
Abstract
Background:
Risk factors for concomitant ligament injuries (CLIs) of the lateral collateral ligament (LCL) and medial collateral ligament (MCL) in children and adolescents with anterior cruciate ligament (ACL) tears are unknown.
Purpose:
To determine whether body mass index (BMI), sex, age, and injury mechanism are associated with CLIs in children and adolescents with ACL tears and whether CLIs are associated with meniscal and chondral injuries and a delay to surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We reviewed the records of patients aged ≤18 years with ACL tears from 2009 through 2013 for sex, age, height, weight, CLI, injury mechanism, intra-articular injury, and time to surgery. Patients were assigned to groups according to the presence of a CLI (CLI group) compared with the presence of an isolated ACL tear (ACL group). BMI was categorized as underweight, normal weight, or overweight/obese. The older group was defined as age ≥14 years for girls and ≥16 years for boys. Logistic regression, Mann-Whitney U tests, and chi-square tests were performed (alpha = 0.05).
Results:
We included 509 patients (267 girls) with a mean age of 15 years (range, 6-18 years) at the time of injury. There were 396 patients (78%) in the ACL group and 113 patients (22%) in the CLI group (90 with MCL, 11 with LCL, and 12 with both MCL and LCL injuries). Groups had similar proportions of overweight/obese patients (P = .619) and girls (P = .104). Older age (odds ratio [OR], 2.0 [95% CI, 1.3-3.3]) and contact injuries (OR, 2.2 [95% CI, 1.4-3.4]) were associated with CLIs. The CLI group had a higher proportion of chondral injuries (P = .001) but not meniscal injuries (P = .295) and presented to surgery earlier than the ACL group (P = .002).
Conclusion:
Older age and contact injuries were associated with CLIs in children and adolescents with ACL tears, whereas BMI category and sex were not. CLIs were associated with a higher proportion of chondral injuries but not meniscal injuries and were not associated with a delay to surgery.
Keywords
The anterior cruciate ligament (ACL) is the most commonly injured ligament of the knee for which reconstructive surgery is performed. 30 However, ACL injuries rarely occur as an isolated event and typically include associated meniscal, articular cartilage, subchondral bone, and collateral ligament injuries. 30 It is critical to identify all injured structures and to determine injury severity to formulate an optimal treatment plan.
The medial collateral ligament (MCL) is commonly injured during an ACL rupture. Approximately 78% of grade III MCL injuries consist of mixed ligamentous lesions, with an injury to the ACL occurring more than 95% of the time. 13 Likewise, the posterolateral corner and the lateral collateral ligament (LCL) are commonly associated with ACL tears, with only 27% of these injuries occurring in isolation. 15 Approximately 57% of grade III LCL injuries occur with a concomitant ACL tear. 15
Although studies have examined the outcomes of collateral ligament injuries in the presence of ACL reconstruction, 8,16,19,26 there are scant data concerning risk factors for these associated injuries in children and adolescents. The purpose of this study was to determine whether body mass index (BMI) category, mechanism of injury, sex, and age group are associated with the rate of concomitant ligament injuries (CLIs) in children and adolescents with ACL tears and whether these CLIs are associated with meniscal and chondral injuries and a delay to surgery. We hypothesized that the CLI group would present to surgery later; have a higher proportion of associated chondral and meniscal injuries; and include more patients who sustained contact injuries and who were older, female, and overweight/obese compared with the ACL group.
Methods
We retrospectively reviewed the medical records of patients who presented to our institution with ACL tears from January 2009 through October 2013. After receiving institutional review board approval, we identified records with ICD-9-CM (International Classification of Diseases, Ninth Revision, Clinical Modification 9 ) diagnostic code 844.2 and CPT (Current Procedural Terminology 1 ) code 29888 for primary ACL reconstruction. We excluded patients with incomplete clinical records, posterior cruciate ligament (PCL) tears without a collateral ligament injury, or ACL graft tears in the setting of previous ACL reconstruction.
The records of all patients aged ≤18 years at the time of injury were reviewed. Variables analyzed were sex, BMI category, mechanism of injury, and age group (older group was defined as age ≥14 years for girls and ≥16 years for boys). Clinical documents and operative reports detailing examination findings as well as magnetic resonance imaging were used to identify CLIs of the knee. We combined grade I and grade II CLIs, and we treated grade III CLIs separately because grade III injuries are commonly reconstructed. We calculated BMI using patient data collected within 30 days of surgery. Using a publicly available calculator from the Centers for Disease Control and Prevention, 8 we assigned patients to the following categories: underweight (≤4th percentile), normal weight (5th-84th percentile), or overweight/obese (≥85th percentile).
Statistical Analysis
Logistic regression, chi-square tests, Mann-Whitney U tests, and independent t tests were performed using SPSS version 22.0 software (IBM). Alpha level was set at 0.05.
Results
Patient Characteristics
We identified 509 patients (267 girls) who underwent primary ACL reconstruction and met the study criteria. There were 396 patients with an isolated ACL injury (ACL group) and 113 patients with CLIs (CLI group). Regarding BMI, 333 (65%) patients were categorized as normal weight and 176 (35%) patients were categorized as overweight/obese. Two patients were categorized as underweight and were excluded. The mean age at the time of injury was 15 years (range, 6-18 years), with 253 patients (73 boys [29%] and 180 girls [71%]) categorized in the older group. Most injuries occurred during sports (91%, n = 463), ranging from the recreational to the professional level. The remaining 46 patients (9%) sustained an injury from other causes such as falling down stairs or motor vehicle or pedestrian accidents. Overall, 167 patients (33%) had contact injuries and 342 patients (67%) had noncontact injuries.
Types of CLIs
The frequency of injuries by ligament type is shown in Table 1. For simplicity, 1 patient with a PCL injury in the absence of an LCL or MCL injury was excluded from the study because our main objective was to assess collateral ligament injuries. Patients were categorized into 4 groups: (1) isolated ACL injury; (2) combined ACL and MCL injuries; (3) combined ACL and LCL injuries; and (4) combined ACL, LCL, and MCL injuries. The presence of a PCL injury did not affect categorization. There were 113 (22%) patients with CLIs (90 with MCL injuries, 11 with LCL injuries, and 12 with both MCL and LCL injuries). Of the 11 LCL injuries, 10 patients had grade I or grade II injuries, and 1 patient had a grade III injury. Of the 90 MCL injuries, 76 patients had grade I or grade II injuries, and 14 patients had grade III injuries. All 12 patients with both MCL and LCL injuries had grade I or grade II injuries.
Concomitant Ligament Injuries in 509 Children and Adolescents With ACL Tears a

a ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Risk Factors for CLIs
The mean (±SD) age at the time of injury was 15 ± 1.7 years for the CLI group and 14 ± 2.2 years for the ACL group (P = .005). In terms of sex, there was no significant difference between the CLI and ACL groups (59% girls vs 51% girls, respectively; P = .104). There were more patients in the older group for boys and girls in the CLI group (63%) compared with the ACL group (46%) (P = .002). The CLI group had a higher proportion of contact injuries (44%) compared with the ACL group (30%) (P = .003). There was no significant difference in the mean BMI percentile between the CLI group (74th percentile) and the ACL group (71st percentile) (P = .343) or in the percentage of overweight/obese patients between the CLI group (33%) and the ACL group (35%) (P = .619). Univariate and multivariate logistic regression were performed to assess BMI category (normal weight vs overweight/obese), sex, age group, and mechanism of injury (noncontact vs contact) (Table 2). Only older age (odds ratio [OR], 2.0 [95% CI, 1.3-3.3]) and contact injuries (OR, 2.2 [95% CI, 1.4-3.4]) were significantly associated with CLIs.
Odds of Experiencing a Concomitant Ligament Injury in 509 Children and Adolescents With ACL Tears a
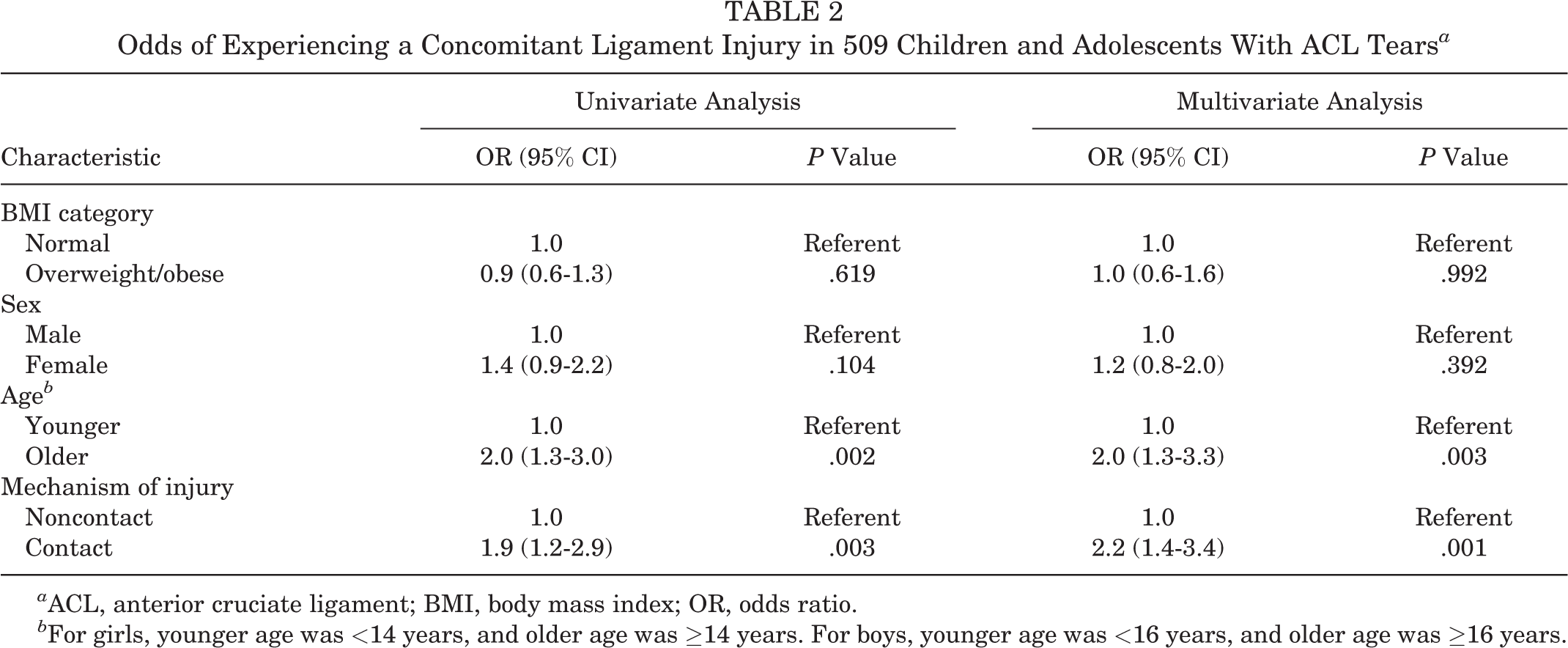
a ACL, anterior cruciate ligament; BMI, body mass index; OR, odds ratio.
b For girls, younger age was <14 years, and older age was ≥14 years. For boys, younger age was <16 years, and older age was ≥16 years.
The CLI group had a higher proportion of associated chondral injuries (71%, n = 80) compared with the ACL group (53%, n = 209) (P = .001). There was no difference between the CLI group (77%, n = 87) and the ACL group (72%, n = 286) in terms of associated meniscal injuries (P = .295). Of the 90 patients with MCL tears, 66 had a meniscal injury (5 medial, 49 lateral, and 12 medial and lateral), and of the 11 patients with LCL injuries, 10 had a meniscal injury (7 lateral and 3 medial and lateral). Of the 12 patients with MCL and LCL injuries, 11 had a meniscal injury (2 medial, 6 lateral, and 3 medial and lateral). The median time to surgery was 6.7 weeks (range, 0.86-33 weeks) for the CLI group and 7.7 weeks (range, 1-141 weeks) for the ACL group (P = .002).
Discussion
We found that older age and contact injuries were risk factors for CLIs in children and adolescents with ACL tears. Contrary to our hypothesis, higher BMI and female sex were not associated with a higher rate of CLIs. There was a higher prevalence of chondral injuries but not meniscal injuries, without an associated delay to surgery, for patients with CLIs.
Risk factors for ACL tears have been studied extensively and include female sex, type of sport, hamstring weakness, increased knee joint laxity, increased BMI, improper biomechanics (eg, valgus knee motion during landing), small ACLs, decreased width of the intercondylar notch, genetic factors, and shoe-surface interface. 3,6,10,14,18,26,31 Addressing these risk factors with interventions such as neuromuscular training can prevent and reduce the incidence of ACL tears. 17 Often, however, ACL tears are accompanied by other ligamentous injuries, specifically MCL injuries. To our knowledge, no studies have examined risk factors for these associated ligament injuries in children and adolescents.
Prior studies have examined CLIs in relation to sex and BMI. Roach et al 27 reported on the incidence of isolated MCL injuries in cadets at the US Military Academy and found no significant difference between men (7.6%) and women (5.4%) (P = .212). Uhorchak et al 31 analyzed the BMIs of 895 cadets at the US Military Academy and found that those who sustained noncontact ACL injuries had a higher mean BMI (25 kg/m2) than those who did not (23 kg/m2) (P = .002). Gomez et al 16 found that 215 high school football players with BMIs >32 kg/m2 had 1.86 times higher odds of sustaining lower extremity injuries (including foot, ankle, hamstring, MCL, and ACL sprains and knee and shin contusions) compared with athletes with BMIs ≤32 kg/m2. In our study, we found no significant differences in the rates of CLIs by sex or BMI.
Newman et al 25 reported the rates of concomitant ACL and MCL injuries of 1.5% (1/66) in patients aged ≤14 years and 2.4% (4/165) in patients aged 14 to 19 years. Of note, they reported no LCL or PCL injuries. These lower rates of CLIs in skeletally immature patients may be attributable to increased ligamentous strength relative to bone compared with that of mature patients. 28 Kluczynski et al, 20 using data from a prospective registry of children and adults undergoing ACL reconstruction, reported a higher rate of contact injuries in patients with combined ACL and MCL tears (58%) compared with patients with isolated ACL tears (21%) (P < .0001). This difference may be because contact injuries more often deliver a varus or valgus load than noncontact injuries. Similarly, in our study, we found an association of higher CLI rates in older children and adolescents and in those with contact injuries.
In our study, an isolated ACL injury occurred at a rate of 78%, whereas 2-ligament injuries (ie, ACL and LCL or MCL) occurred at a rate of 17%. Three-ligament (4%) and 4-ligament (<1%) injuries were rare. The most common CLI was an MCL injury, occurring in 16% of patients. Similarly, LaPrade et al 21 reported on the rates of associated ligamentous injuries in the setting of an ACL tear in adults, using magnetic resonance imaging for acute knee injuries. Isolated ACL injuries occurred at a rate of 61% (83/136), with the second highest rate being ACL and MCL injuries at 21% (29/136).
In our study, we found no difference in meniscal injuries between groups; however, chondral injuries were more prevalent in the CLI group compared with the ACL group. Kluczynski et al 20 reported that there was no statistically significant difference between patients with ACL and MCL injuries compared with patients with isolated ACL injuries in the prevalence of lateral meniscus tears (53% vs 43%, respectively; P = .34), medial meniscus tears (31% vs 34%, respectively; P = .85), and chondral lesions (16% vs 11%, respectively; P = .50). Other studies have shown that lateral meniscus tears (18%-80%) are more prevalent than medial meniscus tears (0%-28%) in the presence of ACL and MCL tears. 4,5,12,23,24,29 In the current study, we have verified this with rates of 74% and 5%, respectively. Studies have consistently found that a delay to surgery is a risk factor for more meniscal and chondral injuries. 2,7,11,22,25 However, a delay would not explain the increased prevalence of chondral injuries in the current study because we found that, on average, the CLI group underwent surgery earlier than the ACL group.
Our study is limited by several factors inherent to a retrospective analysis. The diagnoses of ligamentous, meniscal, and chondral injuries were identified and classified by the treating surgeon only. Although we reported the prevalence of chondral injuries, we did not localize or grade the severity of these injuries. Additionally, grade I and grade II ligament injuries were grouped together. We did not analyze long-term outcome data because our study focused on identifying risk factors for CLIs and not the treatment or long-term outcomes of surgical correction. Our study used chronological age to define younger and older patients; skeletal age will be a better reference for future studies. The major strengths of the study are the large sample size, having accounted for the different rates of maturation for boys and girls by using age groups, and the use of BMI percentiles specific to the pediatric population.
We believe that this study provides valuable information about risk factors for CLIs in the setting of ACL tears in children and adolescents. Consistent with previous studies, MCL tears were the most common CLI, whereas LCL tears and combined MCL and LCL tears were much less prevalent. BMI category and sex were not associated with CLIs. Patients with contact injuries and older patients had a higher prevalence of CLIs than those with noncontact injuries and younger patients. CLIs were associated with a higher proportion of chondral injuries but not meniscal injuries.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.L. has received educational support from Medtronic and research support from Arthrex. T.J.G. has received educational support from Arthrex and Liberty Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children’s Hospital of Philadelphia Institutional Review Board.