
Abstract
Background:
Lumbar spine injuries in National Collegiate Athletic Association (NCAA) athletes have not been well studied.
Purpose:
To describe the epidemiology of lumbar spine injuries in NCAA athletes during the 2009/2010 through 2013/2014 academic years utilizing the NCAA Injury Surveillance Program (ISP).
Study Design:
Descriptive epidemiology study.
Methods:
A voluntary convenience sample of NCAA varsity teams from 25 sports was examined. Mechanism of injury, injury recurrence, and time lost from sport were recorded. Injury rates were calculated as the number of injuries divided by the total number of athlete-exposures (AEs). AEs were defined as any student participation in 1 NCAA-sanctioned practice or competition. Injury rate ratios and injury proportion ratios were calculated to compare the rates within and between sports by event type, season, patient sex, mechanism, injury recurrence, and time lost from sport. Comparisons between sexes were made utilizing data that had both male and female samples.
Results:
An estimated 50,834 lumbar spine injuries were identified. The overall rate of injuries was 2.88 per 10,000 AEs. The rate of injuries was 2.60 per 10,000 AEs in men compared with 2.89 per 10,000 AEs in women for sex-comparable sports. Women were 1.11 times more likely than men to suffer a lumbar spine injury. Women's gymnastics (8.02 injuries per 10,000 AEs) and women's tennis (5.73 injuries per 10,000 AEs) had the highest rates of lumbar spine injuries. Athletes were 1.6 and 2.4 times more likely to sustain a lumbar spine injury during the preseason than the regular season or postseason, respectively. Noncontact was the most common mechanism of injury (45%). Injury recurrence was most common in men’s outdoor track (43%). Most injuries resulted in less than 24 hours of time loss from event participation (64%).
Conclusion:
The rate of lumbar spine injuries was high in NCAA athletes, and injuries commonly recurred (20.73%). In general, women were more likely to sustain a lumbar spine injury compared with men. Higher injury rates occurred during competition and via a noncontact mechanism of injury. In addition to prevention programs, reconditioning programs should be considered to prevent these injuries.
Injuries to the lumbar spine among collegiate athletes are relatively common. 7 The osseous, musculoligamentous, and neuroanatomical aspects of the spine allow for complex multiplanar movements, and dysfunction of any one of these structural elements can lead to injuries. 7,19 As injuries vary, multiple causes of lumbar spine injuries and disorders are reported among collegiate athletes. 7,17
Prior nationwide epidemiological studies have suggested that half of adults in the United States experienced back pain within a given year, and 15% reported “frequent” pain or symptoms lasting longer than 2 weeks. 5 In the collegiate athlete, back injuries are also common. 4,10 Injuries can occur from either a direct injury or from subjective muscle imbalances that prevent optimal kinematics during athletic participation, which lead to injuries or disorders. 17 –20 The previous literature has described both traumatic injury mechanisms and overuse injuries that lead to back abnormalities. 1 Additionally, there has been a reported association of lumbar spine injuries after any lower extremity injury, with a reported incidence of 24% among collegiate athletes. 18 Despite the prevalence of lumbar spine injuries in collegiate athletes, limited literature exists characterizing these injuries. Further characterization of these injuries is needed to develop better prevention and treatment algorithms.
The current literature describing lumbar spine injuries in athletes is limited to the National Football League (NFL) and minimal college samples. 11,16,18 Furthermore, college-level studies have focused on single-university samples with smaller sample sizes. 11,18 As such, a larger epidemiological description of low back injuries in college-level athletes across multiple sports does not yet exist. 1,10,18 Therefore, the purpose of this study was to provide the epidemiological background of lumbar spine injuries recorded among National Collegiate Athletic Association (NCAA) athletes from the 2009/2010 to 2013/2014 academic years using the NCAA Injury Surveillance Program (ISP).
Methods
The study was granted institutional review board exemption from our institution, given the deidentified nature of the database. It was subsequently approved by the research review board of the NCAA. The NCAA ISP is a prospectively gathered injury surveillance system managed by the Datalys Center for Sports Injury Research and Prevention, which is an independent nonprofit research organization. 6 This study included voluntarily submitted self-reported data available for the 2009/2010 to 2013/2014 academic years. The methodology for data gathered in the NCAA ISP has previously been described in the literature and is briefly reviewed below. 12,13
Data Collection
The NCAA ISP utilizes a voluntary self-reported convenience sample of NCAA varsity teams from 25 sports. These 25 sports include men’s football, wrestling, and baseball; women’s volleyball, field hockey, gymnastics, and softball; and men’s and women’s ice hockey, soccer, basketball, lacrosse, indoor track and field, outdoor track and field, cross-country, swimming and diving, and tennis. There is variability in the number of programs participating and the sports reported among the years in the data set. 9,12
Athletic trainers (ATs) working with each participating program are responsible for recording injury and exposure data electronically through each institution’s electronic health record. Data are collected only from varsity-level organized practices and competitions during the preseason, regular season, and postseason. For each injury occurrence, ATs and/or physicians complete a detailed report on the injury itself as well as the circumstances surrounding the injury. 12 Injury data collected include anatomic site, diagnosis, and circumstances of the injury; real time missed from sport; and event type. 12,23 ATs also record the number of student-athletes participating in each practice and competition to determine exposures. 21 After initially inputting injury data, the ATs can return to view and update the data as needed over the course of a season for a change in performance status/condition or return to participation.
Deidentified common data elements were extracted from these certified electronic health record applications. 9,12 Exported data passed through an automated verification process that conducted a series of range and consistency checks limiting outliers. Data that passed the verification process were then placed into the aggregate research data set.
Definitions
Injury
A reportable injury in the NCAA ISP was defined as an injury that (1) occurred as a result of participation in an organized intercollegiate practice or competition, (2) required attention from an AT or physician, and (3) resulted in restriction of the student-athlete’s participation for ≥1 days beyond the injury. 12 Multiple injuries occurring from 1 injury event could be included. If an off-day followed the injury event, the AT was asked to assess whether the injured athlete would have been able to participate. 12 For muscle imbalances or overuse events that restricted an athlete’s participation but did not have associated imaging or a specific diagnosis, the term “sports-associated lumbar disorders” was more appropriately used.
The current study considered all injuries referencing “lower back” or “lumbar” in the definition of lumbar spine injuries. We relied on the training and expertise of the ATs collecting data, as well as other members of the team medical staff assisting in documentation, to accurately diagnose and report all lower back injuries. Radiological studies were not required before inclusion in the data set. The most recently updated diagnoses were used.
Athlete-Exposure
An athlete-exposure (AE) was defined as 1 student-athlete participating in 1 NCAA-sanctioned practice or competition in which he or she was exposed to the possibility of an athletic injury, regardless of the time associated with that participation. 12 For the competition to be considered an exposure, the athlete had to have actual playing time during the event. 12 AEs were limited to varsity-level NCAA-sanctioned practices and competitions occurring in the preseason, regular season, or postseason. 12 AEs were recorded by ATs entering data.
Event Type
Event type was the event, either practice or competition, during which the injury occurred.
Season of Play
Season of play was the season segment (ie, preseason, regular season, postseason) in which the injury occurred.
Injury Mechanism
Injury mechanism was defined as the manner in which the student-athlete sustained his or her injury. In the NCAA ISP, ATs selected from a preset list of options, including player contact, surface contact, equipment contact, contact with an out-of-bounds object, noncontact, overuse, illness, infection, and other/unknown. All contact events were condensed under the title “contact.” Given the lack of lumbar spine injuries being caused by illness or infections (none reported in the convenience sample), these 2 mechanisms were excluded from analysis. Additionally, missing, unknown, or unreported data were demarcated “missing.”
Recurrence
Recurrent injuries were defined as a recurrence of the same injury that occurred previously in the same athlete, either during the current or previous seasons after the athlete had returned to play from a prior injury.
Participation Restriction Time
Injuries were categorized by the number of days that participation was restricted (ie, the date of return subtracted by the date of injury). Participation was considered restricted until an athlete was cleared for unrestricted competition. Injuries resulting in participation restriction <24 hours were also included.
Computing National Estimates
To calculate national estimates of the number of lower back injuries, poststratification sample weights based on sport, division, and academic year were applied to each reported injury and AE. Poststratification sample weights were calculated with the following formula:

where weightabc is the weight for the ath sport of the bth division in the cth year. Weights for all data were further adjusted to correct for underreporting, accounting for the estimated 88.3% capture rate of all time-loss medical care injury events within the NCAA ISP previously reported in the literature. 15
Statistical Analysis
Data were analyzed to assess the rates and patterns of lumbar spine injuries sustained by collegiate athletes. Lumbar spine injuries were analyzed for injury type, time loss, time of season, event type, recurrence, injury mechanism, and participation restriction. The injury rate was defined as the number of injuries divided by the number of AEs. The rates were reported as the ratio of injuries per 10,000 AEs and were calculated for an overall rate as well as individual rates for event type (practice vs competition) and time of season (preseason, regular season, and postseason). Injury rate ratios (IRRs) were calculated to compare rates between event types and by time of season, as they are useful for determining whether one participation type has an increased rate of injuries compared with another. The following is an example of an IRR comparing injury rates between competition and practice:

Injury proportion ratios (IPRs) were calculated to examine differences in injury rates and the distribution among sex-comparable sports (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, and tennis). The following is an example of an IPR comparing the proportion of lower back injuries that were severe in men and women:
All 95% CIs not containing 1.0 were considered statistically significant. Participation restriction time was reported as intervals (<24 hours, 1-6 days, 7-21 days, and >21 days), and descriptive data were presented as percentages of injuries (recurrence, event type, mechanism of injury, etc). Data were analyzed using SPSS software (IBM) and Excel (Microsoft).
Results
Frequencies and Rates
Overall, 1167 lumbar spine injuries and disorders were reported to the NCAA ISP during the 2009/2010 to 2013/2014 academic years among 25 varsity sports (Table 1). The 1167 injuries in this sample represent a national estimate of 50,834 total lumbar spine injuries/sports-associated lumbar spine disorders, estimated by using the nonweighted calculation outlined above. The overall injury rate was 2.88 LSIs per 10,000 AEs based on the reported 1167 injuries in our sample. In sex-comparable sports, a total of 392 injuries occurring in men’s sports were reported to the database, while a total of 347 injuries in women’s sports were reported. These injuries corresponded to injury rates of 2.60 and 2.89 per 10,000 AEs, respectively. Among all sports recorded by the NCAA ISP during the 2009/2010 to 2013/2014 academic years, men’s football sustained the highest number of injures (n = 276; national estimate of 7315). However, women's gymnastics had the highest rate of injury, 8.02 per 10,000 AEs (Table 1).
Lumbar Spine Injury Rates Among Student-Athletes in 25 Sports a

a AE, athlete-exposure.
b National estimates for sports may not sum to total because of rounding.
c One student-athlete participating in 1 practice or 1 competition.
d Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Event Type
The overall number of lumbar spine injuries was highest during practice (n = 851); however, the injury rate during competition was higher than during practice (3.58 vs 2.72 per 10,000 AEs, respectively; IRR, 1.32 [95% CI, 1.16-1.50]), which reached statistical significance. Injury rates were significantly higher during competition in men’s basketball (IRR, 3.64 [95% CI, 2.35-5.62]), men’s football (IRR, 3.20 [95% CI, 2.46-4.17]), men's ice hockey (IRR, 1.59 [95% CI, 1.08-2.33]), men's lacrosse (IRR, 2.02 [95% CI, 1.05-3.88]), women's soccer (IRR, 2.15 [95% CI, 1.33-3.46]), men's wrestling (IRR, 2.23 [95% CI, 1.00-4.67]), and men’s sports overall (IRR, 1.34 [95% CI, 1.08-1.66]). The only sport in which the injury rate was higher during practice was women’s volleyball (IRR, 0.43 [95% CI, 0.23-0.80]) (Table 2).
Lumbar Spine Injury Rates Among Student-Athletes in 25 Sports by Event Type a

a AE, athlete-exposure; IRR, injury rate ratio; N/A, not applicable.
b One student-athlete participating in 1 practice or 1 competition.
c Denotes statistical significance.
d Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Sex Differences
Among sex-comparable sports, men sustained a lower injury rate overall than women (2.60 vs 2.89 per 10,000 AEs, respectively; IRR, 0.89 [95% CI, 0.78-1.04]). There was no statistical difference in event type, season of injury, injury mechanism, or injury type among the sex-comparable sports in terms of frequencies.
Injury Mechanism
Noncontact mechanisms of injury were the most common (n = 20,467; 40%), with overuse injuries comprising the second largest overall proportion (n = 13,926; 27%) of lower back injuries. Among sex-comparable sports, noncontact injuries comprised the largest proportion of injuries in men’s sports (38%), while overuse injuries were most common in women’s sports (45%) (Table 3).
Distribution of Lumbar Spine Injuries Among Student-Athletes in 25 Sports by Injury Mechanism a

a Data are presented as n (%).
b Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Recurrence
Overall, 20.73% of lumbar spine injuries were recurrent. The sports with the highest rates of recurrent lumbar spine injuries were men’s outdoor track, men’s tennis, and women’s outdoor track (43.15%, 37.95%, and 35.01%, respectively). Of note, new injuries comprised the majority of reported injuries in all sports (Figure 1).

Proportion of recurrent (orange) and new (blue) lower back injuries among student-athletes in 25 sports: National Collegiate Athletic Association Injury Surveillance Program, 2009/2010 to 2013/2014 academic years. *Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Time Away From Sport
Among athletes suffering a lumbar spine injury, the majority spent <24 hours away from sport (n = 29,925; 64%) with a 1–calendar day restriction from play. Overall, only 4.68% of athletes suffered an injury that required >21 days away from sport. There was no difference between time missed because of an injury between men or women for sex-comparable sports (Table 4).
Distribution of Lumbar Spine Injuries Among Student-Athletes in 25 Sports by Participation Restriction Time a

a Data are presented as n (%).
b Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Season of Play
The overall season of play in which most injuries occurred was the regular season, with 700 total injuries (injury rate of 2.47 per 10,000 AEs) (Table 5). However, the highest injury rate occurred during the preseason (4.03 per 10,000 AEs). Among sex-comparable sports, men and women both had higher injury rates, 3.42 and 4.10, respectively, during the preseason when compared with either the regular season or postseason (IRR preseason to regular season, 1.63 [95% CI, 1.44-1.83]; IRR preseason to postseason, 2.42 [95% CI, 1.72-3.42]). There was no difference between the sexes in injury rates per season.
Distribution of Lumbar Spine Injuries Among Student-Athletes in 25 Sports by Season of Play a
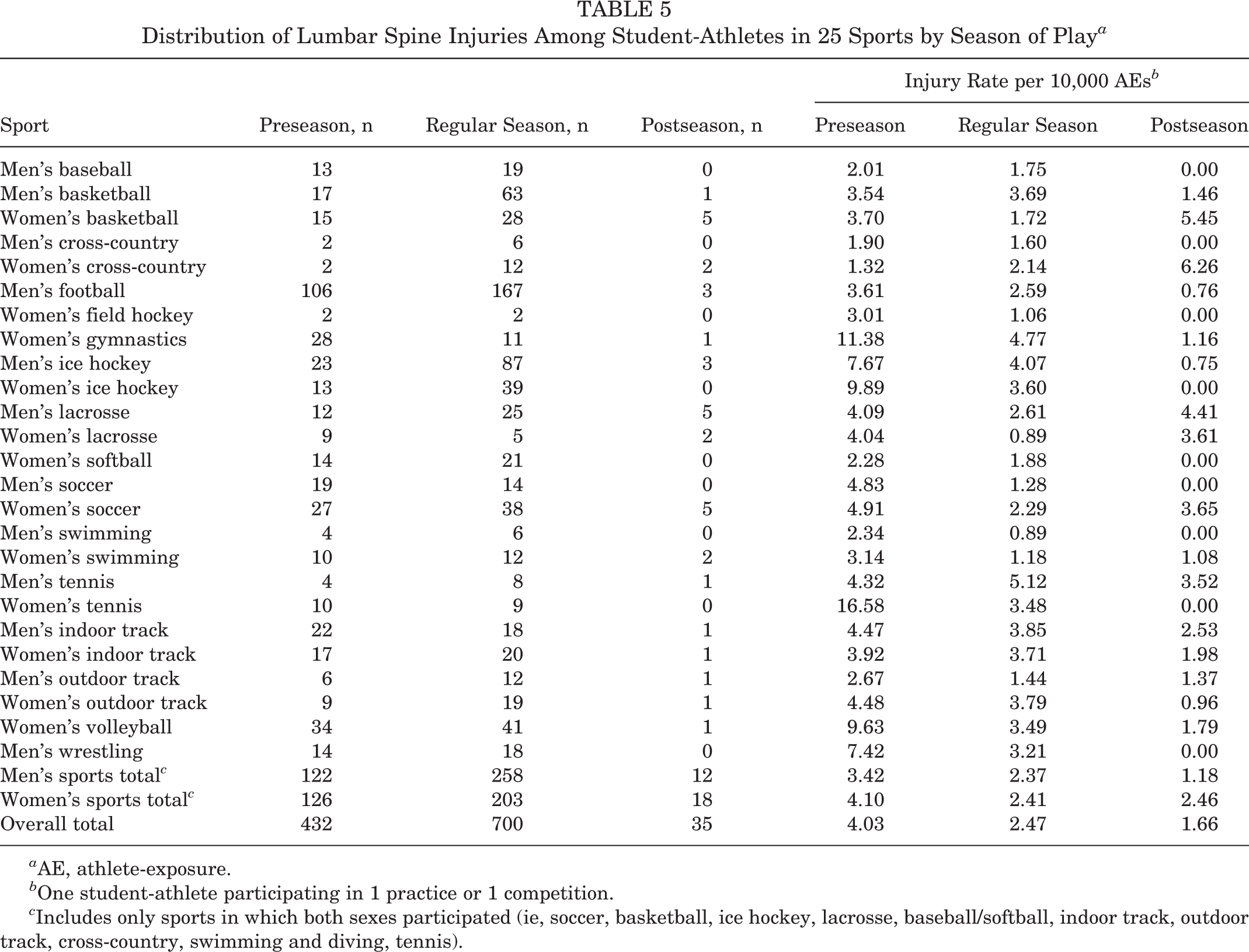
a AE, athlete-exposure.
b One student-athlete participating in 1 practice or 1 competition.
c Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Injury Types
Among all lumbar spine injuries included in the data set, the majority were classified as lower back strains (n = 23,119; 45%). Lower back strains were the most common types of injury in both men’s and women’s comparable sports as well (47% and 44%, respectively). The second most common injury type was pain (unspecified); this accounted for 40% of the overall injury types (Table 6).
Distribution of Lumbar Spine Injuries Among Student-Athletes in 25 Sports by Injury Type a

a Data are presented as n (%).
b Includes only sports in which both sexes participated (ie, soccer, basketball, ice hockey, lacrosse, baseball/softball, indoor track, outdoor track, cross-country, swimming and diving, tennis).
Discussion
The major strength of this study is the ability to characterize a relatively common set of injuries in collegiate athletes. The current literature describing back injuries in athletes is limited to the professional level or smaller sample size studies. Our study is the first to examine the epidemiology of these lower back injuries in collegiate athletes from a convenience sample across 25 NCAA sports. Examining the injury rates, event type, sex-comparable differences, recurrence, injury mechanism, type, and time away from sport will allow for better estimates of injuries at the collegiate level. This potentially helps athletes better understand the potential risks of sports-associated lumbar spine disorders/injuries involved with collegiate athletics. Further work could focus on the use of epidemiological studies such as this to help with the development of prevention and rehabilitation programs that can be sport/sex/mechanism dependent.
The overall high injury rates (see Table 1) in this study complement the previous literature, which has demonstrated a high rate of injuries associated with the lumbar spine region in collegiate athletes. 2,11,24 Kerr et al 13 found that men’s football and men’s wrestling have the highest rates of overall injuries. Our results demonstrated the highest rates among women’s gymnastics and women’s tennis players. The incidence of lumbar spine injuries reported to the NCAA ISP over the 2009/2010 to 2013/2014 time frame was less than that of hamstring, but greater than hip flexor, hip adductor, and quadriceps injury rates (0.35, 0.16, 0.12, and 0.10 per 1000 AEs, respectively). 3,8,9 The reported injury rates from this study suggest that there is an area for potential improvement, as they are higher than for other common collegiate athletic injuries.
Analysis by event setting demonstrated a higher number of total injuries in practice but a higher injury rate in competition. This was consistent with previous work analyzing event type for injury rates in NCAA athletes. 3 Individual men’s football, basketball, ice hockey, lacrosse, and sex-comparable sports aggregate demonstrated significantly higher competition rates of injury. Women's soccer was the only female sport to demonstrate significantly higher competition injury rates. Interestingly, women’s volleyball demonstrated the opposite trend, with both the total number of injuries and injury rate being higher during practice versus competition.
Among sex-comparable sports in our study, the rates of lumbar spine injuries were higher for women. The previous literature examining differences in injury rates between male and female athletes of the same sport is mixed. 18,22 Overall, there is a paucity of studies isolating sex as a main variable between the comparable sports, and this is a potential area for further research. Among injury mechanisms, noncontact injuries predominated. The previous literature has described higher rates of strains, noncontact injuries, and sequela of repetitive rotational movements as the causative agents in lumbar spine injuries among athletes. 7,11
Previous studies have described a relatively high risk of recurrence for lumbar spine injuries, especially among contact sports (18.3%). 10 While new injuries accounted for 78.90% of the lumbar spine injuries reported, this study also demonstrated a high risk of recurrence, with 20.73% of all injuries being classified as recurrent. Overall, this study and previous work identified prior lumbar spine injuries as a strong risk factor for future back injuries. 10
The majority of athletes in our study missed <24 hours of sports-related participation because of their injury. This knowledge that time loss extending >21 days is rare is quite valuable, as Mall et al 16 demonstrated greater time loss (mean, 25.7 days) at the professional level after back injuries. However, NCAA surveillance mechanisms and NFL surveillance mechanisms may differ. While lumbar spine injuries that required >21 days away from sport were the minority in our study (4.68%), there were still 2178 weighted estimated injuries in this category, indicating that severe lumbar spine injuries, while uncommon, do occur. This may explain why other epidemiological studies looking at all injuries by severity have back injuries classified highly in terms of time loss. 13
The majority of athletes in our study were injured during the regular season; however, the highest rates of injury occurred in the preseason. There was no significant difference between injury rates by season of play between sex-comparable sports.
Further differentiation of injuries by type demonstrated that soft tissue back sprains were the most prevalent injury mechanism, irrespective of sex differences. Previous work has demonstrated a link between poor core strength and limited endurance and an increased risk of mild low back pain without a specific osseous or ligamentous injury. 1,14 This coincides with the injury types most prevalent in our study and suggests areas for future research into preventive conditioning programs.
Limitations
Participation in the NCAA ISP is voluntary, and as such, there may be a selection bias among those programs choosing to participate during the elected study period. In addition to selection bias, there may be underreporting of injuries because of the voluntary self-reported nature of the database. This would limit the generalizability to other collegiate programs or professional programs with similarly aged players. The standardization of diagnoses and injury types reported depends on uniform diagnostic criteria among all ATs from all programs participating for this time period, which is a weakness of any multicenter data set study. The ATs reporting injuries are also confined by the NCAA ISP’s definition of an injury, which does not require imaging to make a diagnosis. Additionally, variability in team injury prevention protocols and injury reporting protocols was not considered with these data. Finally, some injuries occur infrequently and are underreported in this data set, resulting in low numbers and underpowered analysis for some sports, which again makes generalizability to professional sports or sports-related practices difficult.
Conclusion
Analysis of the NCAA ISP data demonstrated a relatively high rate of lumbar spine injuries (2.88/10,000 AEs) among collegiate athletes. Women’s gymnastics and women’s tennis had the highest rates of lumbar spine injuries. There was a higher injury rate for women in sex-comparable sports and an overall higher injury rate in competition settings, with the majority of injuries being noncontact in nature. While the majority of injuries (78.90%) were new, there was a relatively high recurrence rate (20.73%). This high rate of injury recurrence suggests that there is an area of possible further research for reconditioning programs in addition to prevention programs. This study helps to better inform athletes, trainers, and coaching staff of the risk of sports-associated lumbar disorders and injuries related to collegiate athletic participation.
Footnotes
Acknowledgment
This publication contains materials created, compiled, or produced by the Datalys Center for Sports Injury Research and Prevention on behalf of the NCAA. The NCAA ISP data were provided by the Datalys Center. The ISP was funded by the NCAA. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the Datalys Center or the NCAA.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.E.H. is a consultant for Arthrex, has received educational support from Arthrex and Smith & Nephew, has grants/grants pending from Arthrex, and has received hospitality payments from Smith & Nephew and Stryker. A.C. is a consultant for Arthrex, Zimmer Biomet, Trice Medical, and Cayenne Medical and has received educational support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Mayo Clinic.