
Abstract
Background:
Various grafts and ligament augmentation devices (LADs) have been used in the search for optimal reconstruction of the anterior cruciate ligament (ACL).
Purpose:
To compare 25-year follow-up results after ACL reconstruction using a bone–patellar tendon–bone (BPTB) graft with or without the Kennedy LAD.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
One hundred patients undergoing ACL reconstruction between 1991 and 1993 were randomized into 2 groups: reconstruction using a BPTB graft alone (BPTB group, 51 patients) or a BPTB graft with the Kennedy LAD (LAD group, 49 patients). The 25-year follow-up evaluation included a clinical knee examination, patient-reported outcome measures, and an assessment of radiological osteoarthritis (OA) according to the Ahlbäck classification. Additional outcomes were reruptures and knee arthroplasty.
Results:
Ninety-three patients (93%) were available for the follow-up evaluation: 48 patients in the BPTB group and 45 in the LAD group. Through telephone calls, 26 patients were excluded from further investigation because of reruptures and arthroplasty in the knee of interest; 67 patients were further investigated. A total of 43 of 44 (98%) and 42 of 44 (95%) patients had negative or 1+ Lachman and pivot-shift test results, respectively. The mean Lysholm score was 85 for the BPTB group and 83 for the LAD group. All mean Knee injury and Osteoarthritis Outcome Score (KOOS) subscale values were ≥73. There were no statistically significant differences between groups in any of these outcomes or regarding the Tegner score, radiological classification of OA, or number of ACL reruptures. Signs of radiological OA were detected in all patients, and severe radiological OA (Ahlbäck grade III, IV, or V) was detected in 32% of patients in the BPTB group and 21% of patients in the LAD group (P = .37). There were 12 patients in the BPTB group and 7 in the LAD group who had documented reruptures (P = .40). One patient in the BPTB group and 6 in the LAD group underwent knee arthroplasty (P = .054).
Conclusion:
In the present study, there were no statistically significant differences between groups in any of the outcomes. After 25 years, 19% of patients had reruptures, 27% had severe radiological OA, and 7% underwent knee arthroplasty.
Keywords
The bone–patellar tendon–bone (BPTB) autograft is one of the most common grafts used in anterior cruciate ligament (ACL) reconstruction. Overall, 85% to 90% of patients receiving this graft report good to excellent outcomes. 25 However, there are some limitations with the use of autografts, such as complications at the donor site, insufficient strength of the autograft compared with the original ACL, and the need of immobilization and protection for optimal graft fixation and revascularization. 21 In a review article, Kartus et al 16 stated that 40% to 60% of patients who underwent reconstruction with BPTB grafts reported various donor site problems. These included anterior knee pain, decreased sensitivity of the knee, and kneeling pain. Because of these weaknesses of autografts generally, and BPTB grafts specifically, synthetic grafts were popular in the 1980s. However, synthetics were later abandoned because of poor results and complications. 15,25,49 Augmentation first became popular during the 1980s after Kennedy et al 19 suggested that it would offer safer and faster healing of the graft, especially during the early postoperative phase. The Kennedy ligament augmentation device (LAD) consists of a bandlike braid of polypropylene, and Kennedy and colleagues 19 suggested that the device would take most of the load in the first phase of the healing process before it gradually transferred the load to an autograft or primary repair site. Their hypothesis was that this would enable earlier functional recovery. 19
The aim of the present study was to detect any differences between 2 groups at 25-year follow-up of a randomized controlled trial, in which results have previously been reported at 2- and 8-year follow-ups. Specifically, patients who had undergone ACL reconstruction using a BPTB graft alone (BPTB group) were compared with those who had undergone ACL reconstruction using a BPTB graft with a LAD (LAD group). Our hypothesis was that patients reconstructed using a BPTB graft without the LAD had the same outcomes 25 years after surgery as patients reconstructed using a BPTB graft with the LAD.
Methods
One hundred patients with ruptured ACLs, who had undergone ACL reconstruction in the period from 1991 to 1993, participated in the study. Randomization was performed with the sealed-envelope method. A national ethics committee approved the study, and written consent was provided by all the examined participants. As previously reported, 13 there were 55 women and 45 men. The mean age at surgery was 25 years (range, 16-42 years) for the BPTB group and 27 years (range, 17-48 years) for the LAD group. The mean time from injury to surgery was 40 months (range, 1-180 months) for the BPTB group and 46 months (range, 3-168 months) for the LAD group, and the ACL rupture was detected both clinically and arthroscopically. The indications for surgery were functional instability with pain and/or swelling during sports or other physical activities. 13 Ninety-five percent of the injuries were caused by sports participation, with team handball and soccer as the favorite activities. There were 51 patients in the BPTB group and 49 in the LAD group, and there were no statistically significant differences between the 2 groups in the level of preinjury activity, age, sex, or previous surgery. 13 Patients with signs of knee injuries other than to the ACL, meniscus, or cartilage were excluded from the study.
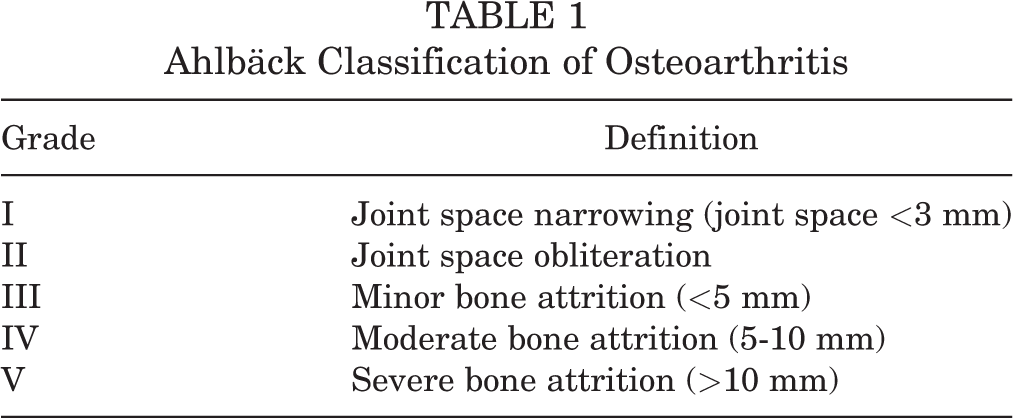
The patients in the current study were first approached by telephone calls to screen whether they had sustained a rerupture of the ACL or underwent arthroplasty. Those who had not were invited to participate for further examinations. The clinical knee examinations were performed by 2 independent observers, M.M.E., and either J.O.D., L.E., T.O.L., or T.G., who were experienced orthopaedic surgeons. Range of motion (ROM), the Lachman test, the pivot-shift test, and KT-1000 arthrometer measurements (MEDmetric) were examined. The Tegner activity scale, 45 the Lysholm functional score, 24 and the Knee injury and Osteoarthritis Outcome Score (KOOS) 39 were completed by either the patient or by the examiner through a telephone interview. Radiographs of the knees were obtained by anteroposterior imaging in the Rosenberg view. The radiographs were then evaluated and graded according to the Ahlbäck 1 classification of osteoarthritis (OA) (Table 1) by an experienced radiologist (R.B.) who did not have any clinical knowledge of the patients.
Ahlbäck Classification of Osteoarthritis
Operative Technique and Rehabilitation
The operative techniques and rehabilitation protocol for both groups have been described in detail in a previous study. 13 The procedures were carried out under epidural anesthesia with the use of a tourniquet. Notchplasty was performed and, if necessary, treatment of the menisci. The menisci were treated with either partial resection, bucket-handle resection, or suturing. The grafts were harvested from the middle third of the ligamentum patellae through 2 short transverse incisions over the patella and the tibial tubercle. In the LAD group, a Kennedy LAD, 8 mm wide and 18 cm long, was sutured to the graft. The femoral tunnel was made by using an outside-in drill guide and a K-wire through the lateral femoral condyle to an exit at the posterior part of the anatomic origin of the ACL on the femoral condyle. When used, the LAD was fixed to the lateral femoral condyle with 2 staples in a belt-buckle fashion, and the tibial end was fixed to the tibia with staples, resulting in double-end fixation.
Postoperatively, the patients underwent an identical rehabilitation program under supervision by the same 2 physical therapists. This included knee motion immediately after surgery, full passive extension of the knee several times a day, and full weightbearing as soon as this could be tolerated. No brace was used. The patients were allowed to return to full sporting activities after 6 months, provided that the strength of the thigh muscle on the operated side was at least 85% of that on the contralateral side and that controlled functional training had been performed without difficulty.
Statistical Analysis
SPSS Statistics version 24.0 (IBM) was used to conduct the statistical analysis. The Mann-Whitney U test was used to examine differences between the groups, and the Pearson chi-square test and Fisher exact test were used for categorical variables. Differences were considered statistically significant when P < .05.
Results
Of the original 100 study patients, 93 were available for the 25-year follow-up evaluation: 48 patients in the BPTB group and 45 in the LAD group. Of the remaining 7 patients who did not participate in our follow-up, 2 patients were dead, 4 patients were unreachable, and 1 patient did not give consent to participate (Figure 1).
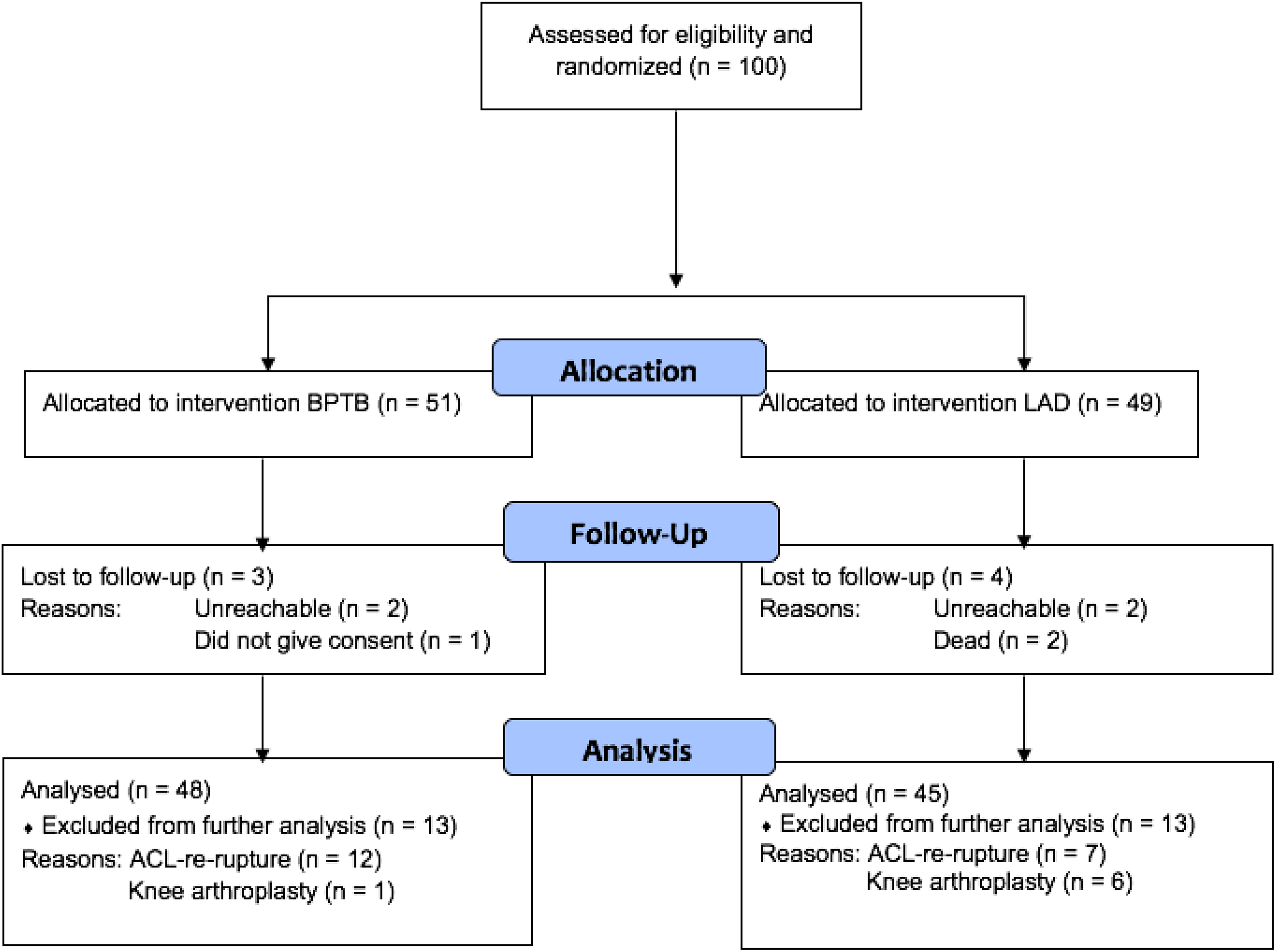
Study flowchart.
There were 19 patients with a documented rerupture of the ACL and 7 who underwent arthroplasty in the knee of interest. Of the 19 patients with documented reruptures, there were 12 in the BPTB group and 7 in the LAD group (P = .40). Seventeen of these patients had undergone revision ACL reconstruction, and 2 had their rerupture detected by arthroscopic surgery. At the 8-year follow-up, there were 5 patients with a rerupture in the BPTB group and 6 patients with a rerupture in the LAD group. One patient in the BPTB group underwent knee arthroplasty compared with 6 patients in the LAD group (P = .054). One of these patients underwent unicondylar knee arthroplasty (LAD group). Two patients who underwent knee arthroplasty (both in the LAD group) also underwent revision ACL reconstruction before their joint replacement. The patients with reruptures and those who underwent arthroplasty in the investigated knee were excluded from further analyses. No patients underwent knee arthroplasty at the 8-year follow-up. An unknown proportion of the patients underwent meniscal treatment during the 25 years after ACL reconstruction. Unfortunately, it was not possible to extract exact information on meniscal injuries and surgery. Therefore, this information is not included in the study.
Ultimately, 67 patients (35 in the BPTB group and 32 in the LAD group) were available for investigation at a mean of 25 years (range, 24-26 years). Eleven of these patients were interviewed by telephone only. This interview consisted of questions about additional surgery and injuries, the Tegner activity scale, the Lysholm functional score, and the KOOS.
Fifty-six patients underwent a clinical examination: 28 patients in each treatment group. The results from the ROM analysis are shown in Table 2. No statistically significant differences were found between the treatment groups.
Results of Range of Motion Analysis a
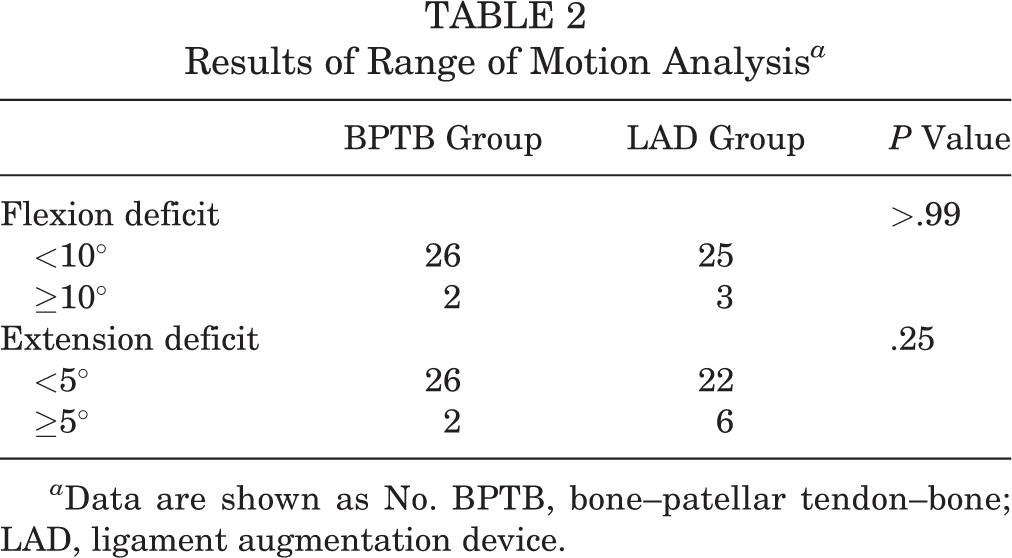
a Data are shown as No. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.
There were 7 of 48 patients in the BPTB group and 6 of 45 patients in the LAD group who had a rupture of the ACL in the opposite knee (P = .90). Two of these patients also had a rerupture in the knee of interest. Additionally, there was 1 patient in the BPTB group who underwent knee arthroplasty on the opposite side. Laxity test results for these patients were excluded from the analyses.
The results from the Lachman and pivot-shift tests are shown in Table 3. No significant differences were found between the groups. Regarding the KT-1000 arthrometer results, we considered the injured-uninjured difference on the maximum manual force displacement test as the principal measurement value. A side-to-side difference >3 mm was considered clinically significant. The results are reported in Table 4. The difference between the mean side-to-side differences in the 2 groups was statistically significant in favor of the LAD group (P = .021).
Results of Lachman and Pivot-Shift Tests a

a Data are shown as No. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.
Results of KT-1000 Arthrometer a

a Data are shown as No. unless otherwise indicated. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.
The median Tegner score was 3 for both the BPTB group (range, 1-9) and the LAD group (range, 0-7) (P = .82) (Figure 2). The mean Lysholm score was 85 (95% CI, 80-90; range, 33-100) for the BPTB group and 83 (95% CI, 79-87; range, 62-100) for the LAD group (P = .395) (Figure 3).

Median Tegner score before injury and at the 2-, 8-, and 25-year follow-ups. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.

Mean Lysholm score preoperatively and at the 2-, 8-, and 25-year follow-ups. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.
The mean values for the 5 subscales of the KOOS are reported in Table 5. There were no statistically significant differences between the groups on any of the 5 subscales (Figure 4).
KOOS Values a

a Data are shown as mean (range). ADL, Activities of Daily Living; BPTB, bone–patellar tendon–bone; KOOS, Knee injury and Osteoarthritis Outcome Score; LAD, ligament augmentation device; QoL, Knee-Related Quality of Life; Sports, Sports and Recreation.

Mean Knee injury and Osteoarthritis Outcome Score (KOOS) value at 25-year follow-up. ADL, Activities of Daily Living; BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device; QoL, Knee-Related Quality of Life; Sports, Sports and Recreation.
Fifty-six patients had radiographs evaluated for OA. The distribution of the different Ahlbäck grades is shown in Table 6. There were no patients without radiological OA in this study. However, Ahlbäck grade I was the most common among our patients. No patients had Ahlbäck grade V. We considered Ahlbäck grade III, IV, and V as severe OA. Altogether, 15 patients (27%) had severe OA: 9 of 28 (32%) in the BPTB group and 6 of 28 (21%) in the LAD group. There were no statistically significant differences between the groups in severe OA (P = .37).
Distribution of Ahlbäck Grades a

a Data are shown as No. BPTB, bone–patellar tendon–bone; LAD, ligament augmentation device.
Discussion
The current 25-year follow-up study found no large differences in the results between the BPTB group and LAD group. As reported in the previous studies on these patient groups, 8,13 we were not able to find any statistically significant differences between the groups in ROM, Lachman test result, pivot-shift test result, patient-reported outcome scores, radiological OA, or rerupture rate 25 years after surgery. This is supported by the results of several other studies. 4,28 –30,33,42,43 There was a statistically significant difference in the mean side-to-side difference in the KT-1000 arthrometer measurements (P = .021). The mean side-to-side differences were 2 mm and 0 mm for the BPTB group and LAD group, respectively. However, the clinical significance of this finding is uncertain, as differences ≤3 mm usually have been classified as normal. 38 There was no advantage with the use of the LAD in the present study. Based on this, we find it reasonable to be skeptical of the increasing use of artificial ligaments and devices in ACL surgery.
Reruptures tended to occur early after reconstruction, as there were already 11 reruptures at the 8-year follow-up. The reason for this could be poor graft positioning, too early return to sports, inadequate tunnel positioning, or failure of graft fixation, among others. 41 After 25 years, there were 8 additional reruptures. If a rerupture is avoided, the BPTB graft seems to be a sustainable graft in the long term, considering the good results from laxity testing. Additionally, subjective assessments of the patients, in terms of both the Lysholm and the KOOS values, showed good knee function and outcomes 25 years after surgery. The mean Lysholm score has been stable since the 8-year follow-up. Unfortunately, 11 of the patients who were included in the analysis of patient-reported outcomes were only interviewed by telephone. The good results from the subjective assessments must be seen in the context of the low Tegner scores, which implies that several patients had low demands on their knee function. The median Tegner score was reduced from 5 (range, 1-9) at the 8-year follow-up to 3 (range, 0-9) at the 25-year follow-up. We consider age as a probable cause for this reduction in the activity level. In addition, signs of radiological OA in all patients may also have contributed to a decrease in the activity level. Nevertheless, most patients seemed satisfied with their knees, and this is an important factor in determining if their reconstruction was successful after 25 years.
The radiological examinations of the patients in the current study detected signs of OA in all the patients’ knees, with Ahlbäck grade I as the most common grade. There was no statistically significant difference between the 2 groups in severe radiological knee OA (P = .37). In comparison, 4 of 68 patients (6%) had radiological OA (Ahlbäck grade ≥I) preoperatively, and 34 (50%) had it after 8 years. The incidence of OA after ACL surgery has ranged from 0% to 100% in different studies. 34 However, the highest rated studies had the lowest rates of OA in patients with isolated ACL injuries. 34 Several different classifications of OA, different types of accompanying injuries, diversity in the patient population, and various follow-up lengths are probably responsible for the variation in results. As previously shown, the correlations between radiological findings and symptoms are limited. 22 However, in our study, the patients with chondral or meniscal lesions were not categorized before surgery. This could possibly have correlated with our results on radiological OA, especially because the mean time from injury to surgery was as long as 40 months. We also chose to exclude the patients with knee replacement from the radiological OA analysis. Most of these patients would probably have been Ahlbäck grade IV or V; however, these patients did not have radiographs taken that corresponded to the present study’s protocol. Based on this, a separate analysis comparing the rates of knee replacement between the BPTB group and LAD group was conducted.
In our study, 12 of 48 patients in the BPTB group and 7 of 45 patients in the LAD group had documented reruptures after 25 years (P = .40). At the 8-year follow-up, there were 11 patients with reruptures: 5 in the BPTB group and 6 in the LAD group. 7 This development shows the importance of long-term follow-up studies in this patient cohort.
One of 48 patients in the BPTB group and 6 of 45 patients in the LAD group underwent arthroplasty in the knee of interest (P = .054). There were no knee arthroplasties at the 8-year follow-up. As Oiestad et al 34 stated in a review article, the main known risk factors for OA are meniscal surgery and meniscectomy. Complete information on meniscal surgery was unfortunately not available for the present study.
In spite of several studies performed on ACL reconstruction and the use of synthetic grafts, # there are still no synthetic devices that have replaced autografts or added extra strength to grafts. The main reasons for this are complications, such as knee synovitis, effusion, and device failure. 20 In addition, synthetic grafts have shown poor long-term results. 25 The LAD was supposed to protect the graft during maturation and thus lead to improved results. This did not happen in our patient cohort. Fortunately, the LAD did not lead to side effects as reported for other devices. Some researchers 2,6,27,35 have suggested that tissue-engineered techniques will lead to a new generation of ACL replacement. These may be capable of regenerating a mechanically robust ACL. 25 As reported in a recent systematic review by van Eck et al, 47 the use of internal bracing in ACL repair may increase the success rate in young patients with acute, proximal tears. The results from our study will be important to consider as we enter a new age of replacements and augmentations.
The main aim of our study was to perform a long-term follow-up on an artificial device in ACL reconstruction. To our knowledge, this is the first study comparing a BPTB graft without augmentation with a BPTB graft augmented with a LAD with a follow-up period of more than 15 years. Some long-term studies have compared other types of ACL surgery and artificial devices. Drogset et al 9 performed a 16-year follow-up of 150 patients who underwent primary repair of the ACL and who were randomized into 3 groups: without augmentation, augmentation with the Kennedy LAD, or BPTB augmentation. BPTB augmentation was superior to augmentation with the Kennedy LAD in terms of subjective knee function and the Lachman test. The patients who underwent primary repair had 10 times more revisions than those who underwent BPTB augmentation. Therefore, the authors did not recommend this technique. In our study, we found no difference in rerupture rates between the BPTB group and the LAD group.
In another study, Ventura et al 48 described the 19-year results of 51 patients with 3 different synthetic grafts. All the grafts were made of polyethylene terephthalate and were used as prostheses in 11 of the patients and as augmentations in 40 of them. The researchers concluded that the patients had good subjective outcomes after 19 years, but through a radiological evaluation with the Ahlbäck classification, the researchers found that all patients had degenerative OA in their knee joint. Most of the patients had Ahlbäck grade III, in contrast to our study in which Ahlbäck grade I was the most common.
Most of the early results with the Kennedy LAD were satisfactory, 19,26,40 and experimental studies on cadaveric specimens and animals have been encouraging. 19,26 Some early studies had acceptable results with the Kennedy LAD when augmenting primary repair of the ACL and comparing this with nonaugmented repair. 10,17 The findings of more recent clinical studies have not encouraged the use of the device. 4,8,13,18,28 –30,33,42,43 One study evaluated the histological development of autologous grafts with and without the Kennedy LAD. 3 When autologous grafts were used together with the Kennedy LAD, they matured slower histologically than autologous grafts did on their own. The authors could not find any advantages with the use of the Kennedy LAD. 3
The Kennedy LAD was withdrawn from the market in 2000 because of unsatisfactory results. One of the more recent artificial augmentation devices introduced is made of polycaprolactone-based polyurethane, which is a degradable material in which 50% of its strength remains after 4 years. Peterson et al 37 published a long-term follow-up on 201 patients randomized to receive a BPTB autograft with or without this device. The authors could not find any significant differences between the groups with regard to clinical examination, KT-1000 arthrometer measurements, or subjective assessment findings of knee function after 4 and 12 years. There has also been a study on the suture tape technique conducted by Daggett et al, 7 which proclaimed that this type of augmentation during ACL reconstruction could reinforce and protect the ACL graft during early incorporation. The authors also believed that it could potentially strengthen the construct to reduce the chance of reinjuries in high-risk athletes. 7 This promotion of synthetic ACL products is supported by the editorial commentary of Lubowitz, 23 which stated that the future of synthetic ACLs may be more relevant than clinical nonbelievers realize.
The high follow-up participation rate of 93%, the study design, and the use of independent observers are some of the strengths of the current study. The comparability with the 2 previous follow-ups at 2 and 8 years 8,13 is another strength. However, there are some limitations to this study as well. First, we conducted telephone interviews with 11 of the 67 patients included in the follow-up examinations. These telephone interviews included the Lysholm functional score and the KOOS, which should be filled out by the patient without surgeon/clinician interference. In addition, our radiographs were taken with the Rosenberg view, which was not part of the original protocol. However, this projection is more sensitive in detecting knee joint space narrowing compared with conventional anteroposterior weightbearing projections. 11 For assessments of these radiographs, we used the Ahlbäck classification, although the scoring system has some weaknesses. 12 This system was chosen to maintain comparability with the past 2 follow-ups. 8,13 This was also the most used classification of OA 25 years ago when the first study was designed. The lack of information on meniscal injuries and surgery that the patients had undergone during the 25 years after reconstruction is another unfortunate limitation. Finally, the study was not blinded because of practical reasons and limited resources.
Conclusion
In the present study, there were no statistically significant differences between the groups in any of the outcomes. Overall, 19% of participants had reruptures, and 7% underwent knee arthroplasty 25 years after ACL reconstruction, with a tendency for more knee arthroplasties in the LAD group. All patients in both groups had signs of radiological OA; however, less than one-third of the patients in both groups had severe radiological OA.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Norwegian University of Science and Technology. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Etisk Komité.