
Abstract
Background:
Artificial ligaments have been developed and used in the treatment of ligamentous injuries since the 1970s. The early generation of artificial ligaments showed promising short-term results but resulted in high rates of rupture and inflammatory reaction in the surrounding tissues.
Purpose:
To determine whether the use of Ligament Augmentation and Reconstruction System (LARS) ligaments is associated with the development of intra-articular foreign body reaction.
Study Design:
Case series; Level of evidence, 4.
Methods:
LARS ligaments were explanted from 15 patients under 6 consultant orthopaedic surgeons at 8 surgical centers. Of these, 14 explanted samples were sent for macroscopic and histological analysis, with the 1 remaining sample sent for scanning electron microscopy, to assess for inflammatory change as well as the degree of fibrous tissue ingrowth.
Results:
We observed a foreign body reaction in 10 of 14 explanted LARS ligaments. Seven samples demonstrated fibrous tissue ingrowth, with 5 producing only focal or incomplete ingrowth. The 2 samples with extensive fibrous coverage were completely free of any foreign body reaction, while all 5 remaining samples with only focal or partial fibrous ingrowth were associated with at least some degree of harmful immune response.
Conclusion:
The LARS ligament is still associated with a clinically significant degree of foreign body reaction despite the LARS Company’s efforts to reduce complications through improved design. The development and completion of fibrous tissue ingrowth may work to reduce the occurrence of a foreign body reaction.
Artificial ligaments have been developed and used in the treatment of ligamentous injuries since the 1970s. Prior to their implementation, autologous tendons and allografts were the most popular methods of managing these conditions; however, the risk of donor site morbidity, weakening of adjacent anatomic tissues, and the transmission of diseases in an era stricken with fear of hepatitis and HIV made the use of artificial grafts increasingly attractive. 7 The long rehabilitation period of natural grafts also drove the development of new artificial substitutes with their early rehabilitation results and faster return to activity, giving them some advantage over biological alternatives. 7
The early generation of artificial ligaments comprised materials such as polytetrafluorethylene and carbon, as used in the Gore-Tex and Proplast prostheses, respectively, during the mid-1970s and polypropylene, as used in the Polyflex ligaments—all of which resulted in high rates of rupture and inflammatory reaction in the surrounding tissues. 7 Later prostheses were developed with a variety of materials, such as polyester (Dacron, PRO-FLEX) and polypropylene (Kennedy LAD). These prostheses, too, showed promising short-term results; however, all were reported to exhibit signs of synovial foreign body reactions in the surrounding tissues. Mechanical failure contributed to the presence of abrasion, wear debris, and bone tunnel enlargement, with numerous cases of rupture and lack of tissue ingrowth also contributing to their poor long-term success. 4,5,7
Chronic synovitis is one of the most significant long-term complications that has been reported for artificial ligaments. 1 –5,7,8,11,12 It is a condition characterized by prolonged inflammation of the synovial membrane and articular cartilage by plastic exudation and fibrous tissue formation, resulting in joint dysfunction and effusion. In the context of ligament reconstruction with artificial prostheses, it represents a long-term immunological response to a foreign agent, leading to adverse symptoms such as pain and reduced mobility and range of motion, as well as predisposing the patient to greater risk of osteoarthritis and the need for subsequent surgical procedures. Its association with the use of artificial ligaments has been attributed to a foreign body response to the implanted prosthesis itself, as well as to the development of wear debris produced by friction between the artificial ligament fibers and bony surfaces. 4,7,10
With the advent of new materials and techniques, most recent artificial ligaments provide a more anatomic design, promote new tissue ingrowth, and minimize the occurrence of a foreign body reaction. 1,4,7,8,11,12 One such prosthesis that claims to fulfill these criteria is the Ligament Augmentation and Reconstruction System (LARS) ligament developed by J.P. Laboureau (Surgical Implants and Devices). It consists of numerous fibers of polyethylene terephthalate arranged in a manner that mimics the native ligament. 6 The extra-articular segment consists of longitudinal fibers bound by a transverse knitted structure designed to provide strength and resist elongation, with the intra-articular segment consisting of multiple parallel longitudinal fibers twisted at 90° angles designed to resist fatigue and allow fibroblastic ingrowth. 5,6 The LARS Company has worked to optimize its ligaments and now believes that these prostheses are inert, do not produce any foreign body reaction, and hence are not directly responsible for any acute or chronic aseptic synovitis. 10,11
In the past, the LARS ligament was deemed responsible for numerous cases of acute aseptic synovitis, which was attributed to the cytotoxic chemicals used in the production of the prosthesis. 3,9,11 More recently, the LARS Company has refined its production techniques so that the cytotoxic chemicals used in the sizing process are completely removed during production, thus preventing any foreign body reaction. In addition, the ligament’s biocompatibility has been enhanced by improving the microporosity of the ligament to promote faster fibroblastic ingrowth and to prevent the production and release of wear debris into the joint.
Recently there has been increasing interest in the use of artificial ligaments, especially in the context of elite athletes having returned early to professional sport, with the accompanying media attention. This in turn has led to the increased use of artificial ligaments for athletes as well as for active patients wishing to return to their previous levels of activity quickly. As the popularity of artificial ligaments grows, the clinician needs to be aware of the ongoing risks associated with their use, even as technology and their design improve. As such, we present our experience with explanted ligaments sent for analysis and report on the histological response as a function of implantation time and common reasons for failure.
Methods
Harvesting of Prostheses
The LARS ligament samples were explanted from 15 patients by 6 consultant orthopaedic surgeons. All ligaments examined were implanted between 2009 and 2014, with time of explantation between 2010 and 2016. The indications for removal of the prostheses included joint instability on examination (n = 8), clinical synovitis (n = 1), trauma (n = 1), late-stage infection (n = 1), prosthetic loosening and rupture (n = 3), as well as total knee arthroplasty of the ipsilateral knee (n = 1). The implants were sent in the same condition at removal to the Centre for Implant Technology and Retrieval Analysis, Royal Perth Hospital, per the standard protocol for all retrieved devices. In summary, retrieved devices are placed in 10% formaldehyde solution in theater and sealed for transport to the center. All devices are accompanied with detailed retrieval notes as completed by the consultant surgeon. After initial triage, 14 ligaments were photographed and sections sent for histological analysis (samples 1-14). The remaining sample (sample 15) was of insufficient quantity for histological analysis and so was sent for scanning electron microscopy (SEM).
Histological Study
Given the nature of the synthetic material admixed with human tissue, the sections taken from each LARS ligament were placed on positively charged microscope slides to aid with adhesion. The fixing and processing of each sample, done over a minimum of 6 hours, were performed on a Leica ASP 300 Enclosed Tissue Processor (Leica Biosystems) with 4 μm–thick sections before being stained with hematoxylin and eosin via a set protocol with a DAKO Autostainer (Aligent Technologies). Once the histological staining process was completed, each section was examined by a consultant pathologist (J.P.) and assessed for degree of fibrous tissue ingrowth, as well as for the presence of a foreign body reaction.
Macroscopic Observations and Microscopy
Ligaments were initially assessed with a Leitz MZ10 (Leitz) stereo microscope to assess their general condition. As sample 15 was of inadequate quantity for histological analysis, it was dehydrated in ethanol, gold coated, and viewed in secondary electron mode with a JCM6000 scanning electron microscope (JEOL). The section of sample 15 that was examined via SEM was taken from the junction of the intra-articular longitudinal fibers and the extra-articular woven fibers. The remnant was scanned, and a cross section through the woven extra-articular fibers was evaluated.
Results
Patient Demographics
The 14 explanted ligaments that were examined histologically with traditional light microscopy were harvested from 11 males and 3 females. The mean ± SD age of these patients at the time of implant removal was 40.5 ± 16.2 years (range, 19-66 years), with the mean time in situ being 26.57 ± 13.4 months (Table 1). The activity level on these patients was recorded as low (n = 2), moderate (n = 4), or high (n = 8), with only 1 patient in the low activity category requiring a mobility aid.
Patient Demographics and General Intraoperative Observations a
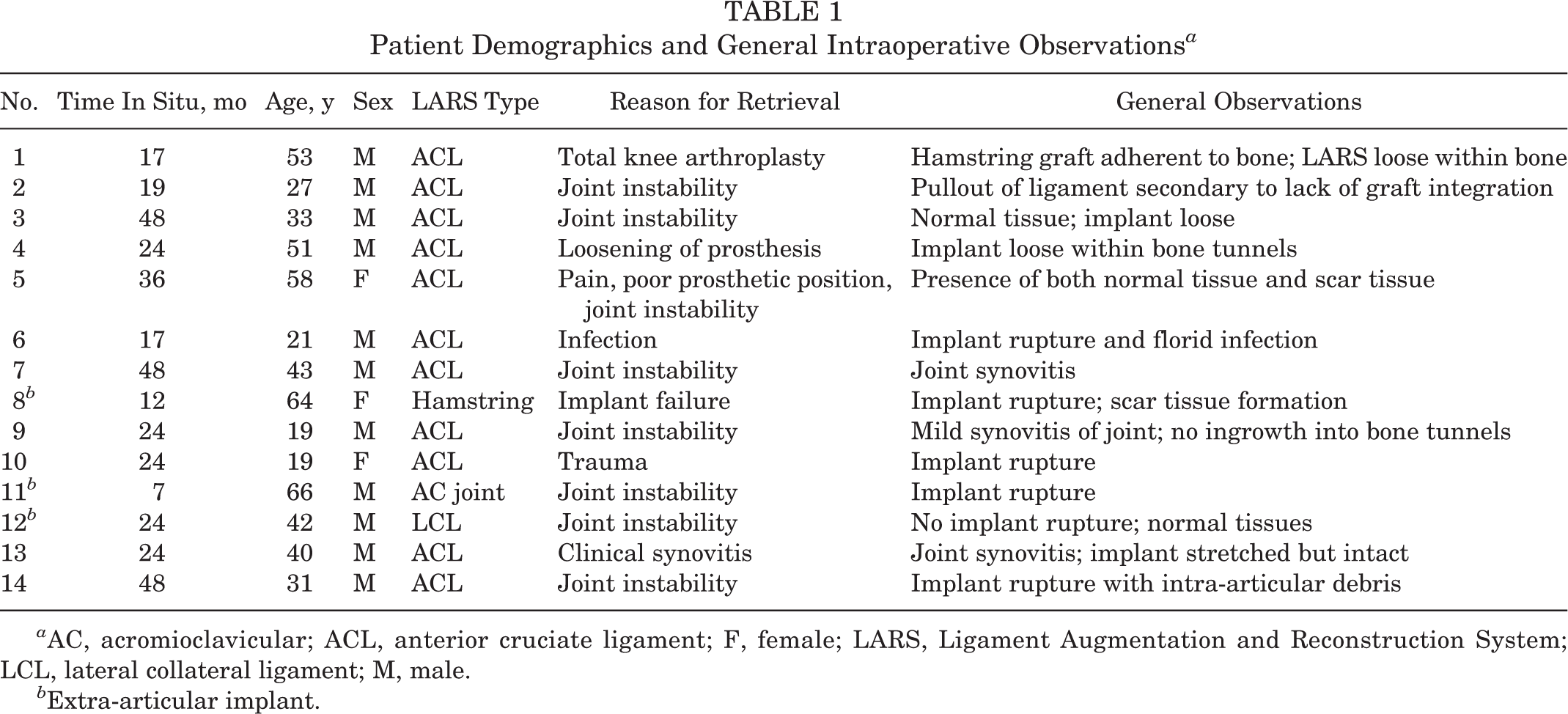
a AC, acromioclavicular; ACL, anterior cruciate ligament; F, female; LARS, Ligament Augmentation and Reconstruction System; LCL, lateral collateral ligament; M, male.
b Extra-articular implant.
Operative Findings
Of the 14 implants examined, 9 ligaments were reported to have failed, with 5 prostheses having ruptured and 4 having been pulled out or loosened away from the bone. Four surgically treated joints revealed macroscopic signs of inflammation, with 3 knees showing generalized synovitis and 1 knee having a florid late-stage infection. Of these 4 cases, only 1 was associated with rupture of the ligament prosthesis (Table 1).
Histological Analysis
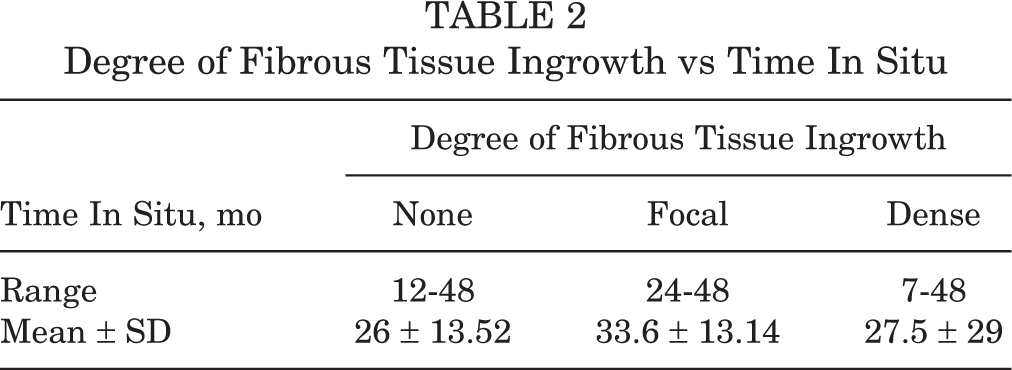
Ingrowth of fibrous tissue was observed in 7 of the 14 samples. Of these, 2 samples were reported to have dense or mature ingrowth, while the remaining 5 exhibited only focal signs of fibrous inset. There was great variation between the time in situ of all samples and the degree of fibrous tissue ingrowth observed, as shown in Table 2. Table 3 demonstrates the relationship between the degree of fibrous tissue ingrowth and the macroscopic outcome of the prosthetic ligament in terms of rupture, loosening, or neither at the time of explantation.
Degree of Fibrous Tissue Ingrowth vs Time In Situ
Associated Degree of Fibrous Tissue Ingrowth vs Operative Observations

A foreign body response, demonstrated by inflammation associated with the presence of giant cells or multinucleated histiocytes on histological analysis, was observed in 10 of the 14 samples (Figures 1 -4). Each sample was reported to have either a moderate or severe reaction, with the time in situ ranging from 17 to 48 months (mean, 31.2 ± 12.6 months). Only 3 samples (samples 8, 11, and 12) did not produce any immunological response and were explanted between 7 and 24 months (mean, 14.33 ± 8.74 months) after the original surgery. All 3 samples were extra-articular implants. Table 4 demonstrates the results of the observed foreign body response as compared with that of ligament rupture or loosening.

Bundles of LARS material showing a marked foreign body inflammatory response, with multinucleated giant cells surrounding individual LARS fibers. There is intervening hyalinized hypocellular fibrous tissue. LARS, Ligament Augmentation and Reconstruction System.

Residual polyethylene-based material can be seen with an associated foreign-body giant cell response.

Disrupted LARS material with a foreign-body giant cell response and intervening markedly hypocellular hyalinized fibrous tissue. LARS, Ligament Augmentation and Reconstruction System.

Marked foreign-body giant cell response to LARS material, with moderately cellular fibrous tissue ingrowth. LARS, Ligament Augmentation and Reconstruction System.
Association of Foreign Body Response vs Operative Observations

Hyalinized necrotic tissue was evident in 3 of the 14 samples, and 3 samples showed signs of an old hemorrhage in the form of hemosiderin-laden histiocytes.
Scanning Electron Microscopy
One sample was collected and examined via SEM after spending approximately 6 years in situ. At the time of explantation, the surrounding tissues appeared normal with no macroscopic signs of an immune reaction. By this stage, the ligament appeared to be fully encapsulated in fibrous tissue (Figure 5, A and B), with such tissue having infiltrated between the woven and individual fibers (Figure 5, D and E). The intra-articular sections examined showed evidence of fracture (Figure 5C), although there were no signs of splitting, shredding, or general degradation that would be expected with long-term wear (Figure 5, C and F).

(A, B) Scanning electron microscope images of explanted LARS ligaments demonstrating fibrous ingrowth, (C) prosthetic fracture, (D, E) fibrous tissue infiltrating woven and individual fibers, and (C, F) long-term wear. LARS, Ligament Augmentation and Reconstruction System.
Discussion
The use of artificial prostheses for the reconstruction of ruptured ligaments has been widely examined since their introduction in the 1970s. They have produced attractive short-term results with great strength and early return to activity, as widely publicized in the media by numerous professional athletes around the globe. A study published in 2002 by Nau et al 8 examined functional differences over a 24-month period following anterior cruciate ligament (ACL) reconstruction with both the LARS ligament and the bone–patellar tendon–bone autograft in 53 cases of chronic symptomatic ACL rupture. Their study demonstrated no differences in International Knee Documentation Committee (IKDC) score and a consistently better Knee injury and Osteoarthritis Outcome Score (KOOS) for the LARS ligament during the first year of follow-up, as well as greater instrument-tested laxity for the LARS ligament at all stages of assessment. These differences, however, were no longer evident at 24 months and revealed no statistical significance by the end of the study.
A study by Iliadis et al 5 comparing artificial ligaments for ACL reconstruction among 72 patients demonstrated high rupture rates for both LARS ligaments (31%) and ABC polyester ligaments (42%) over a follow-up period of 6 to 14 years (mean, 9.5) and 1 to 8 years (mean, 5.1), respectively. The majority of ruptures occurred because of reinjury of the reconstructed knee, usually during sport. Some cases of rupture in the LARS group occurred without knee injury, perhaps signaling graft wear given the longer period of follow-up.
Many review articles, such as those by Legnani et al 7 in 2010 and Chen et al 1 in 2015, have examined the uses and outcomes of synthetic substitutes for ligament reconstructions and have advocated for caution when using such prostheses: although synthetic substitutes have produced promising short-term outcomes, the few long-term data available have revealed inferior results. The reviewers concluded that the ideal characteristics required for an artificial ligament are biocompatibility (chemical stability, degree of polymerization, absence of soluble additives, scarce water absorption, presence of pores for fibroblastic ingrowth) and mechanical properties that mimic the native ligament (traction resistance, stiffness, elongation, torsion, and abrasive resistance). Despite their promising early advantages, artificial ligaments have shown poor long-term outcomes and have been plagued by complications such as joint instability, rupture, high rates of revision, and the development of a foreign body reaction and resultant chronic synovitis. 1 –5,7,8,11,12
All types of artificial ligaments developed so far have been associated with at least some degree of foreign body reaction. 1 –5,7,9,11,12 The LARS Company has worked to refine its prosthesis to produce a strong reconstruction, minimize complications, and optimize biocompatibility. Minerals and natural oils, such as isopalmytate and butyl isostearate, were previously used in the “sizing” process—a technique in which oils are introduced into the ligament fibers so that the carding and spinning of the fibers are made much easier. The LARS Company has now refined its “de-sizing” procedure—the procedure through which the oils used in the sizing process are removed—which has significantly improved since the 1980s to the extent that all cytotoxic substances that could potentially trigger a foreign body reaction have been eliminated. 10 Despite these improvements, there are still reports of foreign body reactions and chronic synovitis in the literature associated with the use of LARS ligaments. 1 –5,7,11,12
Other artificial ligaments made of polyethylene terephthalate, such as the Leeds-Keio ligament, have been shown in previous studies to produce a foreign body reaction of varying degrees between 24 and 48 months following implantation. 1 Glezos et al 3 published a case report in 2012 describing 1 case of ACL reconstruction using the LARS ligament, which produced disabling chronic synovitis, presenting first as pain and effusion of the joint 6 months after initial implantation of the device and ultimately resulting in removal of the prosthesis and complete synovectomy after only 12 months in situ.
In our study, we observed a foreign body reaction in 10 of the 14 explanted LARS ligaments (71.4%), with variation in the severity of the immunological response seemingly unrelated to the time in situ. Interestingly, implant failure occurred in only 5 of the 10 explanted samples that exhibited foreign body reaction (2 ruptured and 3 loosened ligaments), with the remaining 5 prostheses appearing intact at the time of removal (Table 4). Note that all 3 samples that did not produce a foreign body reaction (samples 8, 11, and 12) were extra-articular implants and were not exposed to the intra-articular environment. The 4 samples that exhibited macroscopic signs of inflammation were implanted for 17 to 48 months (mean, 28.25 ± 13.57 months); however, it is uncertain for how long these reactions had persisted. Of the 10 positive samples, 7 were revised for joint instability, 1 for pain (synovitis), 1 for reinjury of the reconstructed knee, and 1 for a late-stage infection.
Despite the manufacturer’s efforts to improve the biocompatibility of its prostheses, it is evident from our investigation that the LARS ligament still produces a foreign body reaction within the reconstructed joint. The degree and timing of such a reaction, however, are unclear and may be a function of surgical technique, host immune response or sensitivity, or other patient factors. Dedicated tissue biopsies of specific regions, such as areas of synovium, tunnel, or intra-articular portions of the joint, could have been taken to correlate with ligament samples to strengthen our results, although this, unfortunately, was not considered prior to removal of the implant samples. The reliability of our results may have been further improved by better documentation of patient symptoms, physical examination, imaging, and preoperative blood tests, for us to truly correlate the clinical preoperative picture with our operative and histological findings.
The extent of the foreign body reaction generated with the use of LARS ligaments may be affected by the development of fibroblastic ingrowth. It is thought that by promoting fibrous ingrowth into the artificial prosthesis, it is possible to improve the strength and longevity of the graft while limiting the production of an immune response. Of the 7 samples that demonstrated fibrous tissue ingrowth into the LARS ligament, 5 produced only focal or incomplete ingrowth, while 2 showed dense or complete fibrous coverage. Interestingly, the 2 samples with extensive fibrous coverage were completely free of any foreign body reaction, while all 5 of the remaining samples with only focal or partial fibrous ingrowth were associated with at least some degree of immune response (Figures 1 and 4).
From this, we cannot draw any firm conclusion about the incidence of the observed immune response to failure of the graft; however, we hypothesize that the complete coverage of the prosthesis with dense fibrous tissue may act to reduce abrasion and wear of the graft fibers against the bone or may even prevent the release and deposition of wear particle into the joint. It is important to note, however, that both samples that exhibited dense fibrous ingrowth (samples 11 and 12) were extra-articular implants and therefore not exposed to the intra-articular environment. It can therefore be thought that the immune response to the graft may have a detrimental effect on the development of fibrous tissue ingrowth. The LARS ligament is designed to facilitate and accelerate fibrous ingrowth into the prosthesis via improved microporosity, although the results produced by the ligament are still rather poor. 1 –5,7,11,12 Furthermore, the LARS Company claims that its ligaments produce complete fibrous coverage by the sixth week following implantation; however, these claims were not supported by our results, as indicated by the inconsistencies seen in the degree of fibrous ingrowth and the variation in time in situ of the examined samples.
Evaluation of the LARS ligament via SEM demonstrated extensive fibrous tissue ingrowth with only minor evidence of wear or degradation of the ligament itself, despite having remained in situ for 6 years. There were no macroscopic signs of an immune reaction when the sample was removed, and unfortunately, given the small quantity of retrieved ligament that we received, we were unable to evaluate the same sample histologically. As we had only 1 sample evaluated via SEM and no histological data with which to compare our results, we were unable to draw any conclusions between the SEM findings and the potential development of a foreign body reaction. We did, however, see the potential for deep fibroblastic ingrowth into the intra- and extra-articular sections of the LARS ligament, and we also observed the effects of this ingrowth on fracture and mechanical wear of the prosthesis. In future studies, SEM may be employed to further evaluate these effects and potentially correlate patient symptoms and examination findings with the degree of mechanical wear and likelihood of implant failure.
With this study, we demonstrated that the LARS ligament, despite efforts to reduce complications through improved design, is still associated with the development of a foreign body reaction. We can draw these conclusions from the data that we collected, but there is still an absence of medium- to long-term outcome studies in the literature to support our results. Synovial biopsies taken at the time of implant removal may have helped strengthen our results by confirming the presence of wear debris; however, these were not taken, and we are unable to confirm that the immune reaction was indeed a response to the presence of the artificial graft. We cannot definitively report the rate of foreign body reaction, as this retrieval study examined only failed explanted ligaments, while many cases of subclinical foreign body reaction may avoid detection.
Furthermore, with our minimal mechanical and SEM data, we were unable to completely ascertain the effects of an immune response on the mechanical properties of these ligaments or to say with certainty how the development of fibroblastic ingrowth may act to augment the immune response. A study aimed at correlating a patient’s preoperative state with the degree of implant wear and mechanical failure is the next step in predicting patient outcomes and preventing aseptic synovitis with the use of artificial ligaments. Such a study would require (1) collecting detailed documentation of each patient’s preoperative symptoms, examination findings, imaging, and blood test results and (2) cross-referencing them with detailed operative findings and systematically collected samples from various set regions of the joint and excised implant, as well as (3) comparing histological and SEM findings for each sample. It has also been suggested that there is the potential for the LARS ligament to be applied as a short- to medium-term adjunct to definitive autologous or allograft reconstructions, although there are no clinical data in this regard. Nonetheless, there is the potential to achieve the long-term stability of natural ligament reconstruction while avoiding the medium- to long-term complications associated with the use of artificial LARS ligaments. In any case, foreign body reaction may still be an issue.
Conclusion
As with the authors of many previous studies, we have concluded that the LARS ligament should be used with caution and that all patients should be closely followed up, monitored, and investigated for potential adverse effects, particularly in relation to the development of a foreign body reaction. More medium- and long-term studies are required, and an understanding of the natural history of LARS-related foreign body reactions is needed to establish safe clinical guidelines for its use. A different approach, such as the use of the LARS ligament as an adjunct to definitive natural ligament reconstruction, may represent a new direction that can be taken for the use of artificial ligaments to produce the best overall outcomes for our patients while avoiding potentially devastating long-term complications. With improving design of artificial ligaments, we may also need to consider new modes of use in an attempt to optimize the results of ligament reconstruction surgery and produce better overall patient outcomes.
Footnotes
The authors declared that they have no conflict of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.