
Abstract
Introduction
The meniscus plays an important role in load transmission, shock absorption, and maintenance of joint stability. 1 Its most important function is the maintenance of hoop tension, which allows for correct intra-articular load transmission and prevention of osteoarthritis—with the medial meniscus (MM) undertaking the bulk (approximately 90%) of this responsibility. 2
Recently, many studies have reported about MM posterior root tear (MMPRT) which is an injury to the posterior meniscal insertion on the tibia. In a normal knee, the MM moves posteriorly when the knee flexes, 3 whereas in a knee with MMPRT, the MM shows severe posterior extrusion (PE) from the tibial plateau in knee flexion as well as medial extrusion (ME). 4 Additionally, MMPRT leads to the inability to convert axial loads into hoop stress and greatly increases the contact pressure on the medial compartment of the knee joint, resulting in an increase in friction and development of osteoarthritis in the articular cartilage; further, it occasionally results in subchondral insufficiency fractures. 5 Biomechanical studies have reported that MMPRT caused a 25% increase in the peak contact pressure, whereas MM posterior root (MMPR) repair led to the restoration of peak contact pressure to normal levels. 6 Many MMPR repair techniques have been developed. Traditionally, a conservative treatment, meniscectomy, meniscal repair, and pullout repair were performed to treat an MMPRT. Previous studies showed that a conservative treatment or a partial meniscectomy in MMPRT led to joint space narrowing and a progression of varus deformity, resulting in osteoarthritis. 7 Although one study suggested that satisfactory clinical outcomes of conservative treatment could be expected in patients with either absent or mild varus limb malalignment or chondral damage, 8 most patients with MMPRT have mild-moderate varus deformity and chondral lesions. Because of the unfavorable success rate of conservative treatment or partial meniscectomy for these patients with MMPRT, MMPR repairs were recommended to obtain favorable clinical outcomes by preventing subsequent meniscal extrusion and cartilage degeneration, 9 provided the patient could meet the indications such as a body mass index <30 kg/m2. 10
Previous studies have described that pullout repairs reduced the posteromedial extrusion especially at 90° knee flexion.11–13 However, the difference in MMPE following the use of different repair techniques is still unknown. This study aimed to investigate and compare preoperative and postoperative MMPE after different pullout repair techniques, including FasT-Fix 360 meniscal repair system (Smith & Nephew, Andover, MA, USA) -dependent modified Mason-Allen suture (F-MMA) and two simple stitches (TSS) with/without an all-inside suture to the posteromedial portion of the MM, as previously described.14–16 In this study, we hypothesized that TSS, but not F-MMA, could prevent the progression of MMPE in knee extension postoperatively.
Materials and methods
Patients
Data were retrospectively collected from medical records. This study was approved by the Institutional Review Board of our institution and was performed in accordance with the Declaration of Helsinki. All patients provided written informed consent prior to participation. This study conforms to the STROBE cohort reporting guidelines. 17
From October 2016 to August 2019, 55 patients diagnosed with MMPRT underwent pullout repairs using F-MMA and TSS at our institution were included in this study. Pullout repairs using F-MMA and TSS techniques have been performed since October 2016 until October 2017 and April 2018 until August 2019, respectively. All patients were diagnosed with MMPRT according to characteristic magnetic resonance imaging (MRI) findings such as cleft, giraffe neck, and ghost signs.18,19 A pullout repair is indicated for patients with a body mass index <30 kg/m2, femorotibial angle <180°, mild cartilage lesions (Outerbridge grades I or II), and osteoarthritis grades 0-2 (Kellgren–Lawrence classification), which were confirmed by preoperative radiographs or MRI. Patients with no available MRI data, other meniscal injuries, anterior cruciate ligament injuries, or a history of surgery in the ipsilateral knee were excluded. Finally, this retrospective study included 18 and 17 cases in the F-MMA and TSS groups, respectively. The MMPRT types were determined by careful arthroscopic examinations according to the meniscal root tear classification. 20
Surgical procedure
Pullout repairs for MMPRT were performed by a single well-experienced surgeon with a standard anterolateral portal for arthroscopic visualization using a 4 mm diameter 30° arthroscope (Smith & Nephew) for both groups. A standard anteromedial portal was used for the instruments. In cases with a tight medial compartment, we used the outside-in pie-crusting technique for releasing the medial collateral ligament by using a standard 18-gauge (1.2 × 40 mm) hypodermic needle (TERUMO, Tokyo, Japan). 21
In the F-MMA group, the torn end of the MMPR or horn was grasped using the F-MMA as previously described. 14 In brief, a No. 2 Ultrabraid (Smith & Nephew) suture was passed through the MM posterior tissue using a Knee Scorpion suture passer (Arthrex, Naples, FL, USA), and two implants of the FasT-Fix were inserted into the MMPR or horn across the Ultrabraid suture.
In the TSS group, the torn end of the MMPR and horn was grasped using TSS as previously described. 15 In brief, two No. 2 Ultrabraid sutures were passed through the meniscal tissue using a Knee Scorpion suture passer. The first suture was inserted into the outer area of the MM posterior root, and the second was inserted into the inner area of the MM posterior horn.
A tibial tunnel was created at the expected anatomic center (referring to the medial tibial plateau, the posterior peak of the medial tibial eminence, and the anterior border of the posterior cruciate ligament) using a MMPRT guide (Smith & Nephew) in both groups. In the F-MMA group, tibial fixation was performed using a double-spike plate and screw (Meira, Aichi, Japan) at 45° knee flexion with 20 N of initial tension using a spring tensioner, 14 whereas in the TSS group, tibial fixation was performed using a bioabsorbable interference screw (Biosure RG, Smith & Nephew) and a cancellous screw (Meira) at 20° knee flexion with 30 N of initial tension. 15
Assessments of radiographs and magnetic resonance images
The Rosenberg 45° posteroanterior standing view was used to assess the Kellgren–Lawrence classification preoperatively and 12 months postoperatively.
Open MRI was performed using an Oasis 1.2 T system (Hitachi Medical, Chiba, Japan) with a coil at 10° and 90° knee flexion, under non–weight-bearing conditions as previously described.22,23 The standard sequences of the Oasis system included a sagittal proton density-weighted sequence (repetition time [TR]/echo time [TE], 1718/12), using a driven equilibrium pulse with a 90° flip angle and a coronal T2-weighted multi-echo sequence (TR/TE, 4600/84) with a 90° flip angle. The slice thickness was 4 mm with a 0 mm gap. The field of view was 16 cm with an acquisition matrix size of 320 (phase) × 416 (frequency).
11
Measurements were performed using a simple MRI-based meniscal sizing technique using the sagittal and coronal views at 10° and 90° knee flexions as previously described.
4
In brief, MMPE was defined as the distance from the posterior edge of the tibia (excluding osteophytes) to the posterior edge of the MM. Using the posterior edge of the tibia as the standard, extrusions toward the posterior from the tibial edge were given positive values, whereas negative values were defined as the absence of such extrusions. For all patients, MMPE was measured at 10° and 90° knee flexions preoperatively and at 3 and 12 months postoperatively (Figures 1 and 2). Magnetic resonance images of the knee in the FasT-Fix-dependent modified Mason-Allen suture group. (a): Preoperative image at 10° knee flexion. Medial meniscus posterior extrusion (MMPE) is −3.58 mm. (b): Three-month postoperative image at 10° knee flexion showing increased MMPE (−1.07 mm), compared to the preoperative MMPE. (c): Twelve-month postoperative image at 10° knee flexion showing increased MMPE (−1.41 mm), compared to the preoperative MMPE. (d): Preoperative image at 90° knee flexion. MMPE is 3.12 mm. (e): Three-month postoperative image at 90° knee flexion showing decreased MMPE (1.61 mm), compared to the preoperative MMPE. (f): Twelve-month postoperative image at 90° knee flexion showing decreased MMPE (1.87 mm), compared to the preoperative MMPE. The distance between the posterior margins of the medial tibial plateau (solid lines) and the medial meniscus (dashed lines) is defined as MMPE. Magnetic resonance images of the knee in the two simple stitches group. (a): Preoperative image at 10° knee flexion. Medial meniscus posterior extrusion (MMPE) is −2.47 mm. (b): Three-month postoperative image at 10° knee flexion showing nearly the same MMPE as preoperatively (−2.89 mm). (c): Twelve-month postoperative image at 10° knee flexion showing increased MMPE (−2.43 mm), compared to the preoperative MMPE. (d): Preoperative image at 90° flexion. MMPE is 3.55 mm. (e): Three-month postoperative image at 90° flexion showing decreased MMPE (1.33 mm), compared to the preoperative MMPE. (f): Twelve-month postoperative image at 90° flexion showing decreased MMPE (1.42 mm), compared to the preoperative MMPE.

Statistical analysis
Data are presented as means ± standard deviations. Statistical analysis and power calculation were performed using EZR software (Saitama Medical Center, Jichi Medical University, Tochigi, Japan). 24 Two orthopedic surgeons independently measured MMPE in a blinded manner. Each observer performed each measurement twice at least 2 weeks apart. Intra- and inter-observer reliability was assessed by intraclass correlation coefficient (ICC). An ICC value of >0.80 was considered to represent a reliable measurement. An ICC of ≥0.75 was considered excellent, ≥0.60 to <0.75 good, ≥0.40 to <0.60 fair, and <0.40 poor. 25 Intra- and inter-group differences were compared using the repeated-measures analysis of variance (rANOVA) with the Bonferroni post hoc tests and Mann–Whitney U test, respectively. The significance level was set at p < .05.
Results
Demographic and clinical characteristics of patients (n=35) in the F-MMA and TSS groups.

Age, height, weight, body mass index, femorotibial angle, and duration from injury to surgery are presented as mean ± standard deviation.
F-MMA, FasT-Fix-dependent modified Mason-Allen suture; TSS, two simple stitches.
Magnetic resonance imaging–based MMPE.

Data are presented as mean ± standard deviation.
3
a Significant difference was observed using Mann–Whitney U test.
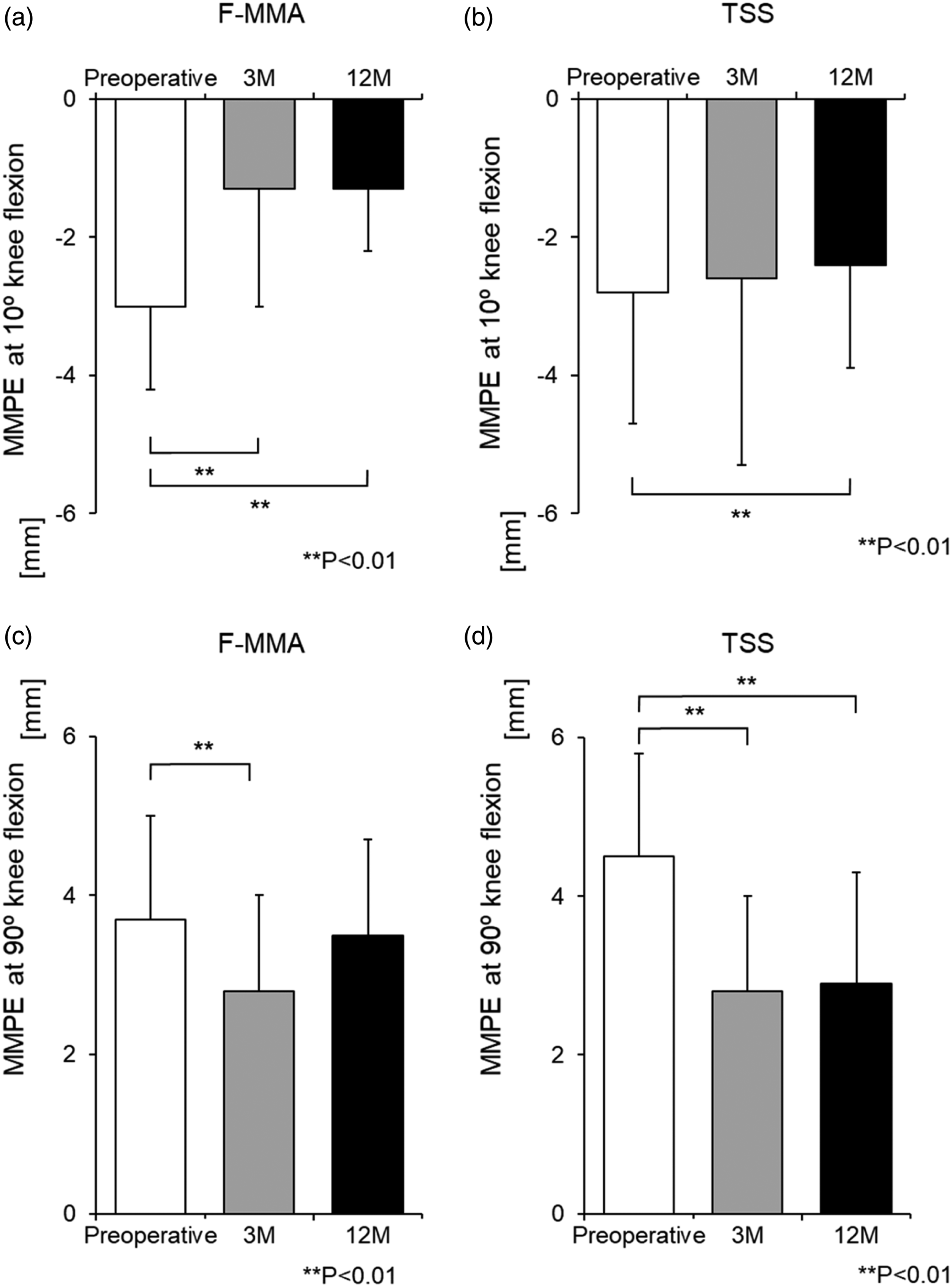
Comparison between the preoperative, 3- and 12-month postoperative MMPE of each group. (a): A significant increase in the 3- and 12-month postoperative MMPE at 10° knee flexion is observed, compared to the preoperative MMPE in the F-MMA group. ** p < .01. (b): No significant difference is observed between preoperative and 3-month postoperative MMPE at 10° knee flexion, although a significant increase is observed between preoperative and 12-month postoperative MMPE in the TSS group. ** p < .01. (c): A significant decrease in the 3-month postoperative MMPE at 90° knee flexion is observed, compared to the preoperative MMPE. ** p < .01. (d): A significant decrease in the 3- and 12-month postoperative MMPE at 90° knee flexion is observed, compared to the preoperative MMPE in the TSS group. ** p < .01. MMPE, medial meniscus posterior extrusion; F-MMA, FasT-Fix-dependent modified Mason-Allen suture; TSS, two simple stitches.
Figure 4 shows comparison between MMPE in the F-MMA and TSS groups. A significant difference was observed in 10° knee flexion only in the 3- and 12-month postoperative MMPE (p = .04/.02, power = 0.48/0.69, Figures 4(c) and (e)). Intra- and inter-observer reliabilities for the measurements of MMPE were considered satisfactory (mean ICC value was 0.85–0.92 and 0.84, respectively). Comparison between MMPE in the FasT-Fix-dependent modified Mason-Allen suture (F-MMA) and two simple stitches (TSS) groups. (a): No significant difference in the preoperative MMPE at 10° knee flexion is observed between the F-MMA and TSS groups.(b): No significant difference in preoperative MMPE at 90° knee flexion is observed between the F-MMA and TSS groups.(c): A significant difference in the 3-month postoperative MMPE at 10° knee flexion is observed between the F-MMA and TSS groups. *p < .05.(d): No significant difference in 3-month postoperative MMPE at 90° knee flexion is observed between the F-MMA and TSS groups.(e): A significant difference in 12-month postoperative MMPE at 10° knee flexion is observed between the F-MMA and TSS groups. *p < .05.(f): No significant difference in 12-month MMPE at 90° knee flexion is observed between the F-MMA and TSS groups.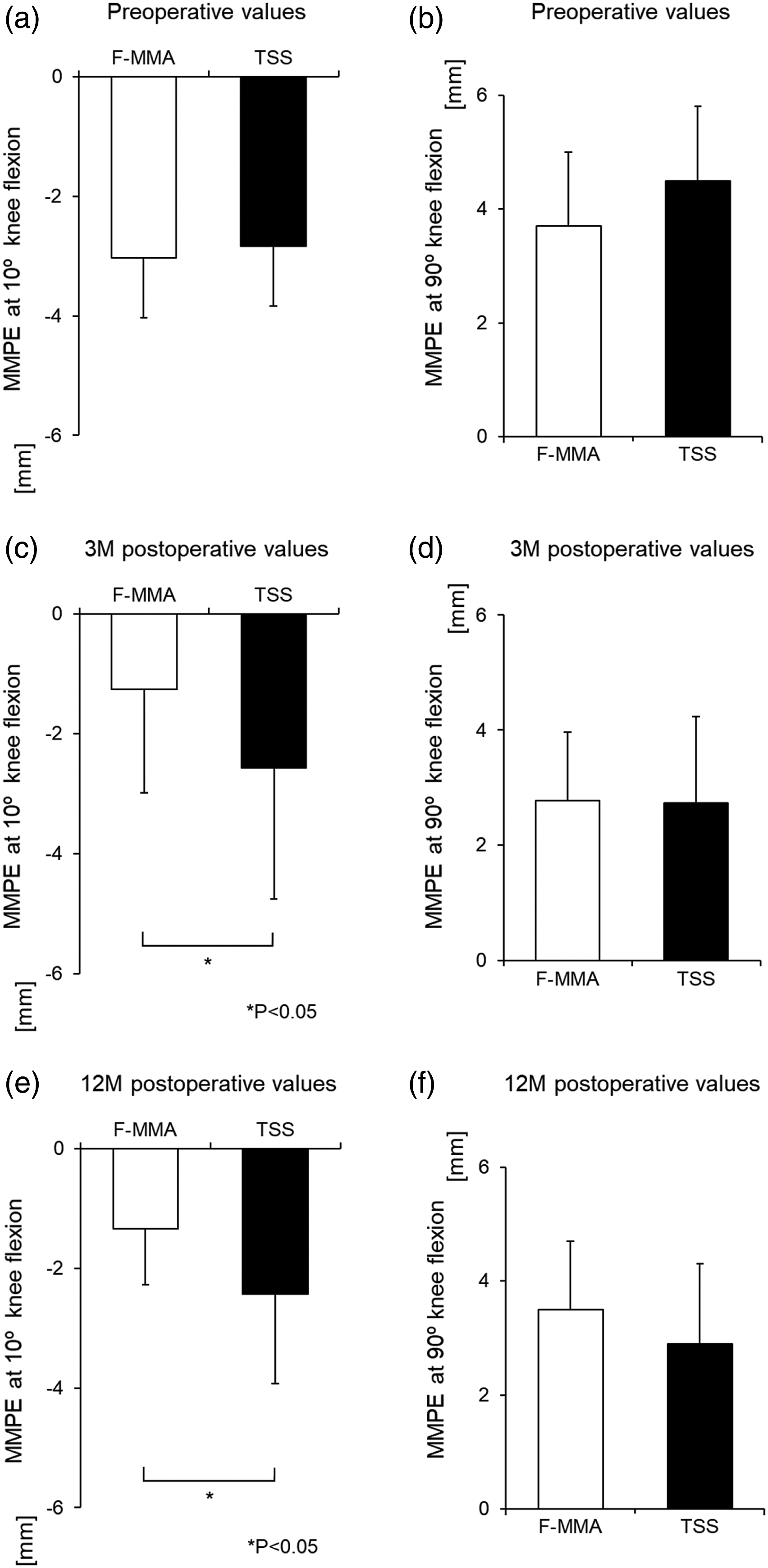
Discussion
The most important finding in this study was that the TSS technique was better at preventing the progression of postoperative MMPE in knee extension than the F-MMA technique. These results confirmed our hypothesis.
MMPRT leads to severe MM medial extrusion (MMME) and MMPE during knee flexion, 4 resulting in a loss of hoop tension and an increase in contact pressure. 26 Because a conservative treatment or a partial meniscectomy in MMPRT would result in an unfavorable clinical outcome, 7 pullout repairs are recommended to restore the biomechanical change in the knee and to reduce MMPE and tibial rotation in knee flexion.27,28 Many studies have reported on MMME in MMPRT. Previous studies have linked increased MMME measurements to unfavorable clinical scores and progression of osteoarthritis in the knee. 29 Thus, an early and accurate decision for pullout repairs of MMPRT is important to prevent the increase of MMME. An episode of posteromedial painful popping and specific MRI findings such as cleft, ghost, and giraffe neck signs are important for diagnosis. 30 However, some studies have reported that MMME does not completely decrease even after a pullout repair is performed. 9 In this study, the MMPE measurements in 90° knee flexion have decreased after the pullout repair in both groups.
To prevent the progression of MM extrusion, the surgical procedures for MMPR repair (all-inside technique, Mason-Allen or modified Mason-Allen sutures, and TSS with or without an additional suture to the extruded posteromedial portion) have improved.15,16,22,31,32 It was previously reported that the F-MMA technique suppressed the progression of MMPE in knee flexion, 22 and in this study, both the F-MMA and TSS techniques improved 3-month postoperative MMPE in 90° knee flexion significantly. In the comparison between the two groups, the 3- and 12-month postoperative MMPE in knee extension was smaller in the TSS group than in the F-MMA group. Therefore, the contact area and pressure in knee flexion could be improved to the same extent in both groups, and those in knee extension could be improved significantly more in the TSS group compared with the F-MMA group.
Based on these findings, it was concluded that the TSS technique might be more useful for improving load distribution than the F-MMA technique. This can be advantageous when standing or walking because the knee flexion angle when standing or walking is less than 30°. In the TSS group, the posterior capsule was not grasped; thus, the MMPE in knee extension did not increase. This might lead to high medial tibial plateau coverage, resulting in an increased contact area, decreased contact pressure, and cartilage preservation. On the contrary, in the F-MMA group, the FasT-Fix penetrated through the posterior capsule when grasping the MMPR or horn; thus, it may have applied force in the direction of the MMPE. The reason for the absence of a significant difference in the flexion position is that the posterior capsule loosens in the flexion position so that the posterior force by the all-inside suture is reduced.
This study had several limitations. First, this was a retrospective study with a small sample size. Second, the relationship between MMPE at 10° knee flexion and the clinical results was still unclear, although the short-term results were favorable in both groups. 33 Third, the actual biomechanical change in the knee joint was not studied in both techniques. Finally, we could only evaluate MM translation under non–weight-bearing conditions. Further studies using a prospective design, a larger sample size, and a long-term follow-up under weight-bearing conditions (if possible) should be performed in the future.
Conclusion
Both the F-MMA and TSS techniques were useful for the reduction of MMPE at 90° knee flexion. In addition, the TSS technique prevented the progression of MMPE better than the F-MMA technique at 10° knee flexion. These findings suggest that the TSS technique has advantages over F-MMA for load distribution when standing or walking.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.