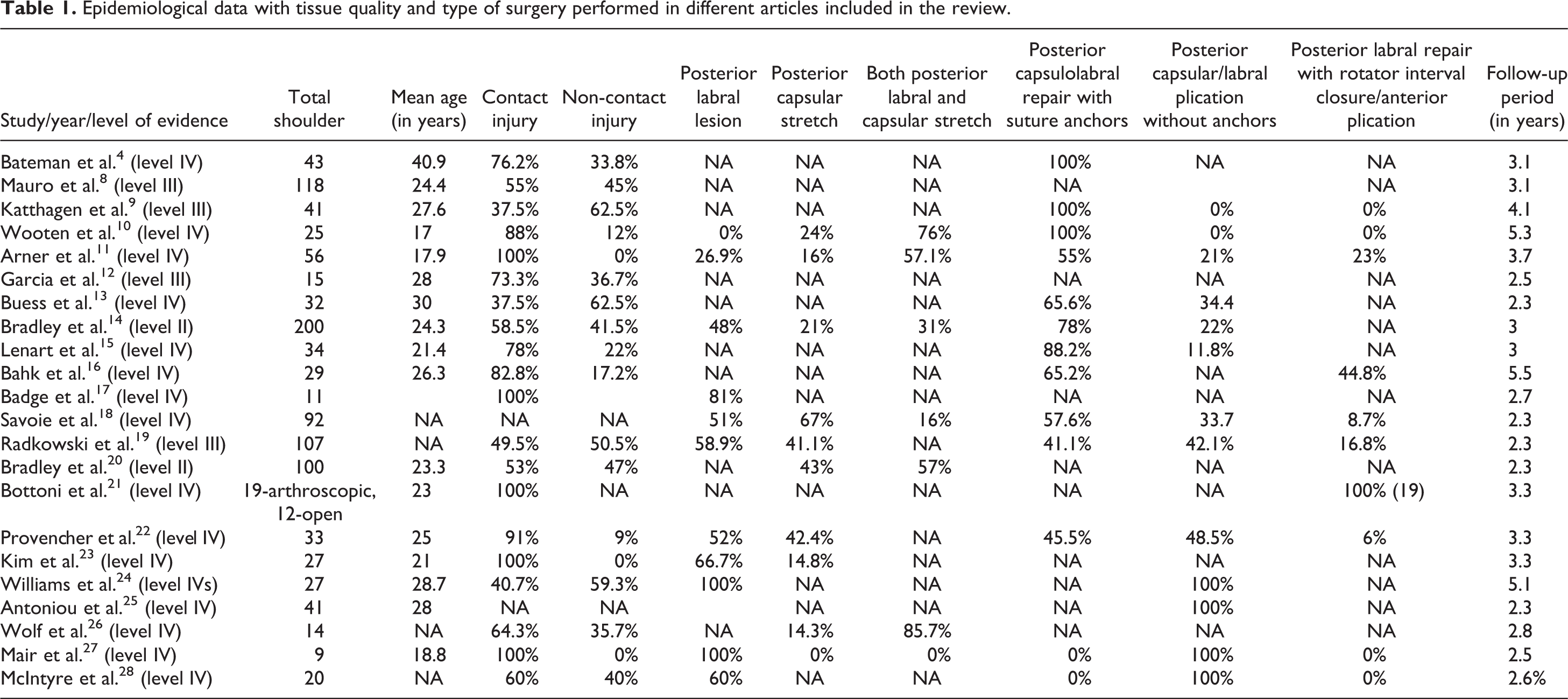
One thousand and one hundred and forty-one article titles were obtained from the three databases in total, of which 384 duplicate articles were removed. The remaining 757 studies were screened and eliminated by the authors (S.R.J. and A.A.S.) based on the exclusion criteria as described above. Eventually, a total of 42 full articles were evaluated. Twenty-two articles eventually met the inclusion criteria and were considered for review (Figure 1). There were 14 articles with level IV evidence, 5 articles with level III evidence and 3 articles with level II evidence. Further information regarding study details can be found in Table 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram summarizing the flow of selection of articles for review within this study.
Epidemiological data with tissue quality and type of surgery performed in different articles included in the review.
A large variety of underlying factors that could potentially influence arthroscopic surgical outcomes for posterior shoulder instability were studied within the included 22 studies. Unadjusted ORs were calculated for all of them. Underlying factors that were found to result in statistically significant differences in surgical outcomes for posterior shoulder instability can be found in Table 2.
Summary of results from systematic review depicting underlying factors that resulted in statistically significant differences in surgical management of posterior shoulder instability.

MD: mean difference; Quick DASH: Quick Disabilities of the Arm, Shoulder and Hand; CI: confidence interval; SST: Simple Shoulder Test; WOSI: WesternOntario Shoulder Instability; SANE: Single Assessment Numeric Evaluation; ASES: American Shoulder and Elbow Society; OR: odds ratio.
The presence of chondral damage was associated with a higher post-operative Quick Disabilities of the Arm, Shoulder and Hand (Quick DASH) score (mean difference (MD) = 17.1; 95% CI = 2.82–31.4; p = 0.02), higher Western Ontario Shoulder Instability (WOSI) index (MD = 468.0; 95% CI = 136.5–799.5; p = 0.006), lower Simple Shoulder Test (SST) score (MD = −2.40; 95% CI = −4.34 to −0.46; p = 0.02) and a lower Single Assessment Numeric Evaluation (SANE) score (MD = −15.4; 95% CI = −30.6 to −0.23; p = 0.05).
The presence of previous shoulder surgery was associated with a lower American Shoulder and Elbow Society (ASES) score (MD = −93.1; 95% CI= −96.9 to −89.3; p < 0.0001). The availability of workers’ compensation was associated with a lower rate of return to work (OR = 0.02; 95% CI = 0.00–0.20; p = 0.0008).
The presence of additional procedures while performing surgery for posterior shoulder instability was associated with lower ASES scores (MD = −6.70; 95% CI = −8.64 to −4.76; p < 0.0001), higher WOSI index (MD = 63.4; 95% CI = 33.0–93.8; p < 0.0001), lower UCLA scores (MD = −2.30; 95% CI = −2.81 to −1.79; p < 0.0001), higher pain scores (MD = 0.72; 95% CI = 0.39–1.05; p < 0.0001) and higher post-operative instability (MD = 0.80; 95% CI = 0.57–1.03; p < 0.0001).
Discussion
Based on our systematic review, there were three common classifications of arthroscopic procedures that have been studied with regard to posterior shoulder instability, namely, posterior labral repairs with suture anchors, posterior labral repairs with rotator interval closure and posterior capsular or labral plication without anchors (Table 1). The type of surgery that has been most commonly studied and described is posterior labral repair with suture anchors. Our review is based on collective data on all three types of surgery as current available data on each type of surgery with regard to predictive factors for outcomes are still limited.
With regard to arthroscopic surgery in general for posterior shoulder instability, however, we found that individual articles have studied, to varying extents, how various factors can influence the eventual outcome of surgery. These factors shall be discussed further below.
Posterior shoulder instability can be divided into traumatic and atraumatic types. Traumatic instability occurs when a provocative injury mechanism is involved without any previous history of instability. 9 Atraumatic instability is identified when there is no obvious provocative injury resulting in the instability that the patient experiences. Katthagen et al. 9 evaluated functional outcomes between atraumatic and traumatic onset posterior instability and found that atraumatic posterior shoulder instability had less favourable outcomes after arthroscopic capsulolabral anchor repair as compared to traumatic onset (Table 2).
It was also found that the presence of chondral damage was associated with poorer outcomes post-operatively. This conclusion was mainly drawn from the study by Bateman et al. 4 which revealed higher Quick DASH and WOSI scores and lower SST and SANE scores among patients with chondral damage when compared to patients without chondral damage who underwent arthroscopic procedures for their posterior instability (Table 2). The presence of chondral damage is suggestive of either a more severe or prolonged form of posterior instability. Similarly, atraumatic posterior shoulder instability tends to be of a more prolonged form of instability as compared to traumatic instability. These factors of severity and chronicity may have contributed to poorer post-operative outcomes.
The presence of concomitant shoulder surgeries, while repairing a posterior shoulder instability, as well as the presence of previous shoulder surgeries were noted to be separately associated with poorer surgical outcomes post-operatively.
It is believed that the poorer outcomes in the presence of concomitant surgeries can be explained in two ways. Firstly, the fact that concomitant operations were required meant that there was more than one posterior shoulder instability pathology which required surgery in the affected shoulder. The pre-operative presence of multiple pathologies could have resulted in significantly poorer pre-operative function as compared to patients with pure posterior shoulder instability. This decreased functional baseline would have made it increasingly challenging for such patients to reach comparative post-operative functional outcomes as compared to those with pure posterior instability. As a consequence, it is expected that such patients who require concomitant shoulder procedures would have poorer post-operative outcomes. Secondly, having multiple surgeries done within the same shoulder would expectedly have resulted in increased inflammation and surgical trauma within the shoulder, hence causing increased pain post-operatively which was shown by Bahk et al. 16 This would have resulted in poorer quality-of-life scores that was shown in the same paper. This would have been especially so if there was no proper pain control and if rehabilitation was not performed appropriately.
The presence of previous surgeries also was associated with poorer post-operative outcomes. Similar to the presence of concomitant injuries, patients who had previous shoulder surgeries may already have had poorer function of their affected shoulder to begin with. Again, the poorer functional baseline would have made it challenging for them to reach comparatively similar functional outcomes as compared to their counterparts with no previous ipsilateral shoulder surgeries done.
The final association we identified with poorer outcomes of arthroscopic repair of posterior shoulder instability is the availability of workers’ compensation. In their article, Antoniou et al. 25 suggested that this was due to perceptions of success of operations being affected by the compensation status of patients. In other words, a patient with a compensation status may have the perception that the operation he or she would undergo may be less effective. Apart from that, the availability of financial compensation may decrease the incentives for patients to rehabilitate well to achieve their pre-operative function.
Limitations
This review had several limitations. Firstly, most importantly, the quality of the review is dependent on the quality of the studies being analysed. Most of the studies included were on level IV evidence, with none of them being of level I evidence. As such, all of the studies included were retrospective in nature. Secondly, the definition of posterior shoulder instability was variable in the studies included. While most of the studies were based on clinical definitions, there were some which only included those that had radiological findings suggestive of posterior shoulder instability, such as posterior labral tears. The variety of definitions would have resulted in differences in inclusion criteria, hence potentially affecting the eventual observed outcomes noted within this review. Lastly, the duration of follow-up within individual studies varied largely, potentially resulting in variances in the proportions of complications and the outcomes observed. Nevertheless, the information derived from this review still remains relevant and does throw light on certain predictive factors that may potentially influence the outcomes of arthroscopic surgery performed for posterior shoulder instability.
Conclusion
In conclusion, poorer outcomes for arthroscopic repair of posterior shoulder instability were associated with atraumatic instability, chondral damage, concomitant shoulder procedures, previous ipsilateral shoulder surgeries and workers’ compensation. Currently, there is still a dearth of high-quality evidence with respect to this area of study. More studies should hence be performed to further validate our findings and to identify other predictive factors associated with poorer outcomes in the arthroscopic surgical treatment of posterior shoulder instability. We believe that identifying such factors will lead to better pre-operative decision-making, counselling and management of patients with posterior shoulder instability.
Footnotes
Author contributions
SR Jain and HC Tan were involved in the conception and design of the study. SR Jain and AA Sayampanathan were involved in the collection and assembly of data. SR Jain and AA Sayampanathan were involved in data analysis and interpretation. All authors were involved in the writing, editing and final approval of the manuscript.
Authors’ note
For further information regarding the data presented within this study, kindly contact AASayampanathan for further details at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.