
Abstract
Background:
Patient-reported outcome (PRO) measures are progressively utilized as evaluation tools in preoperative and postoperative assessments in orthopaedic practice. Identifying the potential utility of psychosocial factors to predict patient-reported pain and functional outcomes is of increasing interest to determine which patients will derive the greatest benefit from surgical treatment.
Purpose/Hypothesis:
The purpose of this study was to determine potential predictive associations between the preoperative 12-Item Short Form Health Survey Mental Component Summary (SF-12 MCS) score, patient characteristics or osteochondral allograft (OCA) morphology, and PROs in patients who underwent OCA transplantation. We hypothesized that poor preoperative mental health is associated with diminished PROs at final follow-up.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 67 patients with a mean follow-up of 2.7 ± 1.0 years (range, 2-6 years) with complete preoperative and at least 24-month postoperative SF-12 MCS, Knee injury and Osteoarthritis Outcome Score (KOOS), Tegner, Lysholm, and International Knee Documentation Committee (IKDC) scores were included in this study. Pearson correlation coefficients and linear regression models were used to distinguish associations between age, sex, smoking status, body mass index, workers’ compensation, previous surgery, concomitant surgery, number of grafts, defect location, total graft size, SF-12 MCS score, and postoperative PRO scores as well as their improvement from baseline (delta).
Results:
The SF-12 MCS showed significant correlation with the KOOS Activities of Daily Living subscale (P = .015), KOOS Sport/Recreation subscale (P = .024), and IKDC (P = .039). In the multivariable linear regression models, the SF-12 MCS had no predictive association with any PRO measure. Patient sex contributed significantly to the final regression models of the KOOS Sport/Recreation (P = .042), Tegner score (P = .024), and Lysholm score (P = .031). The SF-12 MCS showed no bivariate correlation with changes in any PRO score (delta) (P > .05).
Conclusion:
Preoperative mental health status did not predict perceived functional outcomes as assessed by PRO measures at final follow-up. Female sex was negatively correlated with KOOS Sport/Recreation, Tegner, and Lysholm scores.
Keywords
Osteochondral allograft (OCA) transplantation has gained popularity over the past 15 years as a viable treatment option for osteochondral lesions of the knee. 25 Initially indicated as a salvage procedure after previously failed cartilage repair such as autologous chondrocyte implantation (ACI) or microfracture, 8,16 OCA transplantation is increasingly performed as a primary procedure for large osteochondral defects, showing excellent clinical outcomes. 15,18,42 However, factors such as age, low activity level, body mass index (BMI) >35 kg/m2, osteoarthritis, steroid-induced osteonecrosis, multiple previous surgeries, kissing lesions, patellofemoral defects, and prolonged graft storage time are associated with less favorable results. 1,8,14,22,24,28,37
Patient-reported outcome (PRO) measures are progressively utilized in orthopaedic practice to determine success and inform preoperative decision making and surgical indications. The Knee injury and Osteoarthritis Outcome Score (KOOS) is a widely used self-assessed tool to evaluate patient outcomes at short- and long-term follow-up. It assesses 5 separate domains: Pain, Symptoms, Activities of Daily Living (ADL), Sport/Recreation, and Quality of Life (QOL). 32 Previous studies have validated the KOOS as a reliable tool in evaluating patients undergoing cartilage repair, including OCA transplantation. 4,10,11,15
Identifying the potential utility of psychosocial factors to predict patient-reported pain and functional outcomes is of increasing interest to determine which patients will derive the greatest benefit from surgical treatment. Several studies have reported that low preoperative patient mental health can contribute to poor postoperative outcomes among a variety of orthopaedic specialties such as trauma, spine, hand, and upper extremity surgery. # Depression and anxiety have been shown to correlate with worsening pain in patients with osteoarthritis. 19,33,34 Kim et al 19 reported that the presence of a depressive disorder is associated with an increased risk of symptomatic osteoarthritis in patients with minimal to moderate radiographic changes. Similarly, increased postoperative pain, low levels of satisfaction, and unfavorable clinical outcomes can be expected in mentally depressed patients after anterior cruciate ligament reconstruction or total knee arthroplasty. 13,17,41 However, there is a relative paucity of literature investigating the relationship among preoperative mental health, objective abnormalities, and PROs in patients who undergo cartilage repair with an OCA.
Given the uncertain predictive value of preoperative mental health on self-reported outcome scores in patients treated with OCA transplantation for osteochondral lesions of the knee, this study sought to determine the role of psychological factors on patient-reported pain and functional outcomes in patients after OCA transplantation. We hypothesized that poor preoperative mental health, as measured with the 12-Item Short Form Health Survey Mental Component Summary (SF-12 MCS), is associated with diminished KOOS scores at a minimum follow-up of 24 months.
Methods
Our institution prospectively collects data for all patients undergoing cartilage repair. Patients who underwent cartilage repair with an OCA for focal osteochondral defects in the knee by a single surgeon between March 2011 and April 2016 were enrolled for this retrospective study of prospectively collected data. Our institutional review board approved the study before initiation. Exclusion criteria included patients with incomplete preoperative or postoperative self-assessments at 1-year follow-up as described below, as well as incomplete patient demographic data or unreported OCA plug size, location, and number.
Each patient enrolled in this study completed preoperative and postoperative SF-12 MCS, KOOS, Tegner, Lysholm, and International Knee Documentation Committee (IKDC) surveys. The SF-12 is a 12-item questionnaire that assesses specific factors of general health-related quality of life, which is divided into the Physical Component Summary and the MCS. The general population has a mean score of 50 ± 10, and a higher score demonstrates better health-related quality of life. 30,40 Each of the 5 KOOS subscales are scored individually from 0 (extreme knee problems) to 100 (no knee problems).
We recorded each patient’s age at the time of surgery, BMI, sex, smoking status, workers’ compensation status, previous surgery on the index knee, and concomitant surgery such as osteotomy, ligamentous repair/reconstruction, and meniscal allograft transplantation. OCA graft characteristics, including the size, number, and location, were collected from surgical notes.
Statistical analysis was performed utilizing descriptive statistics, bivariate correlations, and univariable and multivariable linear regression models. Descriptive statistics were calculated to determine the sociodemographic and clinical characteristics of patients. Bivariate correlations were assessed by Pearson correlation coefficients (r). Categorical variables were coded as dummy variables for univariable and multivariable linear regression models (ie, for sex, 0 represented male and 1 represented female). Models included patient age, sex, BMI, concomitant surgery, previous surgery, workers’, compensation status; compensation status, smoking status, SF-12 MCS score, baseline scores, and OCA plug number, size, and location. For each regression model, potential predictor variables were first evaluated univariably using one of the PRO measures (KOOS subscales, Tegner, Lysholm, or IKDC) as a dependent variable. Associations displaying significance at P < .1 were included in a multivariable regression model to adjust for covariates. All statistical analyses were performed with SPSS for Mac (version 23.0; IBM). With a sample size of 67 patients, the study was adequately powered to detect the predictive value of included variables in the bivariable and multivariable linear regression models with a moderate effect (Cohen d of 0.3) and a power of more than 0.8 at a level of significance of .05. 7
Results
The senior author (A.H.G.) treated a total of 134 patients with OCA transplantation for focal symptomatic osteochondral lesions within the knee joint during the study period. Of these patients, 67 were excluded from this study because 28 (20.9%) did not complete preoperative self-assessments and 39 (29.1%) completed preoperative but not postoperative self-reported outcome measures at minimum 24-month follow-up. Table 1 presents patient characteristics and preoperative outcome scores for included and excluded patients. Hence, 67 patients with complete preoperative and postoperative PROs were included after fresh OCA transplantation for cartilage defects of the knee by the senior author. The mean age was 35.0 ± 10.0 years (range, 16-54 years), with a mean BMI of 26.8 ± 4.7 kg/m2 (range, 18.8-37.4 kg/m2) and a mean follow-up of 2.7 ± 1.0 years (range, 2-6 years). Overall, 37 patients (55.2%) were female, 5 (7.5%) were active smokers, 2 (3%) had workers’ compensation, 24 (35.8%) underwent concomitant osteotomy, 2 (3%) underwent concomitant meniscal allograft transplantation, and 1 (1.5%) underwent concomitant medial patellofemoral ligament reconstruction; 38 (56.7%) had undergone previous surgery on their index knee.
Patient Characteristics and Preoperative Patient-Reported Outcome Scores a
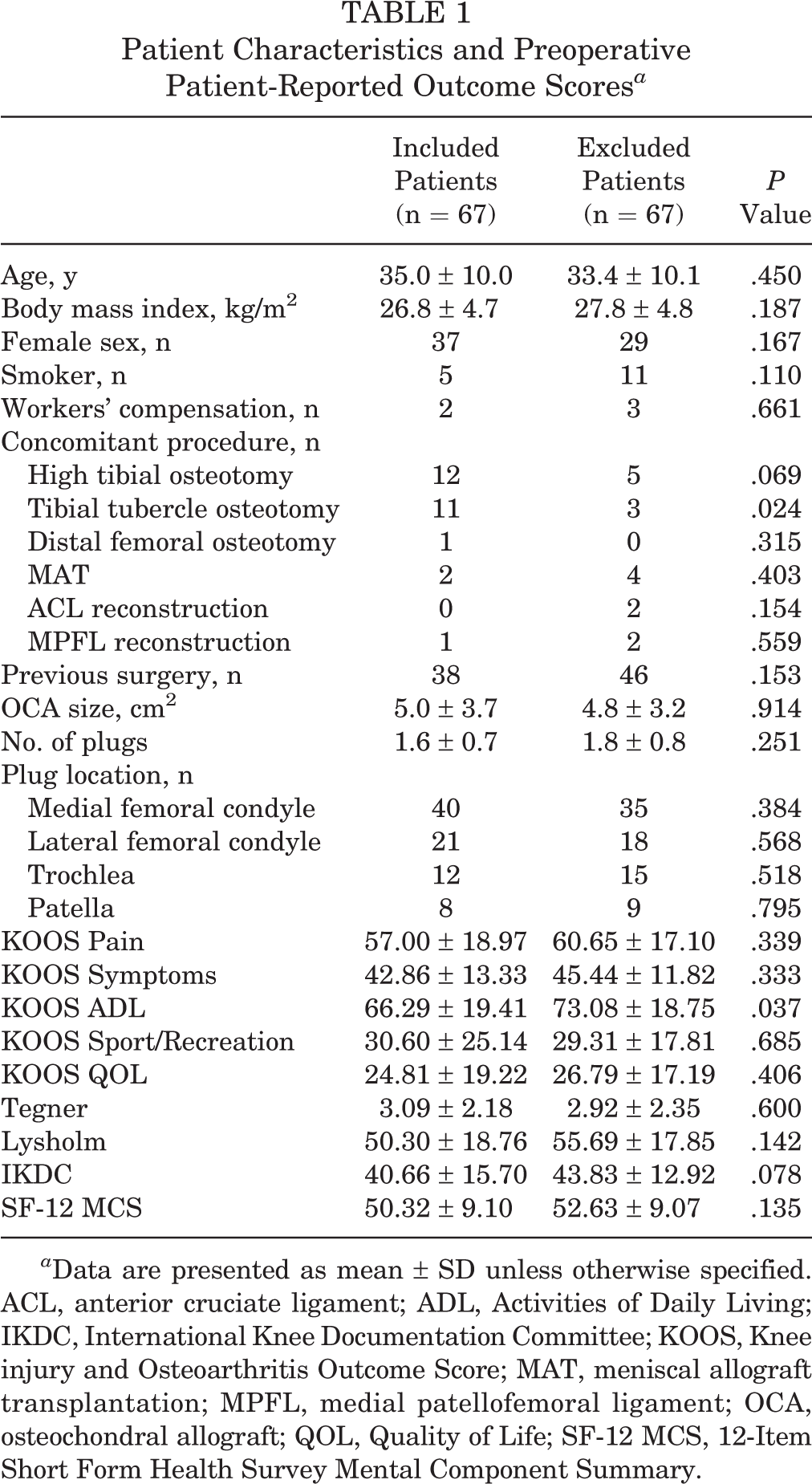
a Data are presented as mean ± SD unless otherwise specified. ACL, anterior cruciate ligament; ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; QOL, Quality of Life; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Concomitant osteotomies included 12 high tibial osteotomies, 11 tibial tubercle osteotomies, and 1 distal femoral osteotomy. The combined size of all implanted OCA grafts per patient averaged 5.0 ± 3.7 cm2 (range, 0.8-17.9 cm2). The number of OCA grafts ranged from 1 to 4, with 53.7% of patients treated with 1 plug, 35.8% with 2 plugs, 9.0% with 3 plugs, and 1.5% with 4 plugs. A total of 40 patients (59.7%) had at least 1 OCA plug implanted in the medial femoral condyle, 21 patients (31.3%) in the lateral femoral condyle, 12 patients (17.9%) in the trochlea, and 8 patients (11.9%) in the patella. The total outcome score and improvement (delta) in scores for all patient-reported surveys are presented in Table 2.
Postoperative Patient-Reported Outcome Scores and Improvement in Scores a
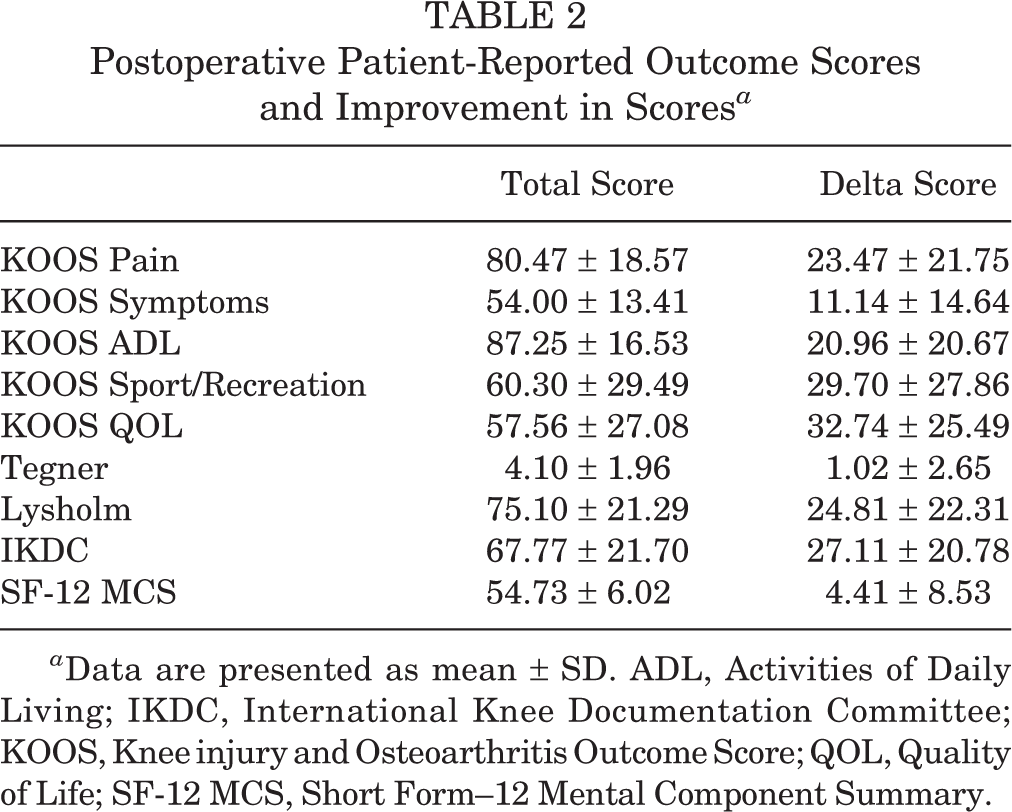
a Data are presented as mean ± SD. ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SF-12 MCS, Short Form–12 Mental Component Summary.
The SF-12 MCS showed a significant association at P < .1 with the KOOS Pain and the Lysholm score and at P < .05 with the KOOS ADL, KOOS Sport/Recreation, and IKDC (Tables 2 –9). At final follow-up, the Tegner score was the only measure that correlated most significantly not with its own preoperative baseline score but with patient sex (P = .024) (Table 8).
Univariable and Multivariable Linear Regression Models for KOOS Pain a
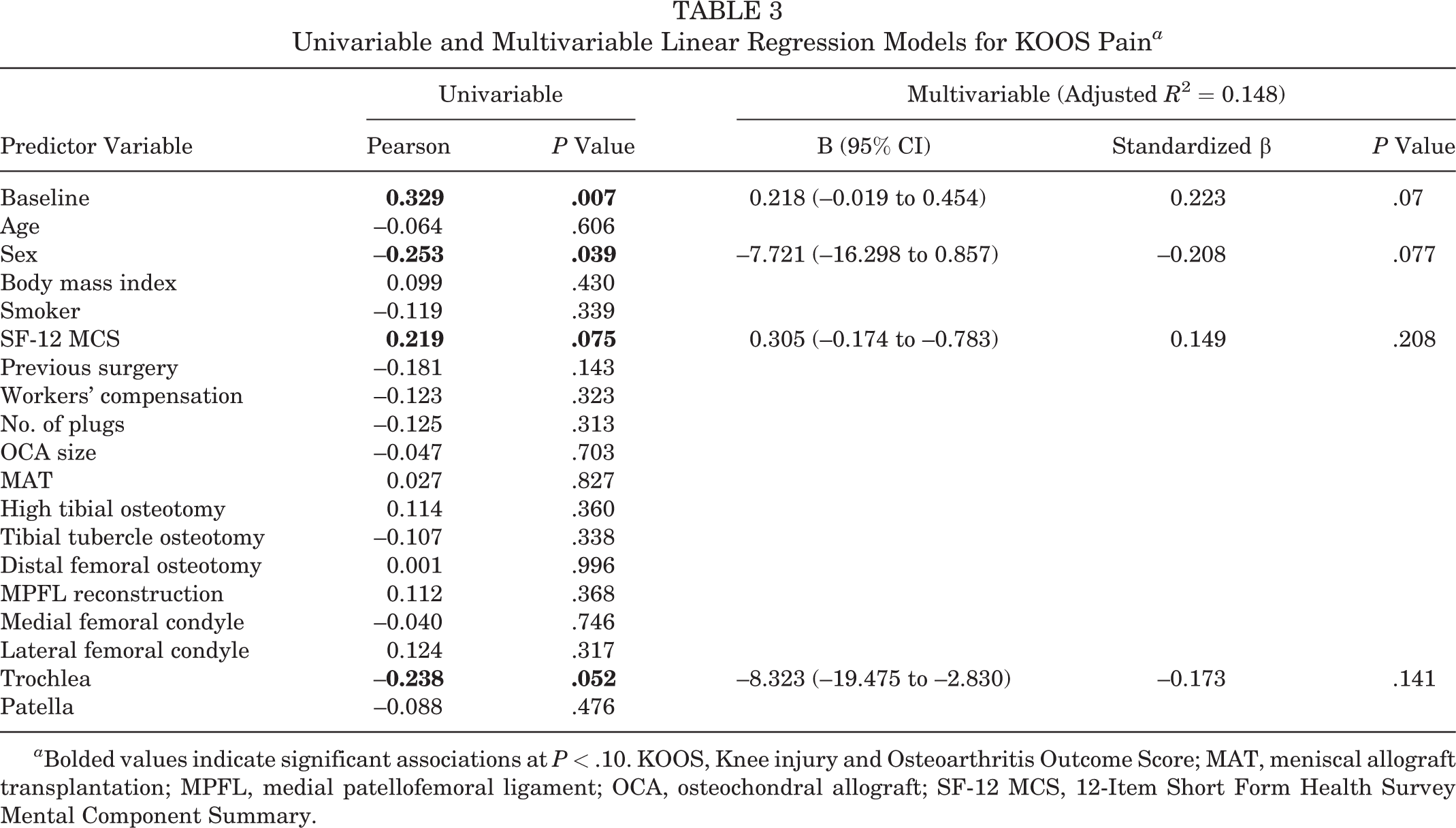
a Bolded values indicate significant associations at P < .10. KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for KOOS Symptoms a

a Bolded values indicate significant associations at P < .10. KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for KOOS Activities of Daily Living a

a Bolded values indicate significant associations at P < .10. KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for KOOS Sport/Recreation a
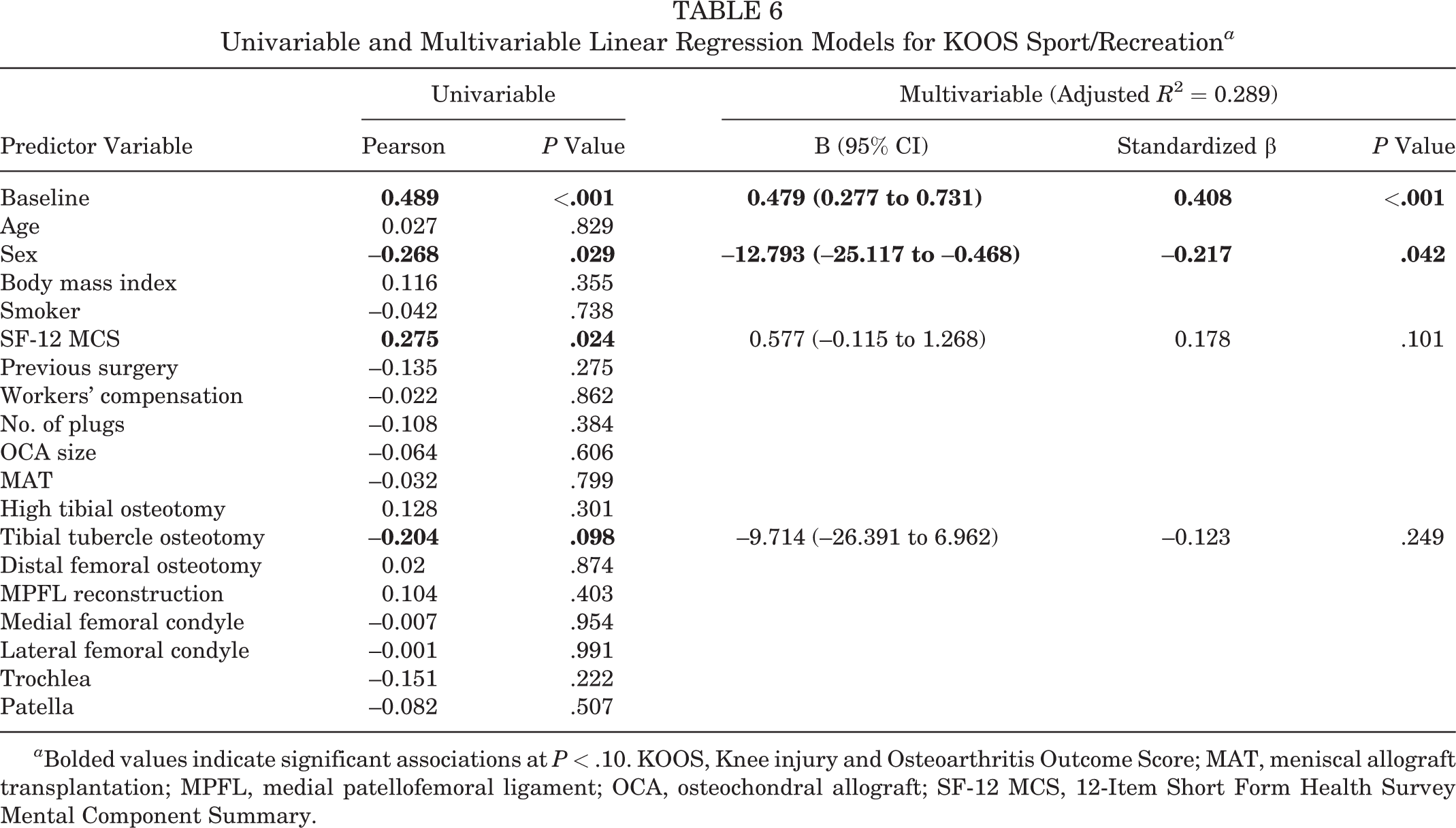
a Bolded values indicate significant associations at P < .10. KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for KOOS Quality of Life a

a Bolded values indicate significant associations at P < .10. KOOS, Knee injury and Osteoarthritis Outcome Score; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for Tegner Score a

a Bolded values indicate significant associations at P < .10. MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable and Multivariable Linear Regression Models for Lysholm Score a

a Bolded values indicate significant associations at P < .10. MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
In the multivariable linear regression models, the SF-12 MCS had no association with any of the PRO measures. The postoperative KOOS Pain score was not significantly predicted by any of the independent variables (P > .05) (Table 3). The postoperative KOOS Symptoms, KOOS QOL, and IKDC scores were significantly associated with only their preoperative baseline score (all P < .05) (Tables 4, 7, and 10). Aside from their own preoperative baseline scores, the KOOS ADL was also significantly predicted by whether a plug was implanted in the trochlea (P = .024) (Table 5), and the KOOS Sport/Recreation was also associated with patient sex (P = .042) (Table 6). Also, patient sex (P = .031) and whether a patient underwent previous surgery on the index knee (P = .023) contributed significantly to the linear regression model of the Lysholm score (Table 9). The Tegner score was predicted only by patient sex (P = .024) (Table 8). The SF-12 MCS showed no correlation with changes in any of the PRO scores (delta) at final follow-up (Table 11).
Univariable and Multivariable Linear Regression Models for IKDC a

a Bolded values indicate significant associations at P < .10. IKDC, International Knee Documentation Committee; MAT, meniscal allograft transplantation; MPFL, medial patellofemoral ligament; OCA, osteochondral allograft; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Univariable Regression of Preoperative SF-12 MCS Score and Improvement (Delta) in Patient-Reported Outcome Scores at Final Follow-up a

a ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SF-12 MCS, 12-Item Short Form Health Survey Mental Component Summary.
Discussion
This is the first report to evaluate the potential influence of a patient's preoperative mental health on outcome scores after treatment with an OCA for symptomatic osteochondral lesions in the knee. The key finding of this study was that preoperative mental health demonstrated no predictive value for postoperative KOOS, Tegner, Lysholm, or IKDC scores or the change in these scores from preoperatively to postoperatively at final follow-up.
Several prior studies across various orthopaedic subspecialties have demonstrated an association between mental health and preoperative and postoperative pain, satisfaction, and outcomes.** Accordingly, it has been suggested to include a preoperative mental health assessment in patient consultations, as it may provide useful prognostic information in patients with osteoarthritis undergoing arthroplasty. 2,21
Interestingly, this did not prove to be the case for patients undergoing OCA transplantation. When adjusted for covariates, no correlation was observed between the preoperative SF-12 MCS score and patient responses to surgery at a minimum of 24 months, as shown by both absolute PRO scores and the change in PRO scores. Patients undergoing cartilage repair are generally younger, with less medical comorbidities, a lower BMI, and a higher level of activity than patients with advanced osteoarthritis who are candidates for total joint arthroplasty. However, when compared with similar populations treated with other cartilage repair procedures, several studies investigating patients who underwent ACI for the treatment of cartilage defects showed a significant influence of preoperative mental health on postoperative functional scores. 3,9 The generally reported shorter time of recovery and easier rehabilitation in patients after OCA transplantation than ACI may explain this observed difference between our results and theirs. Because compliance with rehabilitation and a patient’s mental health are likely related, 5 ACI may require better preoperative mental health than OCA transplantation to attain good compliance with the longer and more involved postoperative course to achieve better postoperative function. Thus, while not ultimately providing predictive value for clinical outcomes after OCA transplantation, these findings may be important for preoperative counseling and choosing an appropriate treatment option among different cartilage repair procedures. Accordingly, we agree with Bartlett et al 3 in suggesting a preoperative psychological assessment in patients undergoing cartilage repair.
We also did not find significant associations between graft size and any postoperative PRO score (all P > .05). In fact, none of the patient- or lesion-associated parameters contributed significantly to the regression model of the KOOS Pain. This finding is in accordance with the results of a recently published study by Tirico and colleagues 36 in which the authors concluded that the size of the lesion had no influence on clinical outcomes in patients after OCA transplantation. While showing that patient sex has significant predictive value for postoperative KOOS Sport/Recreation, Tegner, and Lysholm scores, this study, in contrast to previous studies, 1,12,22,27 did not find any predictive value of patient age, BMI, OCA size, or patellar lesions for clinical outcomes at a minimum follow-up of 24 months.
This study is not without limitations. It is a retrospective review of prospectively collected data, and the study group was relatively small and represented only 50% of the eligible population. As shown in Table 1, however, it can be assumed that the study population is representative of the entire eligible population. Also, presenting to a tertiary referral center for cartilage repair, patients in this study had relatively large or multiple cartilage defects. Thus, it cannot be excluded that the observations may not apply to patients with smaller defects.
Conclusion
In patients undergoing OCA transplantation for cartilage injuries of the knee, preoperative mental health status did not predict perceived functional outcomes as assessed by PRO measures at a final follow-up of at least 24 months. Given the disparity in our findings between OCA transplantation and previous reports on other cartilage repair options, it is advisable to include preoperative mental health as one of the many factors involved in the informed decision-making process between the patient and physician to select the most appropriate cartilage repair procedure.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.A.D. has received educational support from Mid-Atlantic Surgical, Arthrex, and Kairos Surgical. A.H.G. receives research support from JRF; is a consultant for JRF, Aesculap Biologics, Sanofi-Aventis, Geistlich Pharma, Genzyme, Aastrom Biosciences, and Smith & Nephew; has received hospitality payments from LifeNet Health, Fidia Pharma, and Stryker; and has received honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners HealthCare.