
Abstract
Background:
Anatomic glenoid reconstruction involves the use of distal tibial allograft for bony augmentation of the glenoid surface. An all-arthroscopic approach was recently described to avoid damage to the subscapularis tendon and preserve the capsule and labrum.
Purpose:
To explore and compare change in surgical time between 2 proposed methods used for the treatment of anterior shoulder instability—arthroscopic anatomic glenoid reconstruction (AAGR) and arthroscopic Latarjet (AL)—over successive procedures. We also compared graft positioning on the anterior glenoid surface between the 2 methods.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a single-surgeon retrospective review of 54 cases of surgically treated recurrent anterior shoulder instability: 27 had AAGR with distal tibial allograft, while the other 27 had AL. AAGR with the distal tibial allograft was the primary choice for the treatment of anterior shoulder instability; however, AL was performed when tibial allograft was not available from the bone bank. Thus, there was an overlapping period for those 2 procedures. Procedure start and end times were recorded, and duration was calculated. Postoperative 3-dimensional computed tomography scans were reviewed, and graft position was judged to be in the lower third (desired position), middle third, or upper third of the anterior glenoid surface. To assess learning, these data were organized in chronological order of surgery, and each surgical cohort was divided into 3 chronological clusters of 9 patients each. Learning was assessed through change in operative time over successive clusters, change in variability of operative time among clusters, and change in graft positioning among clusters. Statistical analysis comprised a 2-tailed independent-sample t test and the Levene test for equality of variance.
Results:
Our study found that AAGR was significantly faster to perform than AL in the early (P = .001), middle (P = .001), and late (P = .05) clusters of each cohort. Duration of surgery did not significantly improve across clusters within each cohort (P = .15-.79). There were no significant changes in the variability of surgical time in the AAGR group (P = .09) or the AL group (P = .13). Desired positioning of the bone graft on the anterior glenoid surface (lower third) was identified more commonly in the AAGR cohort.
Conclusion:
AAGR is faster to learn and perform than AL for the treatment of recurrent anterior shoulder instability with significant glenoid bone loss. The current study found higher rates of desired graft positioning for AAGR clusters.
Anatomic glenoid reconstruction is a recently proposed alternative to Latarjet in the treatment of glenoid bone defects in patients with recurrent anterior shoulder instability. This procedure was initially described by Provencher and colleagues, 10 and it involves the use of distal tibial allograft to re-create a cartilaginous surface with which the humeral head may articulate. Originally, Provencher et al 10 described the postoperative outcomes of 3 patients treated for glenoid bone deficiency with this technique. A systematic review of 8 studies on anatomic allograft-based glenoid reconstruction showed that open anatomic glenoid reconstruction provides excellent clinical outcomes, with low rates of recurrent instability, high osseous incorporation, and no evidence of graft resorption (level 4 evidence). 13
Wong and Urquhart 15 recently developed an all-arthroscopic approach to anatomic glenoid reconstruction that avoids damaging the subscapularis muscle and allows for a repair of the anterior labrum and capsular tissues. Paladini and colleagues 9 found that some patients suffered weakening of the subscapularis muscle, with a positive belly-press test or positive lift-off test, following arthroscopic Latarjet (AL), which was attributed to disruption of the subscapularis muscle. Arthroscopic anatomic glenoid reconstruction (AAGR) may circumvent this problem by keeping the subscapularis muscle intact.
The AL procedure is currently used to treat glenohumeral bone loss, given its satisfactory outcome score 4 and low incidence of resorption. 16 However, this procedure is technically demanding and fraught with complications, including nonunion of the bone graft and nerve damage. 5
Glenohumeral bone loss associated with recurrent anterior instability is also managed by the arthroscopic Bankart repair technique, which attempts to tighten the anterior tissues to overcome bone loss. However, long-term recurrence rates with the arthroscopic Bankart repair for patients with significant bone loss (>25%) are still high, around 35%. 14 Additionally, the nonanatomic labral repair involved in this procedure is believed to lead to early failures. 1
AAGR may be a suitable alternative to AL for the treatment of glenohumeral bone loss in the setting of recurrent anterior shoulder instability. Its technique is nearly identical to the arthroscopic Bankart repair technique, with 1 additional medial portal created with an inside-out technique. In contrast, the AL requires 4 additional portals and a coracoid bone harvest. This difference theoretically gives AAGR an advantage in speed. Moreover, the subscapularis muscle is spared by the AAGR technique but disrupted when the AL technique is used, thus creating potential adverse changes to range of motion and strength. Finally, AAGR spares the capsule and labrum, 15 while the AL technique disrupts these structures. 7
The primary goal of this investigation was to describe a learning curve for surgeons learning AAGR and to compare it with that of AL. In our study, the learning curve was composed of change in operative time over successive procedures, change in variability of operative time over successive procedures, and technical results in the form of graft positioning on the anterior glenoid.
Methods
Ethical approval for this study was obtained from the Nova Scotia Health Authority. This was a retrospective review of 54 patients who underwent arthroscopic stabilization and bony augmentation of glenoid deficits between 2012 and 2015. These patients included 27 who were treated with AL and 27 who were treated with AAGR. The indications for either AL or AAGR were clinical and radiographic signs of shoulder instability with significant glenoid bone loss (54 patients) and failure of prior Bankart repair (18 patients). AAGR with distal tibial allograft was the priority choice for the surgeon, but AL was performed when distal tibial allograft was not available from the bone bank. Consequently, both procedures were performed during the study period. Each surgical cohort was divided into 3 clusters of 9 patients depending on the date of surgery: early (first 9 patients); middle (middle 9 patients) and last (last 9 patients).
A standard workup was performed preoperatively, including plain radiographs and a 3-dimensional computed tomography (CT) scan. Glenoid bone loss was identified by preoperative 3-dimensional CT scans for all patients. The minimum amount of bone loss was 12% for this study population, with a mean of 20%.
All operations were conducted with the patient in a lateral decubitus position and were performed by 1 shoulder arthroscopy reconstruction fellowship–trained surgeon with 9 years of practice and a surgical volume of approximately 200 shoulder arthroscopy cases per year (I.H.-B.W.). He has experience with open Latarjet and AL, and he developed the AAGR technique. 15 The technique is similar to arthroscopic Bankart repair, with 1 additional step: prior to inserting the suture anchors, 1 additional medial portal is created for inserting the bone graft. Once the quantity of bone loss was measured, distal tibial allograft was prepared to match the size of the bony defect. AL procedures were also performed in the lateral decubitus position in this study, as this technique assists with optimal placement of this graft on the native glenoid. 7
The start and end times for each surgery were recorded, and duration was calculated. Postoperative CT scans performed at 2 years after surgery were examined by a single observer (I.H.-B.W.) to assess the positioning of bone graft.
To evaluate the surgical learning curve, surgical times for AAGR and AL were recorded and organized in chronological order, and the mean surgical time was compared among clusters to assess for learning at early, middle, and late stages. Furthermore, the variability of surgical time within each cluster was assessed, and comparisons of variability were made among clusters; lower variability of operative time was judged to represent more advanced learning.
Further assessment of learning was made through a review of graft positioning on postoperative CT scans. Graft placement was judged as the middle of the graft being was centered over the lower, middle, or higher thirds of the glenoid. As the glenoid is pear shaped, with the largest part of the glenoid centered in the lower third, the attempt was made to put the bone graft in the lower third to re-create the same shape of the native glenoid. Again, each surgical cohort was divided into clusters of 9 patients, and graft positioning was compared among clusters to assess for learning.
Statistical Analysis
Two-tailed independent 2-sample t tests (at 95% CI) were performed to see the difference between the clusters of AL and AAGR. The Levene test for variance was done to see the variability of surgery duration between the clusters of AL and AAGR. Statistical analyses were performed with SPSS (v 24; IBM).
Results
The mean ± SD patient age was 29 ± 11.6 years; 79% of patients were male, and 43% of surgery was performed on the right-hand shoulder. Based on the cluster model, our analysis found that each AAGR cluster had a significantly faster mean surgical time than that of the corresponding AL cluster. The mean surgical time for the first cluster of the AAGR cohort was 1.26 ± 0.60 hours, which was significantly faster than the first cluster of the AL cohort (2.31 ± 0.44 hours; P = .001). AAGR remained significantly faster than AL when surgical times in the second and third clusters of each cohort were compared (P = .001 and .05, respectively) (Table 1).
Comparison of Surgical Duration (in Hours) Between Procedures by Cluster a
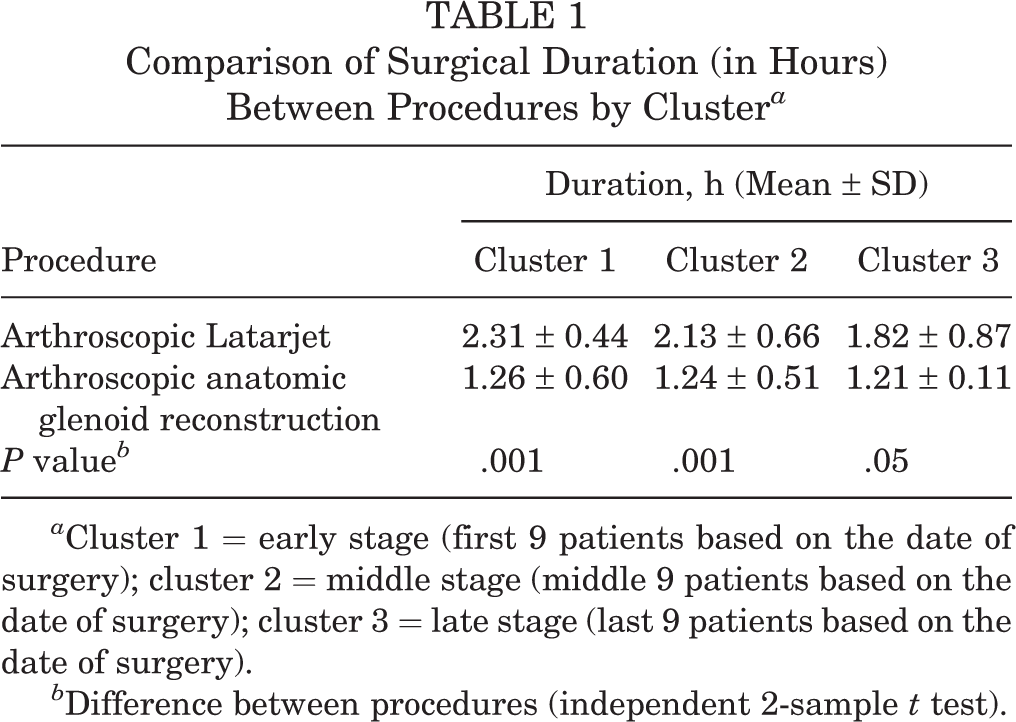
a Cluster 1 = early stage (first 9 patients based on the date of surgery); cluster 2 = middle stage (middle 9 patients based on the date of surgery); cluster 3 = late stage (last 9 patients based on the date of surgery).
b Difference between procedures (independent 2-sample t test).
We observed improvement in surgical time over successive surgery in the AAGR and AL cohorts, although the intercluster differences were not statistically significant within each cohort (P = .15-.79) (Tables 2 and 3). Regarding the variability of surgical time for each cluster within the surgical cohorts, we found no significant changes in either the AL group (P = .13) or the AAGR group (P = .09) (Tables 2 and 3, respectively).
Difference in Surgical Time Among the 3 Clusters of the Arthroscopic Latarjet Cohort

a Two-tailed independent-sample t tests were performed to identify differences between clusters.
b Levine test was performed to assess the variability of duration among the clusters (ie, equality of variance among all clusters).
Difference in Surgical Time Among the 3 Clusters of the Arthroscopic Anatomic Glenoid Reconstruction Cohort
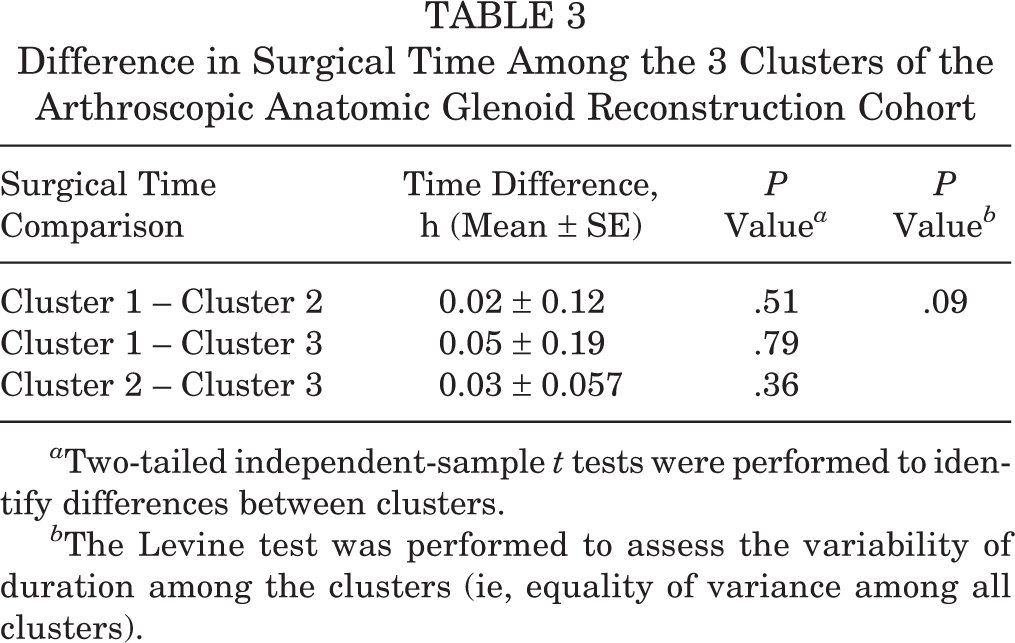
a Two-tailed independent-sample t tests were performed to identify differences between clusters.
b The Levine test was performed to assess the variability of duration among the clusters (ie, equality of variance among all clusters).
Graft positioning was assessed by postoperative CT scan (Figure 1), with positioning in the lower third of the glenoid being most desired. 11 Again, each surgical cohort was divided into equal clusters of 9 cases; within each cluster, the number of cases with final graft placement in the high, middle, or lower third of the glenoid was recorded (Table 4).

Postoperative computed tomography scan (3-dimensional) showing the graft positioning.
Graft Positioning on the Anterior Glenoid Among the 3 Clusters Between the Procedure Cohorts a

a Values are presented as n (%).
Patients in the AL surgical cohort had grafts placed in the lower third of the glenoid in 56% of cases in the early cluster; this rate increased to 78% by the middle cluster and remained stable for the late cluster. Patients in the AAGR surgical cohort had grafts placed in the lower third of glenoid in 67% of cases in the early cluster, and this rate increased to 100% for the middle and late clusters.
There was no intraoperative or immediate postoperative complication, including excessive bleeding, infection, neurovascular injury, or screw breakage in either group.
Discussion
The open Latarjet procedure is currently considered the standard of care for the management of anterior shoulder instability with significant glenoid bone loss. 8 In comparison with the open technique, the arthroscopic technique has similar excellent clinical outcomes 4,11 and less resorption. 16 However, the AL technique is not widely adopted, primarily because of the high cost, 11 the technical difficulty, and the relatively high complication rates (11% at 2 years), 6 including nonunion and nerve damage. 5
AAGR is a novel technique used to address glenoid bone loss in cases of recurrent anterior shoulder instability and is being proposed as an alternative to AL. Some of its technical advantages include preservation of the subscapularis muscle, capsule, and labrum. However, disadvantages of AAGR include the high cost of allograft, graft availability, health of articular cartilage, graft resorption, and potential disease transmission. Our study sought to determine the learning curve for AAGR, including optimization of surgical time and accuracy of graft placement on the anterior glenoid surface. We found that AAGR was faster to perform and that the optimal surgical time was more reproducible in the AAGR cohort than the AL cohort; graft placement was also more accurate in AAGR.
A notable difference between these techniques is that AAGR obviates the need for a subscapularis split; among patients who undergo AL, this split has the potential to cause postoperative subscapularis weakening with positive belly-press and lift-off tests. 9 Moreover, AAGR requires 1 new portal and uses distal tibial allograft, while AL requires 4 new portals and a coracoid bone harvest. The far medial portal used in AAGR is established with an inside-out technique and avoids major neurovascular structures, with the exception of the cephalic vein. AAGR preserves and repairs the capsule and labrum, while AL excises the capsule and labrum in most cases. 15
Our clinical study on surgical learning curves found that AAGR is faster than AL and easier to learn: operative time was significantly faster for AAGR, although the improvement in operative time was not significant. While the faster operative time is an attractive feature for surgeons considering adopting this technique, the tendency toward a consistent duration of surgery suggests that AAGR can also be more easily reproduced. This implies that intraoperative problems might be more predictable and that solutions to these problems may be more easily implemented.
Furthermore, our study found excellent rates of graft placement on the inferior one-third of the anterior glenoid surface in the AAGR cohort; accuracy of placement reached 100% in the third cluster of AAGR cases. By comparison, AL had lower accuracy rates across all clusters, reaching a maximum of 78%. The latter finding is similar to the results of a study comparing graft placement accuracy in open Latarjet versus AL 12 ; in that study, 76% of arthroscopic cases had optimal coracoid graft positioning based on postoperative CT scan. It should also be noted that in the same study, open Latarjet cases demonstrated 100% accuracy of graft placement. 12 Thus, AAGR preserves the accuracy of graft placement attained with an open procedure while providing the advantages of an arthroscopic approach. However, the factors responsible for difficulties in lower graft positioning for AL are yet to be established.
The learning curve for AL has been previously described. In a 2013 study, Castricini and colleagues 2 studied 30 consecutive AL procedures performed by a single surgical team. They divided this cohort into the first and last 15 patients and found that operative time decreased significantly from the first group to the second: 4 stages (joint evaluation, subscapularis split, coracoid harvesting, and graft fixation) were performed faster in the second group, while graft transfer took equally as long between groups. Both groups had a similar demographic composition, preoperative Rowe score, Rowe score change, and final graft placement.
Cunningham and colleagues 3 reviewed 28 AL and 36 open Latarjet procedures performed by a single surgeon, with age, sex ratio, and preoperative Instability Severity Index Scores being comparable between the groups. 3 Mean operative time was 146 ± 51 minutes for the arthroscopic group and 82 ± 24 minutes for the open group; 3 arthroscopic cases encountered technical difficulties requiring conversion to open. These results highlight the challenging nature of the AL technique and the reasons for which it is not widely adopted.
To the best of our knowledge, no other study has been published that describes the learning curve for AAGR procedure. The results obtained in this study are limited by the fact that all surgery was performed by a single surgeon who regularly performs the AL procedure, and thus, the learning curve for AAGR represented that surgeon’s transition from one technique to another. Consequently, the findings of our study cannot be generalized, as other surgeons might have different experiences in terms of learning the 2 proposed procedures. Moreover, this was a nonrandomized study with no data regarding cost and detailed clinical outcome.
Conclusion
AAGR is a potential alternative to AL for the management of glenohumeral bone loss in recurrent anterior shoulder instability. 14 Our results show that this procedure is faster to perform and easier to learn than the AL, with superior accuracy of bone graft placement in the lower one-third of the glenoid. Additional studies will need to be performed to compare the long-term outcomes of these 2 procedures for recurrent anterior instability with significant glenoid bone loss.
Footnotes
Acknowledgment
The authors acknowledge the help of Ryland Murphy for data collection and management and Jalisa den Hartog for coordinating research and work with the research ethics board.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Nova Scotia Health Authority.