
Abstract
Background:
To date, no studies have analyzed the influence on clinical outcomes of the interval between an anterior cruciate ligament (ACL) injury and double-bundle (DB) reconstruction with hamstring tendon autografts.
Hypotheses:
(1) Performing ACL reconstruction sooner after an injury will reduce postoperative anterior and rotatory knee instability, (2) postoperative range of knee motion or functional results will not be affected by different intervals between injury and surgery, and (3) preoperative isokinetic peak torque of the quadriceps and hamstring muscles will be lower in patients undergoing surgery earlier, while postoperative muscle strength will not be affected by surgery timing.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study was conducted on a total of 171 patients who had undergone anatomic DB ACL reconstruction with hamstring tendon autografts. The patients were divided into 3 groups based on the time to surgery: (1) ≤1 month after the injury (group E; n = 25), (2) between 1 and 3 months after the injury (group M; n = 72), and (3) >3 months after the injury (group D; n = 74). Patients were assessed for a minimum of 2 years after surgery.
Results:
Concerning postoperative anterior laxity, 1-way analysis of variance demonstrated a significant difference (P = .0274) among the 3 groups. Anterior laxity was significantly less in group E than in group D (P = .0206). Spearman rank correlation analysis showed a significant correlation (ρ = 0.200; P = .0327) between anterior knee laxity and time to surgery. Also, a significant correlation (P = .0461) was found between the degree of the pivot-shift phenomenon and time to surgery. There were no significant differences in loss of knee extension or flexion among the 3 groups, nor were there any differences in the Lysholm knee score or International Knee Documentation Committee grade. Postoperatively, there were no significant differences in peak torque of the quadriceps or hamstring muscles among the 3 groups.
Conclusion:
Early DB reconstruction led to significantly less anterior laxity compared with delayed reconstruction. There were no significant differences in postoperative range of knee motion or functional results among the 3 time intervals between injury and surgery in this study.
An anterior cruciate ligament (ACL) injury is mostly caused by sports, and the most common treatment option for a young athlete with a complete ACL tear is surgical ACL reconstruction. 5,9,47 However, the interval between the ACL tear and reconstruction, that is, the timing of reconstruction after an ACL injury, has been debated as a significant factor that affects the clinical outcome after ACL reconstruction. In a landmark study, Shelbourne et al 43 recommended waiting at least 3 weeks from the time of injury before performing single-bundle (SB) ACL reconstruction with a bone–patellar tendon–bone (BPTB) graft because the risk of arthrofibrosis increased with ACL reconstruction that was carried out within the initial 3 weeks after an injury, resulting in poor clinical results. This recommendation was corroborated by several clinical studies. 17,36,42,48 However, many studies have since reported that no loss of range of knee motion was found with ACL reconstruction performed proximate to the injury. 4,18,22,34,35 Thus, there have been some controversies in the previous studies concerning SB ACL reconstruction with an autogenous BPTB graft.
The hamstring tendon autograft has also been widely used for ACL reconstruction. Regarding the influence of the timing of ACL reconstruction with a hamstring tendon graft after ACL injuries on clinical results, Bottoni et al 6 reported that there were no significant differences between the early (range, 2-17 days) and delayed (range, 42-192 days) reconstruction groups in extension or flexion loss relative to the nonoperative side, operative time, side-to-side difference in anterior laxity, or subjective knee evaluation findings. On the other hand, Sgaglione et al 41 reported that in SB reconstruction using the hamstring tendon, patients undergoing surgery at an earlier time were noted to have a significantly better outcome compared with those after delayed reconstruction, although the range of knee motion was significantly less in the early reconstruction group. In 2018, a meta-analysis concluded that early reconstruction resulted in comparable clinical and stability outcomes compared with delayed ACL reconstruction. 31 Thus, considering the optimal surgical timing for SB ACL reconstruction, there has been no significant difference in clinical outcomes between early and delayed reconstruction. 3
Arthroscopic anatomic double-bundle (DB) ACL reconstruction using autogenous hamstring tendons has attracted notice since the first report on clinical outcomes was reported in 2004, 51 although the DB technique has never demonstrated a great deal of difference compared to standard ACL reconstruction. A number of clinical studies have analyzed risk factors that influence the postoperative outcome after DB reconstruction. 19,28,38,46 No studies, however, have been conducted to analyze the influence of the interval between the ACL injury and DB reconstruction on clinical outcomes. Thus, the optimal surgical timing of DB reconstruction with autogenous hamstring tendons remains unclear.
We conducted a retrospective case-control study to clarify the influence on clinical outcomes of the timing of anatomic DB ACL reconstruction using hamstring tendon autografts. We divided the patients according to the period in which reconstruction was performed after the injury and then compared the groups concerning postoperative anterior and rotatory laxity, range of knee motion, the Lysholm score, the International Knee Documentation Committee (IKDC) grade, and muscle strength. Based on our clinical experience and the results of previous studies in the literature, we formed the following 3 hypotheses: (1) performing ACL reconstruction sooner after an injury will reduce postoperative anterior and rotatory knee instability; (2) postoperative range of knee motion or functional results will not be affected by the interval between injury and surgery; (3) concerning the strength of the quadriceps and hamstring muscles, preoperative isokinetic peak torque will be significantly lower in the patients who underwent early reconstruction compared with those who underwent delayed reconstruction, while there will be no significant differences in postoperative muscle strength among the 3 groups.
Methods
Study Design
A retrospective case-control study was conducted at Hokkaido University Hospital and Yagi Orthopaedic Hospital with data from 208 patients who had undergone anatomic DB ACL reconstruction with hamstring tendon autografts for unilateral ACL injuries between 2012 and 2015 and who were evaluated for ≥2 years after surgery. Two senior orthopaedic surgeons (K.Y. and E.K.), who were sufficiently trained concerning this surgery, performed all operative procedures using the same protocol. Intraoperatively, concomitant meniscal tears and chondral injuries were observed and recorded by each surgeon at the time of ACL reconstruction. After surgery, all patients underwent postoperative management using the same rehabilitation protocol, as reported previously. 26,52 To test the study hypotheses, we divided the patients into 3 groups: (1) group E, in which surgery was performed within 1 month (30 days) after the injury; (2) group M, in which surgery was carried out between 1 (31 days) and 3 months (90 days) after the injury; and (3) group D, in which surgery was performed at >3 months (91 days) after the injury. Then, the preoperative background factors and postoperative clinical results were statistically compared among the 3 groups. This retrospective study design using patient data was approved by the institutional review board of our hospital.
Patient Characteristics
All 208 initial study patients had sustained a unilateral ACL injury. The diagnosis of injured ligaments was made based on a detailed history of the knee injury, a physical examination on the pathological status and abnormal laxity, routinely performed plain radiographs and magnetic resonance imaging scans, and findings at surgery. Patients with a combined injury of the posterior cruciate ligament, the lateral collateral ligament, the posterolateral (PL) corner structures of the knee, and the medial collateral ligament (grades II and III) were excluded from this study. In addition, patients with any previous surgery for ligament injuries, a concurrent fracture, or osteoarthritis were also excluded. Some patients (n = 5 [16%] in group E, n = 16 [18%] in group M, and n = 16 [18%] in group D) were excluded because they were lost to follow-up. There were 2 patients (1 from group M and 1 from group D) who showed a recurrence of instability of the knee after a reinjury and underwent revision surgery. These patients were excluded from the analysis. No postoperative surgical site infection was observed in this study.
Ultimately, 171 patients (99 men and 72 women), with a mean age of 27.2 years (range, 13-71 years), were registered for evaluations (Figure 1). In groups E, M, and D, there were 25, 72, and 74 patients, respectively, who underwent reconstruction at a mean of 0.8, 1.9, and 8.0 months after the injury, respectively (Table 1). The follow-up period ranged from 24 to 78 months, with a mean of 31.6 months. Among the 3 groups, there were no significant differences in sex, age, body mass index, or the general joint hypermobility score assessed according to the criteria of Carter and Wilkinson 10 (Table 1).

Study design and follow-up examinations. ACL, anterior cruciate ligament.
Preoperative Characteristics of Patients a

a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate statistical significance (P < .05).
b One-way analysis of variance.
c Chi-square test.
d According to the criteria of Carter and Wilkinson. 10
Concomitant medial meniscal injuries were found in 16.0%, 6.9%, and 24.3% of groups E, M, and D, respectively, and concomitant lateral meniscal injuries were found in 36.0%, 23.6%, and 27.0% (Table 1). According to our policy for meniscal injuries, an unstable longitudinal meniscal tear in the red zone was repaired, while a meniscal tear in the white zone was resected. In addition, we did not repair a red zone tear if it was too degenerated. Subsequently, the repair rate of medial meniscal injuries was 75.0%, 80.0%, and 27.8% in groups E, M, and D, respectively, while the repair rate of lateral meniscal injuries was 22.2%, 29.4%, and 35.0% (Table 1).
Concomitant articular cartilage injuries were observed in 4.0%, 4.2%, and 13.5% of groups E, M, and D, respectively, in the medial compartment and in 4.0%, 4.2%, and 2.8%, in the lateral compartment (Table 1). All the cartilage injuries were evaluated as grade I or II according to the International Cartilage Research Society classification. 8 The basic policy for a chondral injury was that this lesion was treated nonoperatively. Therefore, no surgical treatments were applied to the chondral lesions in the present study.
Surgical Procedure
The details of the DB ACL procedure have been previously described. 51,52 Briefly, a tibial tunnel for the PL bundle was created using a hole-in-one guide (Wire-navigator; Smith & Nephew). Then, a guide wire for anteromedial (AM) bundle reconstruction was inserted in the same manner. The 2 tibial tunnels were made with a cannulated drill corresponding to the measured diameter of the prepared substitute. To create 2 femoral tunnels for the AM and PL bundles, first, a guide wire was drilled at the center of the femoral attachment of the AM bundle through the AM tibial tunnel by using an offset guide (Transtibial Femoral ACL Drill Guide; Arthrex). A guide wire was inserted at the center of the PL bundle attachment on the femur through the PL tibial tunnel. Finally, 2 sockets were created for the AM and PL bundles, respectively, with cannulated drills. The locations of the tunnels have previously been reported. 26,29
For graft preparation, the harvested semitendinosus tendon was cut in half and doubled over. A commercially available polyester tape (Leeds-Keio Artificial Ligament; Neoligaments) was mechanically connected at an unlooped end of the doubled tendon by using a previously reported technique. 51,52 An Endobutton CL BTB (Smith & Nephew) was attached at the looped end (Figure 2A). 28 Finally, the graft for the PL bundle (5.5- to 6-mm diameter) was introduced through the tibial tunnel to the femoral tunnel by using a passing pin. The Endobutton was flipped on the femoral cortical surface. Then, the graft for the AM bundle (6- to 7-mm diameter) was placed in the same manner (Figure 2B). For graft fixation, an assistant surgeon simultaneously applied tension of 30 N to each graft using 2 tensiometers (Meira) at 10° of knee flexion for 2 minutes according to biomechanical and clinical studies. 23,26 –29,50 Then, a surgeon simultaneously secured the 2 tape portions onto the tibia using 2 spiked staples (Smith & Nephew) in a turnbuckle fashion.

(A) The hamstring tendon autografts (anteromedial [AM] and posterolateral [PL] bundles) were connected in a series with polyester tape and Endobuttons for double-bundle reconstruction. (B) There were 2 grafts transplanted across the knee joint at the time of surgery at 90° of knee flexion in the arthroscopic view by using the lateral infrapatellar portal.
Postoperative Management
Postoperative management was performed according to an original rehabilitation protocol. 55 Based on the results of previous biomechanical studies, we encouraged quadriceps and hamstring muscle training immediately after surgery. 54 The static squat exercise was started 1 week postoperatively. A postoperative immobilizer was applied for 2 weeks after surgery. Full weightbearing with a hinged brace was then allowed 2 weeks after surgery. Several types of athletic training were gradually allowed after 6 weeks, although no running was allowed until 6 months after surgery. Return to full sports activity was generally permitted at 9 months after surgery.
Clinical Evaluations
Each patient underwent clinical examinations at 2 years after surgery. The side-to-side difference in anterior laxity was measured with a KT-2000 arthrometer (Medmetric) at 30° of knee flexion under an anterior drawer force of 133 N, although Goodwillie et al 16 found that the side-to-side difference may play less of a role in clinical outcomes. A well-trained physical therapist and a surgeon, who were blinded to the surgical timing, collected the KT-2000 arthrometer results postoperatively. Moreover, 2 well-trained orthopaedic surgeons performed the pivot-shift test, the results of which were subjectively evaluated by the examiners. 26 For the pivot-shift test, the result of “2+” was defined as when the examiner felt a sudden rotational slip movement between the tibia and femur, a so-called jog, during the test for the injured knee. The 2+ pivot-shift result indicated an obvious failure of ACL function. The result of “+” was defined as when the examiner felt some difference in the rotational movement during the test between the injured and uninjured knees but did not obviously feel a sudden rotational slip movement. This result indicated some insufficiency of ACL function but did not indicate complete failure of the ACL.
As to the overall evaluation, the Lysholm knee score (maximum score, 100 points) and the IKDC knee examination form were used. Isokinetic peak torque of the quadriceps and hamstring tendons was measured at 60 deg/s of angular velocity using a Cybex II dynamometer (Lumex) in both knees before and 2 years after surgery. Peak torque as measured postoperatively in the reconstructed knee was represented as a ratio (percentage) of the injured to uninjured knee.
Statistical Analysis
An a priori power analysis was performed. In a study by Sgaglione et al, 41 the difference between early and delayed surgery in the KT-1000 arthrometer measurement was 27%, with 22 and 28 knees in the early and delayed groups, respectively. Based on this result, a sample size of 23 was calculated to have 95% power to test our hypotheses. Moreover, intraobserver variability for the KT-2000 arthrometer measurements and pivot-shift test was satisfactory (mean intraclass correlation coefficient, 0.72 [range, 0.62-0.79] and 0.86 [range, 0.81-0.90], respectively). Statistical analyses were conducted using 1-way analysis of variance (ANOVA) along with the post hoc Tukey-Kramer test, chi-square test, and Spearman rank correlation analysis. The significance level was set at P = .05. A commercially available software program, JMP 11 (SAS Institute), was used for statistical calculations.
Results
Anterior Knee Laxity
The preoperative side-to-side difference in anterior knee laxity averaged 3.7 ± 2.6, 3.4 ± 3.2, and 4.6 ± 2.8 mm in groups E, M, and D, respectively, with no significant differences among the 3 groups on 1-way ANOVA. On the other hand, the postoperative side-to-side difference in anterior knee laxity averaged 0.6, 1.2, and 1.5 mm in groups E, M, and D, respectively, demonstrating a significant difference (P = .0274, 1-way ANOVA) among the 3 groups (Table 2). The post hoc test showed that anterior laxity was significantly less (P = .0206) in group E than in group D (Table 2). In addition, Spearman rank correlation analysis showed a significant correlation (ρ = 0.200; P = .0327) between the side-to-side difference in anterior knee laxity and the timing of ACL reconstruction (Figure 3). Namely, the earlier that ACL reconstruction was performed, the better anterior laxity was.

Spearman rank correlation analysis showed a significant correlation between the side-to-side difference in anterior knee laxity and the 3 groups (ρ = 0.200; P = .0327).
Postoperative Side-to-Side Difference in Anterior Knee Laxity and Pivot-Shift Test Results a
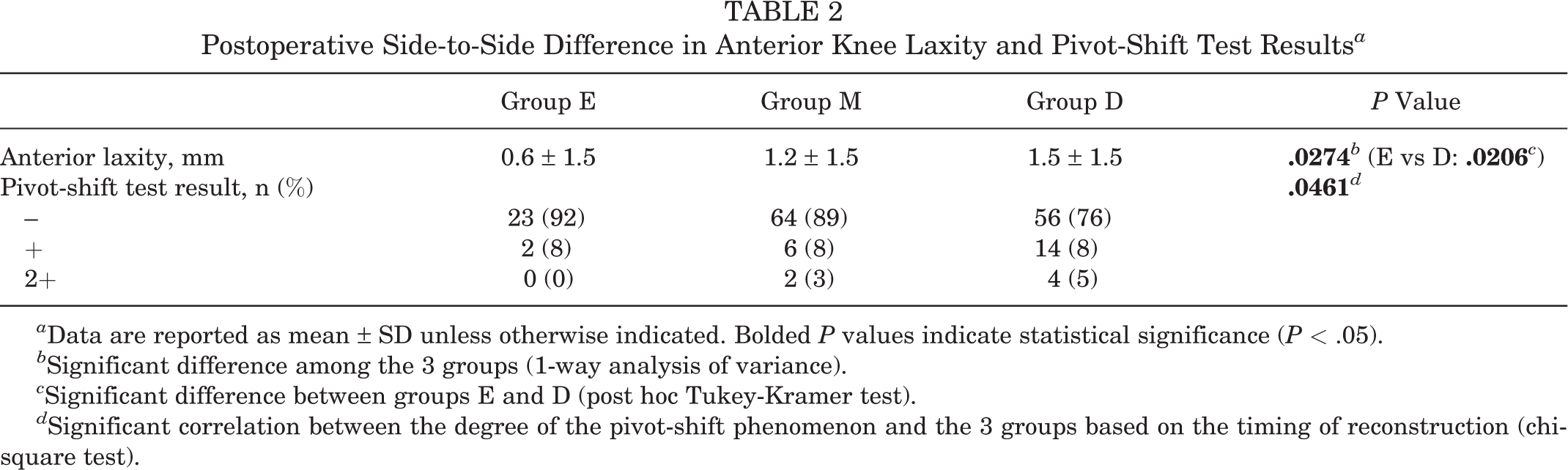
a Data are reported as mean ± SD unless otherwise indicated. Bolded P values indicate statistical significance (P < .05).
b Significant difference among the 3 groups (1-way analysis of variance).
c Significant difference between groups E and D (post hoc Tukey-Kramer test).
d Significant correlation between the degree of the pivot-shift phenomenon and the 3 groups based on the timing of reconstruction (chi-square test).
Pivot-Shift Test Results
Regarding the preoperative pivot-shift test, 7 and 18 patients were rated as + and 2+, respectively, in group E; 15 and 57 patients were rated as + and 2+, respectively, in group M; and 18 and 56 patients were rated as + and 2+, respectively, in group D. The chi-square test showed no significant difference among the 3 groups. On the other hand, results of the postoperative pivot-shift test are shown in Table 2. The chi-square test demonstrated a significant correlation (P = .0461) between the degree of the pivot-shift phenomenon and the timing of ACL reconstruction. Namely, the earlier that ACL reconstruction was performed, the better the pivot-shift test result was.
Postoperative Knee Motion and Functional Results
Loss of knee extension greater than 5° occurred in 8.0%, 5.6%, and 4.1% in groups E, M, and D, respectively. Loss of knee flexion greater than 15° was found in 4.0%, 0.0%, and 4.1% in groups E, M, and D, respectively. There were no significant differences in the loss of knee extension or flexion among the 3 groups (Table 3).
Clinical Outcomes at 2 Years Postoperatively a

a Data are reported as n (%) unless otherwise indicated. IKDC, International Knee Documentation Committee.
b One-way analysis of variance.
c A = normal; B = nearly normal; C = abnormal; D = severely abnormal.
Concerning the postoperative functional results, there were no significant differences among the 3 groups on the Lysholm score or IKDC grading (Table 3).
Quadriceps and Hamstring Muscle Strength
Preoperatively, 1-way ANOVA showed that there were significant differences in peak torque of the quadriceps (P = .0277) and hamstring (P = .0069) muscles among the 3 groups (Table 4). The post hoc test showed that peak torque of the quadriceps muscle in group D was significantly greater (P = .0380) than that in group M and that peak torque of the hamstring muscle in group D was significantly greater than that in groups E (P = .0481) and M (P = .0142) (Table 4). At 2 years after surgery, however, ANOVA showed that there were no significant differences in peak torque of the quadriceps or hamstring muscles among the 3 groups.
Isokinetic Peak Torque a

a Data are reported as mean ± SD. Peak torque was calculated as a ratio of the injured to uninjured knee. Bolded P values indicate statistical significance (P < .05).
b One-way analysis of variance.
c Post hoc Tukey-Kramer test.
Discussion
The present study tested 3 hypotheses concerning the influence on clinical outcomes of the timing of anatomic DB ACL reconstruction with hamstring tendon autografts. First, ANOVA demonstrated a significant difference in postoperative anterior laxity among the 3 groups. Anterior laxity in group E was significantly less than that in group D. In addition, there were significant correlations between postoperative anterior knee laxity, as well as the results of the pivot-shift test, and the timing of ACL reconstruction . These results confirmed our first hypothesis that the earlier DB ACL reconstruction was performed after the injury, the less postoperative anterior and rotatory knee instability there would be. Second, there were no significant differences in the loss of knee extension or flexion among the 3 groups, nor were there differences in the postoperative Lysholm score or IKDC grade, thus confirming our second hypothesis. Third, preoperative quadriceps muscle strength in group D was significantly greater than that in group M, and preoperative hamstring muscle strength in group D was significantly greater than that in groups E and M. Postoperatively, however, there were no significant differences in peak torque of the quadriceps or hamstring muscles among the 3 groups. Our third hypothesis was therefore confirmed. Thus, the present study showed that early DB reconstruction using hamstring tendon grafts improved knee stability to a significantly greater degree than delayed reconstruction, without any detrimental effect on postoperative range of knee motion. However, this improvement did not influence the functional knee score.
“Early” and “delayed” ACL reconstruction procedures have not been clearly defined to date. 6,11,13,14,21,31 A meta-analysis 31 showed that in previous clinical studies, early reconstruction was performed in the period from 9 days to 5 months after the injury, while delayed reconstruction was performed in the period from 10 weeks to 24 months. Bottoni et al 6 reported that their early reconstruction was performed in the period from 2 to 17 days after the injury. Chen et al 11 carried out their early reconstruction in the period from 3 to 7 weeks after the injury. In the present study, we divided the patients into 3 groups (within 1 month of injury, between 1 and 3 months, and after 3 months), however we also did not clearly indicate what is meant by early reconstruction.
Concerning the influence of the timing of ACL reconstruction on postoperative knee stability, there have been controversies in previous studies. 1,2,6 Bottoni et al 6 and Ahlen and Liden 1 found that there was no difference in postoperative knee stability between early and delayed reconstruction. On the other hand, Ahn and Lee 2 reported that the time from injury to surgery over 12 weeks was found to be a significant risk factor for postoperative instability after SB reconstruction. The results of the present study support the latter findings, in that early DB ACL reconstruction was significantly better in terms of postoperative anterior and rotatory knee stability than delayed DB ACL reconstruction.
There may be a criticism that a mean improvement of <1 mm in anterior laxity is not clinically significant for the patient, even though it is statistically significant. However, this improvement does not mean that postoperative anterior laxity was improved only by 1 mm in each knee. In addition, the knees in the early group had a significantly higher percentage of negative pivot-shift test results than those in the delayed group: 92% compared with 76%, respectively. Thus, we should regard the <1-mm improvement in knee laxity in the early group as resulting from the finding that early reconstruction could significantly increase the number of knees with normal knee laxity.
We considered a few possible mechanisms to explain these results. First, it is known that the intra-articular biological milieu immediately after an injury is significantly different from that in the chronic phase. 20,30,37,39 In addition, previous studies have reported that the intra-articular biological environment immediately after an ACL injury significantly affects healing of the graft after ACL reconstruction. 45,53,56 Therefore, there is a strong possibility that graft healing is more enhanced after early ACL reconstruction than after delayed reconstruction. Second, Signorelli et al 44 reported that the degree of anterior knee laxity gradually increases in the chronic ACL-deficient knee because the secondary restraints to anterior drawer loads are gradually relaxed. In the present study, the early group had fewer medial meniscal injuries and medial meniscectomy procedures. There is a possibility that the secondary restraints might have been more relaxed in the delayed reconstruction group than in the early reconstruction group and that this preoperative difference affected the anterior laxity results evaluated at the 2-year period. Third, several biomechanical studies have shown that DB reconstruction produces better knee stability compared with the commonly performed SB reconstruction technique. 24,25,49 In addition, many comparative studies have reported significant superiority in anterior and/or rotatory stability of the knee after DB reconstruction, while other studies have reported no differences between the 2 reconstruction techniques. 26,32,52
We believe that it is clinically important to restore normal knee stability because less than normal knee stability may cause meniscal injuries and osteoarthritic changes in the long term after ACL reconstruction, resulting in a reduction of functional results. We should note that all of the patients who underwent ACL reconstruction simply hoped to achieve the same stability and functionality. We consider that the ideal goal of ACL reconstruction is to simultaneously restore normal knee stability and function. From this viewpoint, early reconstruction can offer the clinical results of DB ACL reconstruction closer to the ideal goal. Further studies should be conducted to clarify the true mechanism.
The loss of knee motion caused by early ACL reconstruction has been a main focus in the debate concerning the best timing of ACL reconstruction after an injury. Harner et al 17 reported that early reconstruction with a BPTB graft, which was performed within 1 month after the injury, increased the risk of the loss of knee motion. On the other hand, Bottoni et al 6 found that early reconstruction using a hamstring tendon graft did not result in a loss of motion as long as a rehabilitation protocol emphasizing extension and early range of motion was employed. Thus, concerning the influence of the timing of ACL reconstruction on the clinical outcome, there has been controversy. The present study showed that there was no significant difference in postoperative range of knee motion between early and delayed ACL reconstruction using hamstring tendon grafts.
Postoperative muscle strength is known to be important for postoperative clinical outcomes. 40 Yasuda et al 55 clarified the isolated morbidity of hamstring tendon harvest in SB ACL reconstruction. They reported that the harvest did not significantly affect quadriceps muscle strength but that it reduced hamstring muscle strength for approximately 1 year. They also showed that ACL reconstruction itself significantly reduced quadriceps and hamstring muscle strength in the injured limb. Therefore, the postoperative reduction of quadriceps and hamstring muscle strength is caused by the combined effect of the graft harvest and surgical invasion. In the present study, even though there was a significant trend that preoperative muscle strength in the early reconstruction group was weaker than in the delayed reconstruction group, postoperative muscle strength was almost equal in all the 3 groups at 2 years after surgery. Eitzen et al 15 reported that patients with preoperative quadriceps muscle strength deficits >20% had persistent significantly larger strength deficits 2 years after surgery. However, de Jong et al 14 reported that although an increased preoperative quadriceps muscle strength deficit resulted in a lower functional score at 6 and 9 months postoperatively, the score improved by 12 months postoperatively. We considered that the weaker muscle strength measured immediately after the injury may be caused by knee pain because of posttraumatic inflammation and that it can be restored within a year if postoperative rehabilitation with common protocols is performed.
As for clinical relevance, the present study suggested that early DB ACL reconstruction using hamstring tendon grafts is beneficial to obtain better postoperative knee stability without any detrimental effects on the other clinical results, even though the mild improvements in anterior laxity did not improve functional outcome scores. Bottoni et al 6 suggested some theoretical advantages of early ACL reconstruction: (1) a faster return to full activities because there is no initial delay in beginning rehabilitation, and (2) further meniscal or chondral injuries that may occur if an athlete returns to some level of activities with an ACL-deficient knee may be avoided. In the present study, there was a significant trend that the incidence of medial meniscal injuries was significantly greater in the delayed reconstruction group. Previous studies 7,12,13,33 have also implied a strong possibility that early ACL reconstruction can reduce meniscal injuries postoperatively.
There are several limitations to this study. First, this is a retrospective study. The number of patients in group E, in which surgery was performed within 1 month after the injury, was less than that in the other groups because we decided the timing of ACL reconstruction according to the most common guideline, which recommended waiting at least 1 month from the injury. However, there were 25 patients who underwent ACL reconstruction within 1 month after the injury because of various circumstances, such as the patient’s motivation to undergo surgery and rehabilitation to return to school, an occupation, or a sports activity. In addition, patients competing in professional/collegiate sports may have undergone earlier reconstruction. Therefore, we should acknowledge that this was not a randomized study and that there may be inherent bias between groups. On the other hand, we have a limited schedule for orthopaedic surgery in the operation theater of our university hospital. All ligament surgical procedures are planned in order of admission because ACL reconstruction is not an emergency in our hospital. Therefore, we decided this timing without knowing the condition of the knee at the time of reconstruction, such as the stiffness of the knee, meniscal injuries, and articular cartilage damage. This retrospective study was conducted to verify this common guideline. Although we considered that the number of samples was enough according to the power analysis using previous KT-1000 arthrometer measurements, there is a possibility of type I and II errors concerning the other evaluations. The results of this study suggest the validity of a prospective randomized study to confirm the conclusion obtained in the present study.
Second, the follow-up period was for a minimum 2 years in the present study, which was performed by a single research group. Therefore, long-term follow-up and multicentric studies are needed. However, previous clinical studies on the timing of ACL reconstruction were conducted using a short-term follow-up study design: For example, Shelbourne et al 43 and Bottoni et al 6 reached their landmark conclusions in the follow-up period of a minimum of 13 weeks and 6 months, respectively. Therefore, we believe that the follow-up period in the present study was acceptable. Third, early postoperative KT-2000 arthrometer measurements were not obtained in this study. Therefore, there is a possibility that the patients had different anterior knee stability between immediately after surgery and at 2 years postoperatively. Fourth, the present study did not include intra-articular evaluations with second-look arthroscopic surgery at the final follow-up period. However, knee laxity and range of knee motion can be determined independently of the intra-articular conditions.
Conclusion
This retrospective case-control study was conducted to clarify the impact of the timing of anatomic DB ACL reconstruction using hamstring tendon autografts on the clinical outcome in 171 patients. The present study showed that, first, postoperative anterior laxity in the early group was significantly less than that in the delayed group. Second, there were no significant differences in postoperative range of knee motion or the functional results among the 3 groups. Third, even though preoperative strength of the quadriceps and hamstring muscles was significantly lower in the patients who underwent early reconstruction than in those who underwent delayed reconstruction, this difference disappeared 2 years after surgery. The results of this study suggest the validity of a prospective randomized study to confirm these findings.
Footnotes
One or more of the authors declared the following potential conflict of interest or source of funding: This work was supported in part by a Grant-in-Aid for Scientific Research (16H03158) from the Ministry of Education, Culture, Sports, Science and Technology of Japan. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board of Hokkaido University Hospital.