
Abstract
Background:
Prior to the annual National Football League (NFL) Draft, the top college football prospects are evaluated by medical personnel from each team at the NFL Scouting Combine. On the basis of these evaluations, each athlete is assigned an orthopaedic grade from the medical staff of each club, which aims to predict the impact of an athlete’s injury history on his ability to participate in the NFL.
Purpose:
(1) To identify clinical predictors of signs, symptoms, and subsequent professional participation associated with football-related injuries identified at the NFL Combine and (2) to assess the methodological quality of the evidence currently published.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. We reviewed all studies that examined musculoskeletal injuries identified among athletes at the NFL Combine and associated outcomes. Data on signs, symptoms, and subsequent NFL participation were collected, and the methodological quality of the studies was assessed.
Results:
Overall, 32 studies, including 30 injury-specific studies, met the inclusion criteria. Twenty studies analyzed data collected at the NFL Combine from 2009 and later. When compared with matched controls, athletes with a history of a cervical or lumbar spine injury, rotator cuff repair, superior labrum anterior-posterior repair, anterior cruciate ligament reconstruction, full-thickness chondral lesions of the knee, or Lisfranc injury played in significantly fewer games early in their NFL careers. Additionally, athletes with a history of a cervical or lumbar spine injury, rotator cuff repair, and navicular injury had decreased career lengths versus controls. Defensive players and linemen were found to have decreased participation in the NFL for several injuries, including prior meniscectomy, anterior cruciate ligament reconstruction, and shoulder instability. Career length follow-up, measures of athletic participation, and matching criteria were highly variable among studies.
Conclusion:
For medical professionals caring for professional football athletes, this information can help guide orthopaedic grading of prospects at the NFL Combine and counseling of athletes on the potential impact of prior injuries on their professional careers. For future studies, improvements in study methodology will provide greater insight into the efficacy of current treatments and areas that require further understanding.
Each offseason, the top college football prospects are invited to attend the National Football League (NFL) Scouting Combine. This weeklong event is held prior to the NFL Draft and allows the medical staff of each NFL club to collect medical histories, perform comprehensive physical examinations, and collect imaging modalities, including plain radiographs, magnetic resonance imaging (MRI), and computed tomography as indicated. Subsequently, the medical staff of each club assigns each player an orthopaedic grade, according to its own criteria, in an attempt to predict the impact of a given history on a player’s physical durability, career longevity, and participation in the NFL. 5 This information often affects a player’s draft status, and up to 6% of players may even receive failing medical grades. 4
Since 1987, databases have been formed containing the medical information of all players evaluated at the NFL Combine. 4 Numerous retrospective studies based on these data have been published. 1,4 –6 In recent years, Provencher and colleagues have published several studies with NFL Combine data collected from 2009 to 2015, analyzing the association between specific prior injuries and outcomes in the NFL (draft position, games played, and games started during the first 2 NFL seasons). 1,8,9,22,25,28,31,32,38 These studies enable team management, scouts, coaches, physicians, and athletic trainers to better understand the impact of a given injury on a player’s participation in the NFL. More important, even beyond the NFL, such information may (1) help athletes and medical professionals better understand the ability to return to sport at a high level, (2) guide treatment options, and (3) set appropriate expectations for both parties. 6
The purpose of this systematic review was to critically evaluate the available literature on clinical predictors of outcomes relevant to musculoskeletal injuries reported or diagnosed at the NFL Scouting Combine. Specifically, we sought to (1) identify clinical predictors of signs, symptoms, and subsequent professional participation associated with football-related injuries identified at the NFL Combine and (2) assess the methodological quality of the currently published evidence.
Methods
A systematic review was conducted in July 2018 according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 20 PubMed (Medline), Embase, and the Cochrane library were searched with the terms “National Football League,” “NFL,” “combine,” “injury,” and surgery.” The search was limited to English-language articles. Titles and abstracts from these searches were independently reviewed by 2 authors (D.W., S.A.T), and full-text articles meeting the inclusion criteria were then obtained and reviewed. Additionally, the references of all included full-text articles were scanned for further eligible studies.
Inclusion criteria were established before data collection. Studies were included if they reported on musculoskeletal injuries identified among athletes at the NFL Combine and their association with clinical signs and symptoms and/or future participation in the NFL, including games played and career length. Studies were excluded if they (1) were case reports of 1 or only a few participants; (2) were epidemiologic studies that reported just the prevalence of specific injuries at the NFL Combine and did not evaluate for associations between injury and clinical signs, symptoms, or outcomes in the NFL; or (3) examined football-related injuries occurring after the NFL Combine. After elimination of duplicate articles among databases and screening of abstracts for relevance, 32 studies were analyzed (Figure 1). Thirty studies examined a cohort of athletes with a specific diagnosis or injury. All studies were retrospective, with the exception of 2 studies that prospectively collected data at the NFL Combine from a single year. 2,12

PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flowchart of the literature search process.
Two authors (D.W., M.A.) extracted the data, which were then reviewed by the coauthors. Any disagreements in data were resolved by consensus or by arbitration of a third author (L.J.W.). The tabulated data included the injury or surgery, combine years studied, number of injuries and athletes, and level of evidence. Outcomes collected included draft status, game participation data, NFL career length, and clinical assessments derived from physical examination, imaging, and functional measures related to the specific injury.
The level of evidence of the selected studies was determined according to the criteria established by the Oxford Centre for Evidence-Based Medicine. 39 As no randomized clinical trials were identified among the included studies, the MINORS criteria (methodological index for nonrandomized studies) were used to assess the methodological quality of the studies. 36 This tool has 8 criteria to assess the methodological quality of noncomparative studies and 4 additional criteria for assessing the methodological quality of comparative studies. Each criterion is scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with the global ideal score being 16 for noncomparative studies and 24 for comparative studies.
Results
Data by Injury
Of the 32 studies, 30 were injury specific. There were 2 studies on cervical spine injuries, 30,35 5 on foot injuries, 7,23,25,37,38 1 on hand injuries, 26 4 on hip/groin injuries, 14,17,18,33 9 on knee injuries, 2,8,9,13,21,22,24,31,32 3 on lumbar spine injuries, 27,29,34 and 6 on shoulder injuries. 10,11,15,16,19,28 No studies specifically examined injuries of the ankle, elbow, or long bones. Nineteen studies analyzed data collected at the NFL Combine from 2009 or later. ∥ There were 22 level 3 studies (Table 1) and 8 level 4 studies (Table 2). Based on the MINORS criteria, the mean score for methodological quality of the level 3 studies was 16.4 (range, 13-19) out of a possible 24 points. The mean score for methodological quality of the level 4 studies was 10.8 (range, 7-13) out of a possible 16 points.
Summary of Injury-Specific NFL Combine Level 3 Retrospective Studies a

a ACL, anterior cruciate ligament; ACLR, ACL reconstruction; BMI, body mass index; FAI, femoroacetabular impingement; ICRS, International Cartilage Repair Society; ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine; MCL, medial collateral ligament; MRI, magnetic resonance imaging; NA, not available; NFL, National Football League; PCL, posterior cruciate ligament; ROM, range of motion; SLAP, superior labrum anterior-posterior.
Summary of Injury-Specific NFL Combine Level 4 Studies

a ACL, anterior cruciate ligament; ACLR, ACL reconstruction; BMI, body mass index; FAI, femoroacetabular impingement; MCL, medial collateral ligament; MRI, magnetic resonance imaging; NA, not available; NFL, National Football League; PCL, posterior cruciate ligament; ROM, range of motion.
Cervical and Lumbar Spine
Athletes with a cervical spine diagnosis (including spondylosis, stenosis, sprain/strain, herniated disc, and spine spasms) were less likely to be drafted, played fewer games (Table 3), and had decreased NFL career lengths (Table 4) as compared with controls. Those with a history of multiple stinger episodes were noted on MRI to have a lower mean subaxial cervical space available for the cord, with 5.0 mm reported as the critical value. Of note, players with a cervical sagittal canal diameter <10mm did not have any significant differences in games played or performance score compared with matched controls, and no neurological injury occurred during their careers. 35
NFL Games Played Data a
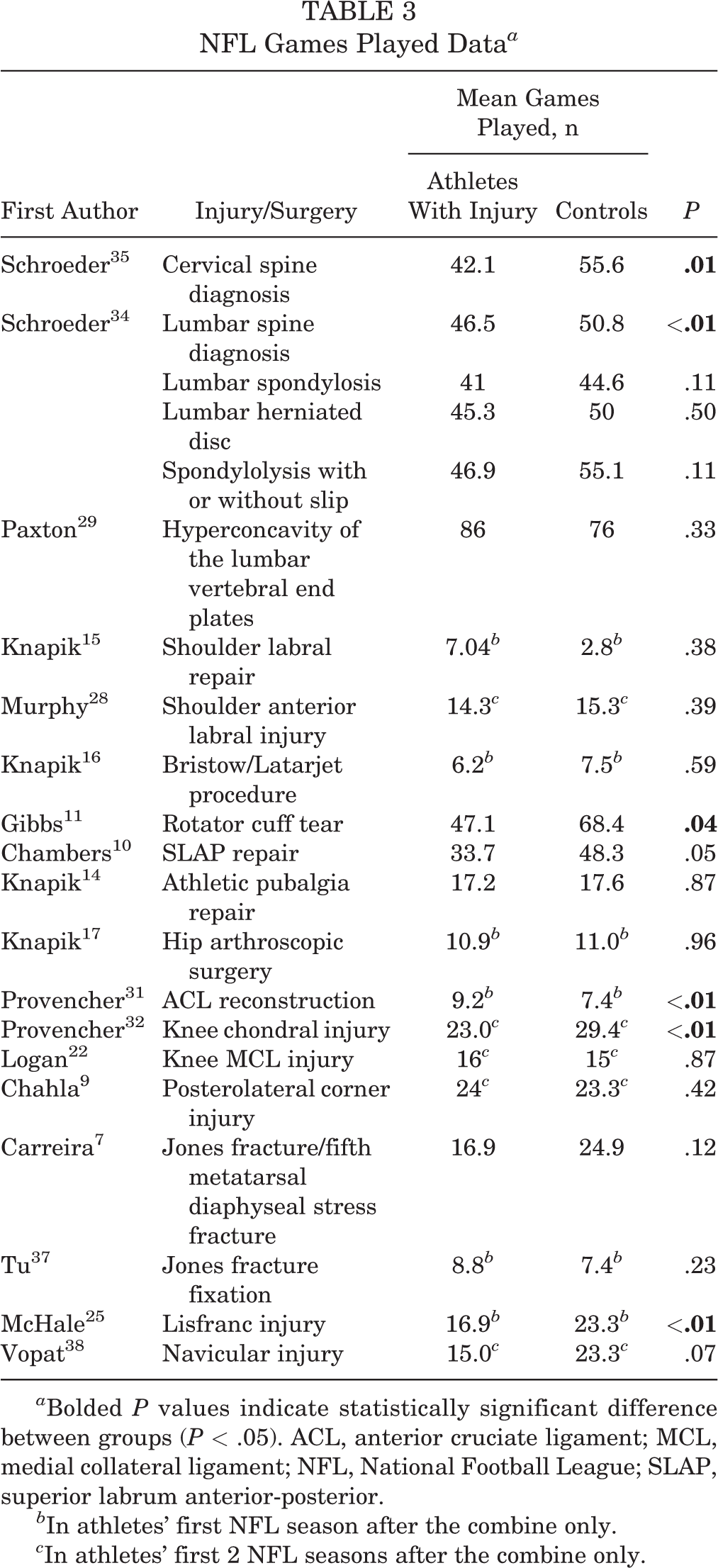
a Bolded P values indicate statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; MCL, medial collateral ligament; NFL, National Football League; SLAP, superior labrum anterior-posterior.
b In athletes’ first NFL season after the combine only.
c In athletes’ first 2 NFL seasons after the combine only.
NFL Career Length Data a
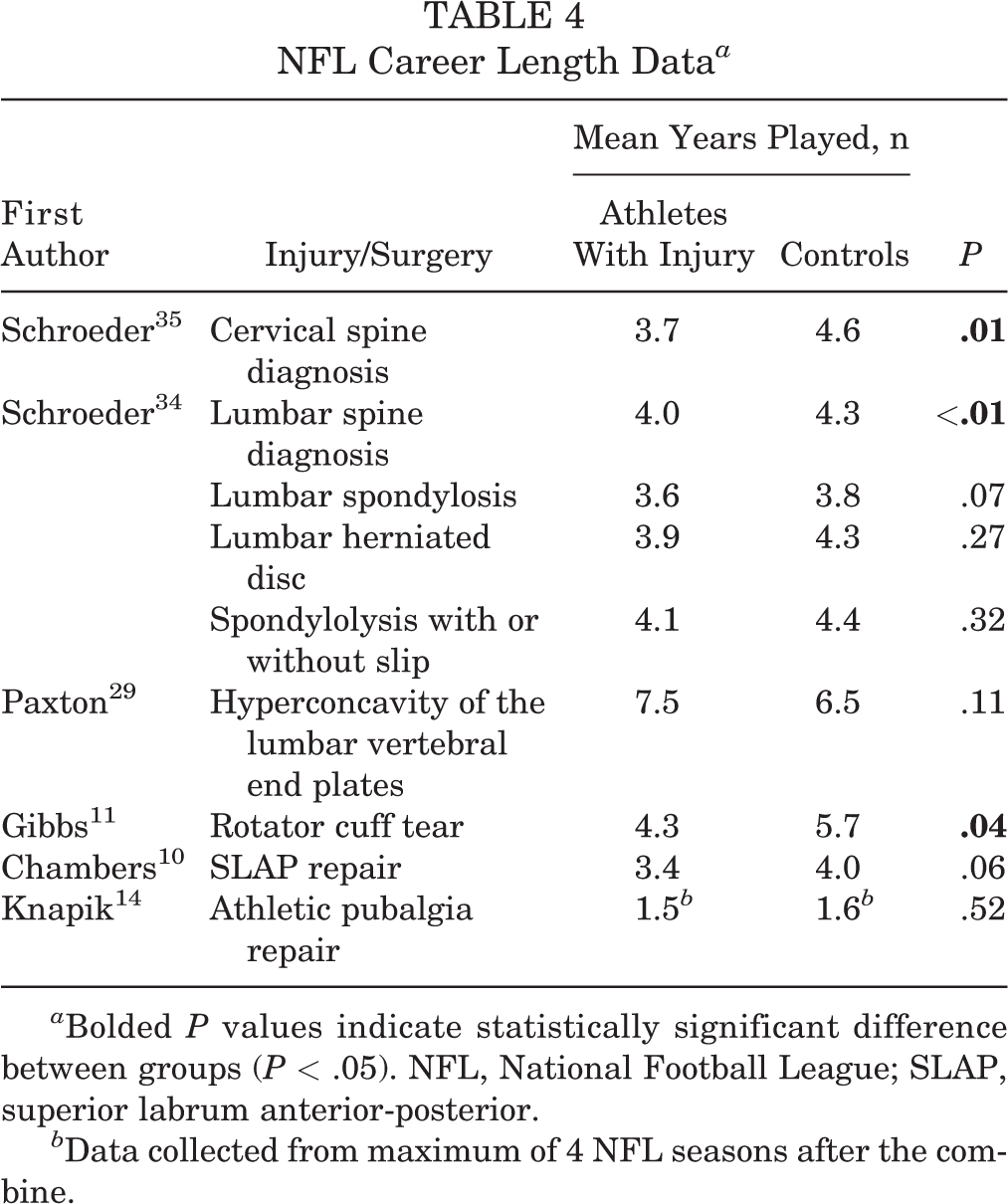
a Bolded P values indicate statistically significant difference between groups (P < .05). NFL, National Football League; SLAP, superior labrum anterior-posterior.
b Data collected from maximum of 4 NFL seasons after the combine.
Athletes with a history of a lumbar spine diagnosis (including degenerative spondylosis, herniated disc, spondylolysis, and strain) were less likely to be drafted and had a decreased number of years played, games played, and games started. Radiographic evidence of hyperconcavity of the lumbar vertebral end plates (disk space expansion) in linemen was not associated with a significant difference in career length, games played, or games started as compared with controls.
Shoulder
Two studies demonstrated that athletes with labral injuries or those who had undergone labral repair of the shoulder did not have any significant differences in draft status, games played, games started, or snap percentage when compared with controls. 15,28 Furthermore, athletes with evidence of recurrent labral tears on MRI did not have any significant differences in draft status, games played, or games started versus those with intact labral repairs. For athletes treated with bone block augmentation for shoulder instability, as many as 40% to 77% of athletes had evidence of glenohumeral arthritis on radiographs. Against controls, those who were drafted were not at significant risk for diminished participation with regard to games played or started in their first season in the NFL. In contrast, athletes with a history of a rotator cuff tear, of which 45% received operative treatment, were less likely to be drafted, played and started in fewer games, and played in fewer years versus controls. Finally, those treated with superior labrum anterior-posterior (SLAP) repair had no significant differences in draft status and performance scores as opposed to controls; however, they played and started in fewer games than healthy controls.
Hip and Pelvis
Athletes who had undergone athletic pubalgia repair or hip arthroscopic surgery did not have any significant differences in draft status, games played, or games started as compared with controls. Although the prevalence of cam- or combined-type femoroacetabular impingement and osteitis pubis was higher among symptomatic athletes, an increased alpha angle was the only independent predictor of athletic-related groin pain.
Knee
When compared with controls, athletes who had undergone anterior cruciate ligament (ACL) reconstruction were more likely to be picked lower in the draft, and they played and started fewer games in their first 2 NFL seasons. Chondral injuries of the knee were noted in 4.4% of athletes at the NFL Combine who had knee MRI because they reported prior injury or reported knee pain but had no known history of surgery; the patellofemoral joint was the most affected compartment. Athletes with chondral injuries, in the setting of no prior knee surgery or prior meniscectomy, played and started in fewer games versus controls. Specifically, subchondral bone edema and full-thickness chondral lesions were associated with fewer games played. Athletes with a history of medial collateral ligament injury or posterolateral corner knee injury did not have any significant differences in draft status, games played, or games started as opposed to respective controls.
Foot
A history of proximal fifth metatarsal fractures, including Jones fractures, was not associated with a difference in draft likelihood, games played, or games started, as compared with controls. In contrast, a history of Lisfranc or navicular injury was associated with worse draft position and fewer games played and started during the first 2 NFL seasons. In addition, a prior navicular injury was associated with significantly decreased probability of playing ≥2 years in the NFL.
Data by Position
Two level 3 studies specifically examined injuries identified at the NFL Combine and their impact on NFL participation by player position. 1,6 Based on the MINORS criteria, the mean score for methodological quality of these studies was 17 (range, 16-18) out of a possible 24 points. NFL participation data by athlete position are summarized in Table 5. Game participation appears to be affected by injuries most in offensive and defensive linemen and defensive backs. Of note, spondylolisthesis was not significantly associated with a reduced percentage of athletes playing in the league or a shorter career length at any position.
NFL Participation Data by Athlete Position a

a ACLR, anterior cruciate ligament reconstruction; NFL, National Football League.
b In first 2 NFL seasons after the combine only.
Discussion
When compared with matched controls, athletes with a history of a cervical or lumbar spine injury, rotator cuff repair, SLAP repair, ACL reconstruction, full-thickness chondral lesions of the knee, or Lisfranc injury played in significantly fewer games early in their NFL careers. Additionally, athletes with a history of a cervical or lumbar spine injury, rotator cuff repair, or navicular injury had decreased career length versus controls. The potential impact of these injuries seems to vary by player position as well, with defensive players and offensive and defensive linemen having decreased participation in the NFL for several injuries, including prior meniscectomy, ACL reconstruction, and shoulder instability (Figure 2). Nevertheless, the available literature remains highly variable with regard to length of follow-up, matching criteria, measures of participation outcomes, and overall methodological quality.

Summary of NFL participation data sorted by injury identified at the NFL Combine. ACLR, anterior cruciate ligament reconstruction; ICRS, International Cartilage Repair Society; MCL, medial collateral ligament; NFL, National Football League; PCL, posterior cruciate ligament; PLC, posterolateral corner; SLAP, superior labrum anterior-posterior.
Using NFL Combine data collected by 1 team from 1987 to 2000, Brophy et al 5 examined the correlation between orthopaedic grade and career longevity in the NFL. Players with a high grade (no injury, minor injury, or successful surgical interventions) had a mean career of 42 games, as opposed to 34 games for players with a low grade (incomplete recovery and/or injury likely to recur) and 19 games for players with a failed grade. Thus, assigning orthopaedic grades to college football prospects based on their injury history has historically been a useful practice for predicting career longevity in the NFL. Of note, we found an increasing trend of likelihood of playing in the NFL for players treated with ACL reconstruction or shoulder stabilization over the study period, likely reflecting the improved understanding of these injuries and advancements in surgical technique and rehabilitation. As a result, over time, fewer players received failed grades at the combine.
Although recent NFL Combine studies have improved a medical professional’s ability to predict the impact of a prior injury on a player’s professional career, there is a dearth of studies examining athletes with a history of hand, elbow, long bone, and ankle injuries. Although hand and ankle injuries are among the most commonly identified injuries at the NFL Combine, 1,4 this review found only 1 study on hand injuries and no studies on ankle injuries. Furthermore, while the lone hand study examined the clinical and radiographic outcomes of scaphoid fracture, it did not assess NFL participation metrics. 26
Moreover, future studies utilizing more rigorous methodology would allow medical professionals to provide more accurate predictions of a prior injury’s impact on an athlete’s NFL career. Currently available studies on injuries of the cervical spine or lumbar spine classify all spine diagnoses together in their analyses, resulting in heterogeneous cohorts. These aggregated diagnoses, which included stinger, spondylosis, stenosis, spondylolysis, and sprain/strain, are all unique pathologies that have different symptoms and prognoses. Although the studies by Schroeder et al 34,35 found that athletes with a cervical or lumbar spine diagnosis were less likely to be drafted and played in fewer games than controls, diagnoses of strain, scoliosis, and spasms were included in relatively fewer numbers when compared with the more severe diagnoses of spondylosis, spondylolysis, herniated disc, and stenosis. Future studies examining a more focused cohort of spine diagnoses are needed.
Additionally, measurement of draft status, games played and started, snap percentage, and game performance metrics are influenced by a multitude of factors (eg, player position, team needs, opponent game plan, depth chart), which can ultimately confound the results. Many currently available studies do not account for these factors. For instance, with regard to player position, drafted quarterbacks often do not play in any games during the first few years of their professional career, owing to their position on the depth chart, whereas kickers often go undrafted but are signed by teams and play during their rookie years. Several studies utilizing a matched control group did not match per player position. 14,17,29,30,32,37 Some players are made inactive on game day despite being healthy and participating in practice. Therefore, measurement of games played or games started may not accurately represent the degree of professional athletic participation. Metrics such as athlete exposures, which accounts for practice participation, or days on the “physically unable to perform”–injured reserve list would better characterize athletic participation. Finally, missed time caused by reinjury to the previously injured anatomic area is more likely to be indicative of the impact of a specific prior injury on participation in the NFL.
Other limitations of this qualitative review are related to the level and availability of evidence reviewed. The majority of the studies reviewed were retrospective and used injury data that were self-reported or derived from scouting, introducing recall bias. Instead of using the NFL Injury Surveillance System, some studies used publicly accessible websites to collect participation and performance data, for which their accuracy or completeness cannot be verified. The majority of studies that measured participation or performance analyzed data within only the first 1 or 2 NFL years after the combine. 1,8,9,22,25,28,31,32,38 Analysis of outcomes within the first 4 to 5 years, which is the length of the typical rookie contract, may be more valuable from an administrative perspective. The impact of injuries within an anatomic region may not be mutually exclusive to the same region; for instance, limited hip rotation and femoroacetabular impingement have been linked to risk of ACL injury. 2,3 Finally, there is inherent selection bias in the analyzed studies, since athletes who were invited to the combine likely had successful outcomes after their injuries. These studies did not include athletes who were not invited to the combine but still made it to the professional level. Therefore, these findings cannot necessarily be extrapolated to the average collegiate football athlete, nor can they necessarily be extrapolated to high school or younger athletes, owing to the higher demands that are placed on the musculoskeletal system in the NFL.
Conclusion
NFL prospects with a history of a cervical or lumbar spine injury, rotator cuff repair, SLAP repair, ACL reconstruction, full-thickness chondral lesions of the knee, or Lisfranc injury played in significantly fewer games early in their NFL careers. Game participation was also dependent on player position, with defensive players and offensive and defensive linemen having decreased participation for several injuries. For medical professionals caring for professional football athletes, this information can help guide orthopaedic grading of prospects at the NFL Combine and counseling of athletes on the potential impact of prior injuries on their professional careers. For future studies, improvements in study methodology—including longer career follow-up, more accurate measures of athletic participation, more robust and consistent matching criteria, separate investigation of specific spine diagnoses, and prospective designs—will provide greater insight into the efficacy of current treatments and areas that require further understanding.