
Abstract
Background:
The success of anterior cruciate ligament (ACL) reconstruction requires reliable and rigid graft fixation. Cortical suspensory fixation (CSF) devices have become an acceptable alternative to interference screws for soft tissue ACL grafts. However, CSF devices have been reported to be associated with tunnel widening and increased postoperative anterior laxity compared with interference screw fixation. Adjustable CSF devices were introduced to avoid these problems but have been associated with graft lengthening and inconsistent outcomes.
Purpose:
To (1) report the side-to-side difference (SSD) in anterior laxity at 150 N, clinical scores, and failure rates 2 years after ACL reconstruction with 4-strand semitendinosus autografts using an adjustable CSF device and (2) determine the preoperative factors associated with clinical outcomes.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 131 patients who had undergone primary ACL reconstruction, performed with 4-strand semitendinosus grafts that were secured using Pullup adjustable-length CSF devices with femoral and tibial fixation techniques, were prospectively enrolled in this study; 34 patients were excluded because of contralateral instability or ipsilateral knee injuries that required additional surgery. This left a cohort of 97 patients who were evaluated preoperatively and at 6, 12, and 24 months. The evaluation consisted of measuring the SSD in anterior laxity and patient-reported outcome scores (International Knee Documentation Committee [IKDC] and Lysholm scores). Regression analyses were performed to determine associations between these outcomes and 9 preoperative variables.
Results:
Only 2 patients could not be reached, 2 could not be evaluated because of contralateral ACL tears, and 2 had graft failure. At 2-year follow-up, the remaining 91 patients had a mean SSD in anterior laxity of 0.8 ± 1.8 mm (range, –4.2 to 5.3 mm), mean IKDC score of 87.6 ± 10.6 (range, 43.7-100.0), and mean Lysholm score of 90.8 ± 9.3 (range, 56.0-100.0). At final follow-up, compared with knees with partial ruptures, those with complete ruptures had equivalent laxity (P = .266) and Lysholm scores (P = .352) but lower IKDC scores (P = .009). Multivariable regression revealed that the IKDC score decreased with increased preoperative laxity (β = –1.35 [95% CI, –2.48 to –0.23]; P = .019).
Conclusion:
The novel adjustable-length CSF device produced satisfactory anterior laxity and clinical outcomes, with a failure rate of 2.1%, which compare favorably with those reported for nonadjustable CSF devices.
Failure rates of anterior cruciate ligament (ACL) reconstruction at 2 to 4 years range between 1.5% and 15.3% for the general population 50,52 and between 16.5% and 25.0% for patients younger than 20 years. 35,38,40 Recent prospective studies and meta-analyses have not proven that patellar tendon ACL grafts have lower failure rates than hamstring tendon grafts. 42,55,66
Numerous attempts have been made over the past decades to improve the outcomes and survival of ACL reconstruction through better understanding of ligament insertion sites, 20,58,59 more accurate tunnel placement, 60 and improvements in graft fixation techniques. 19,21,50,61 While bioabsorbable interference screws have addressed various problems of metal screws, they remain associated with graft migration, 48 cyst formation, 65 and tunnel widening, 23,39,41,54 despite the use of osteoconductive materials. 1,4,7,32,46 For these reasons, cortical suspensory fixation (CSF) devices are gradually gaining widespread use, 50 although they remain associated with tunnel widening, induced by micromotion at the bone-graft interface due to the “windshield wiper” and “bungee cord” effects, 13,14,23,36,41,54 as well as with loop lengthening. 34 Adjustable-length CSF devices have aimed to avoid some of these problems by enabling fine-tuning of graft tension intraoperatively. 41,57
Recent laboratory biomechanical studies have reported lengthening of adjustable CSF devices, 47,51 although this may not be observed in clinical settings, where rapid graft osteointegration can prevent postoperative lengthening. Furthermore, newer adjustable-length CSF devices have been developed to prevent lengthening and have demonstrated good graft incorporation at 6 months with minimal tunnel widening, 17,19 although their midterm clinical outcomes have not yet been reported.
The goals of this prospective cohort study were to (1) report the side-to-side difference (SSD) in anterior laxity, clinical scores, and failure rates 2 years after ACL reconstruction with 4-strand semitendinosus (4ST) autografts using an adjustable CSF device and (2) determine the preoperative factors associated with clinical outcomes. The hypothesis was that, at 2 years, the novel adjustable CSF device would grant adequate improvements over baseline functional scores and laxity, comparable with those reported in the literature for nonadjustable CSF devices.
Methods
Study Design
We prospectively enrolled 131 consecutive patients who underwent primary ACL reconstruction between June 2014 and February 2015. All patients had subjective instability and functional impairment, confirmed by a positive Lachman test and/or pivot-shift test finding. All operative procedures were performed by the senior surgeon (P.C.) with 4ST grafts that were secured using Pullup (SBM) adjustable CSF devices at both the femur and tibia. Early radiographic and clinical results were published for the device at 6 months postoperatively, including the SSD in anterior laxity, International Knee Documentation Committee (IKDC) scores, tunnel widening, and graft ligamentization. 19 The institutional review board approved this study in advance, and all patients provided written informed consent for the use of their data and images for research and publishing purposes. A total of 34 patients were excluded because they had unstable contralateral knees (n = 25) or concomitant peripheral ligament injuries that required additional surgery (n = 9), leaving a study cohort of 97 patients (Figure 1).

Flowchart of patients enrolled in the study.
Surgical Technique
All patients were operated on using the same surgical technique in the supine position, under general anesthesia and ultrasound-guided femoral nerve block, with a pneumatic tourniquet at the base of the thigh (300 mm Hg). 18 The semitendinosus was extracted using a tendon harvester (ConMed), folded into 4 loops, and stitched along its entire length using resorbable suture. The resulting hamstring tendon graft was tensioned at 50 N on a graft preparation station (GraftTech) to form a 4-strand graft (Figure 2). The graft was then passed through 2 Pullup adjustable CSF devices: the first with an 8-mm femoral cortical plate and the second with a larger 12-mm tibial cortical plate. Two incisions were made: anterolateral for the arthroscopic portal and anteromedial for the instruments. A single-bundle anatomic technique was used. With the knee flexed at 120°, the femoral tunnel was drilled from inside-out, leaving a socket 25 mm deep, and was always centered on the anteromedial fibers of the native ACL, behind the intercondylar ridge and 1 cm above the top of the posterior condylar cartilage. 18,58 The tibial tunnel was drilled from outside-in, without a socket, and at the center of the anteromedial bundle footprint. The graft was then placed within the tunnels by pulling it from the tibia to the femur. After ensuring that the femoral cortical plate had correctly flipped, the sutures on the femoral side were fully tightened to approximately 100 N (Figure 3). Next, the sutures of the tibial cortical plate were partially tightened using a moderate force of 20 N with the knee flexed at 90°. Finally, the knee was flexed and extended through 5 to 10 cycles to adjust graft placement and tensioning, and the device was fully tightened at full extension.
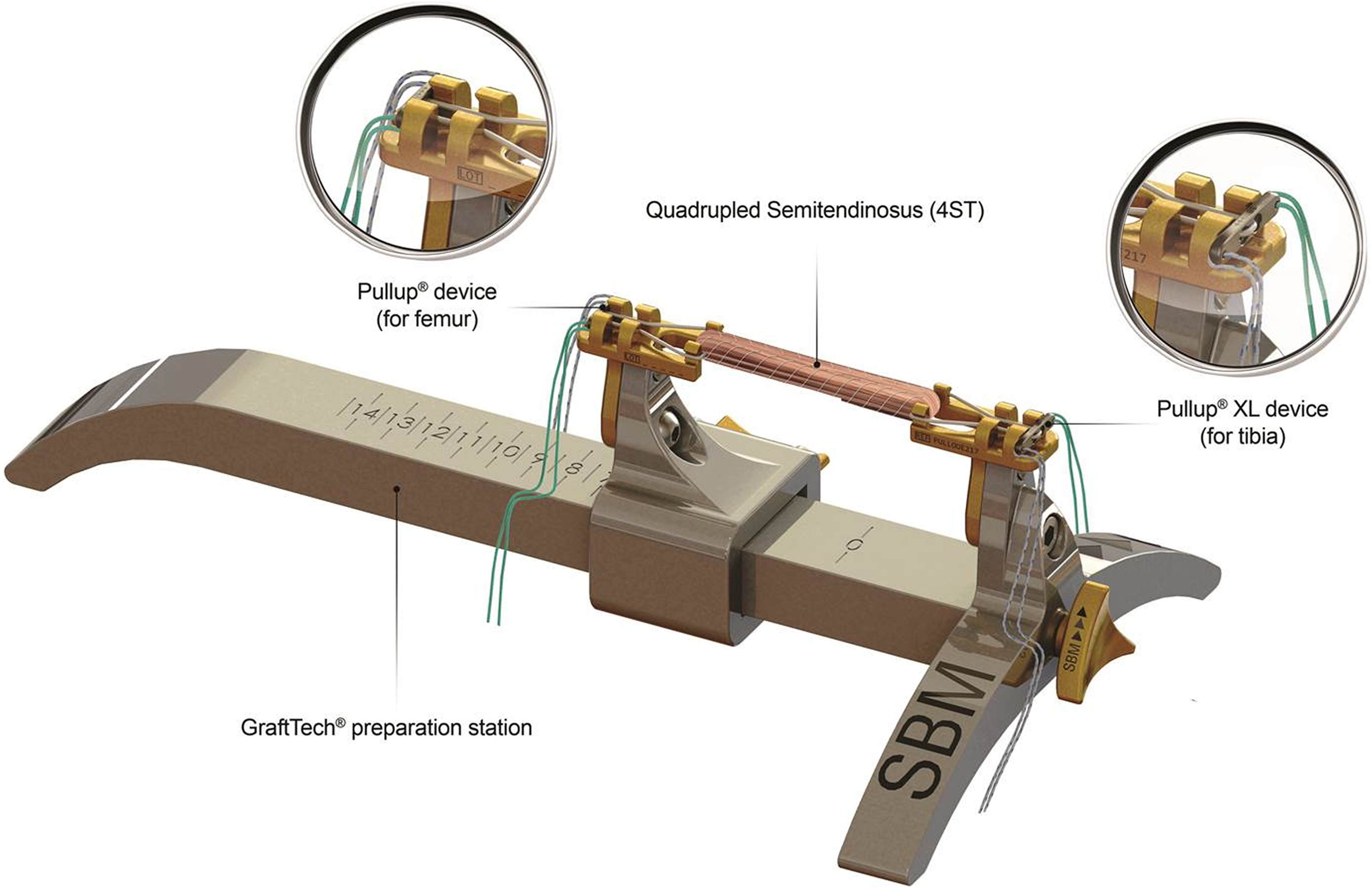
Image of the GraftTech preparation station used to tension the graft and install it on the suspension device.

Drawing of the graft after installation.
Rehabilitation Protocol
All patients followed the same nonaggressive rehabilitation protocol, with immediate partial weightbearing on crutches, a fully mobile brace, and full range of motion. The brace was removed after 3 weeks and the crutches removed after 4 weeks. Driving was permitted after 5 weeks, cycling and swimming after 6 weeks, and jogging after 3 months. Noncontact pivoting sports were allowed after 6 months, and pivoting contact sports were allowed after 9 months.
Clinical Evaluation
Patients underwent a clinical evaluation preoperatively and at 6 months, 1 year, and 2 years after surgery. The ACL remnants were assessed on preoperative magnetic resonance imaging (MRI) and arthroscopically to distinguish between complete tears and partial tears. Partial tears had at least 1 ACL bundle intact but were all deemed dysfunctional because of limited resistance to anteroposterior forces and/or rotational moments. The SSD in anterior laxity was measured by an independent blinded operator (N.B.) using the GNRB system 9,31,53 (Genourob). The GNRB system uses a transducer to measure anterior translation of the tibial tuberosity relative to the femur in 20° of flexion when an increasing calibrated anterior force is applied. The values reported here represent anterior translation under a constant force of 150 N. The SSD in anterior laxity was calculated by subtracting anterior laxity of the injured/operated (ipsilateral) knee from that of the healthy (contralateral) knee. In our practice, more than 3 mm of SSD is considered high but does not necessarily indicate an ACL tear or graft failure. Rather, graft failure is suspected if combined with a positive Lachman test and/or pivot-shift test and is validated on MRI. Subjective and objective IKDC and Lysholm scores were collected at each clinical evaluation. In addition, the Tegner score was collected at final follow-up. In knees suspected to have graft failure, MRI and a positive pivot-shift test were used to confirm the diagnosis.
Statistical Analysis
Descriptive statistics were used to summarize the data. The Shapiro-Wilk test was used to assess the normality of distributions. For non-Gaussian quantitative data, differences between groups were evaluated using the Wilcoxon rank-sum test (Mann-Whitney U test). For non-Gaussian categorical data, differences between groups were evaluated using the Fisher exact test. Univariable and multivariable regressions were performed to determine associations between 3 outcomes (postoperative SSD in anterior laxity, IKDC score, and Lysholm score) and 9 independent variables (age, sex, preoperative sports level, preoperative knee laxity, partial vs complete rupture, graft diameter, time from injury to surgery, and presence of medial or lateral meniscal lesions). With a sample size of 97, our regression models were deemed sufficiently powered, considering the recommendations of Austin and Steyerberg 5 of 10 participants per variable. Statistical analyses were performed using R version 3.3.2 (R Foundation for Statistical Computing). P values <.05 were considered statistically significant.
Results
The final cohort of 97 patients comprised 33 women (34%) and 64 (66%) men, with a mean age of 30.9 ± 10.7 years (range, 14.8-56.1 years) (Table 1). Their mean body mass index (BMI) was 24.6 ± 3.9 kg/m2 (range, 17.6-38.3 kg/m2), and the mean time from injury to surgery was 26.4 ± 64.7 months (range, 0.3-321.4 months). About half (56%) of the patients practiced sports competitively. The mean graft diameter was 8.8 ± 0.6 mm (range, 7.5-10.5 mm) (Table 2). At final follow-up, 2 patients could not be reached, 2 could not be evaluated because of contralateral ACL tears, and 2 had graft failure (2.1%). Both of the patients with graft failure underwent a reoperation (see Figure 1). Both were young male patients who practiced sports at competitive levels and had graft damage as observed on MRI, and both patients had complete ACL tears with no meniscal lesions and underwent surgery within 3 months from injury, with preoperative laxity of 6.3 mm and 4.0 mm, respectively. The first patient was a 15-year-old soccer player with a BMI of 23.8 kg/m2 who had graft failure 4 months postoperatively, likely because he returned to sport sooner than authorized. The second patient was a 17-year-old rugby player with a BMI of 31.1 kg/m2 who had graft failure 26 months postoperatively.
Patient Demographics a

a Data are presented as n (%) unless otherwise specified. ACL, anterior cruciate ligament.
Clinical Outcomes a

a Data are presented as mean ± SD (range). IKDC, International Knee Documentation Committee.
For the remaining 91 patients, the mean SSD in anterior laxity improved from 3.1 ± 2.0 mm (range, 0.1 to 9.8 mm) to 0.8 ± 1.8 mm (range, –4.2 to 5.3 mm), and all patients had a negative pivot-shift test. The mean subjective IKDC score improved from 60.4 ± 15.0 (range, 33.3-95.4) to 87.6 ± 10.6 (range, 43.7-100.0) and the mean Lysholm score from 75.6 ± 13.0 (range, 44.0-100.0) to 90.8 ± 9.3 (range, 56.0-100.0).
The SSD in anterior laxity was significantly lower at 6 months after surgery (P < .001) and did not change thereafter (see Figure 4). In contrast, both clinical scores continued to improve from 6 months to 1 year after surgery, after which they remained stable. An assessment of the IKDC score subcomponents (Figure 5) revealed a general improvement after surgery, with the patients reaching “A” grades in 97.5% of the cases for mobility, 94.9% for laxity, 97.6% for the hop test, and 86.1% for the global score at 2 years. The IKDC hop test score, unlike the IKDC mobility and laxity scores, which peaked at 6 months, improved continuously between 6 months and 2 years after surgery. At 2 years, patients with preoperative complete ACL ruptures had an equivalent SSD in anterior laxity (P = .266) and Lysholm scores (P = .352) to patients with preoperative partial tears but lower IKDC scores (P = .009) (Figure 6).
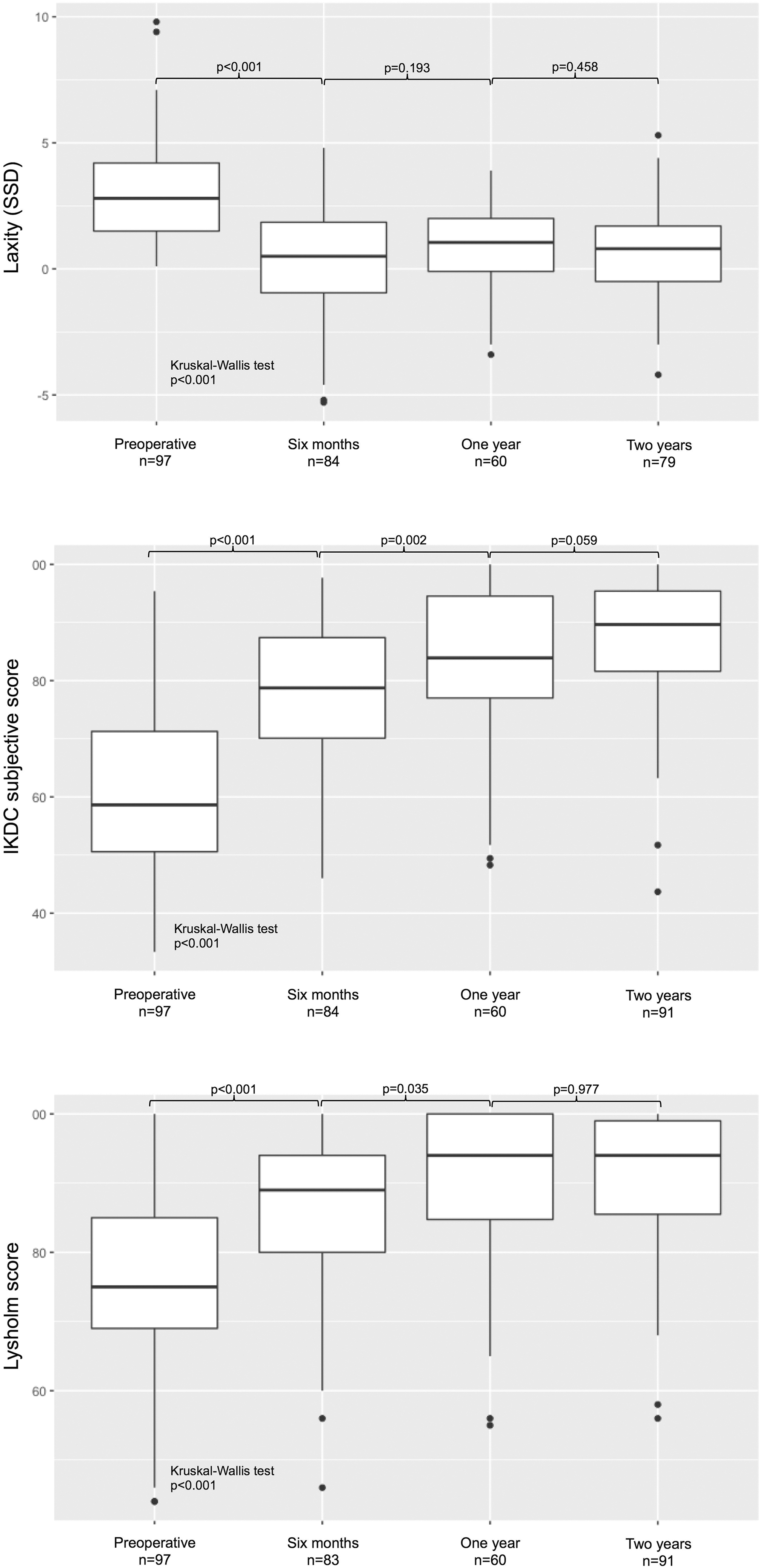
Box plots indicating improvements in knee laxity and clinical scores at different follow-up visits. P values indicate the significance of overall trends (Kruskal-Wallis test) as well as differences between consecutive follow-up visits (Mann-Whitney test). Dots indicate outliers. SSD, side-to-side difference.
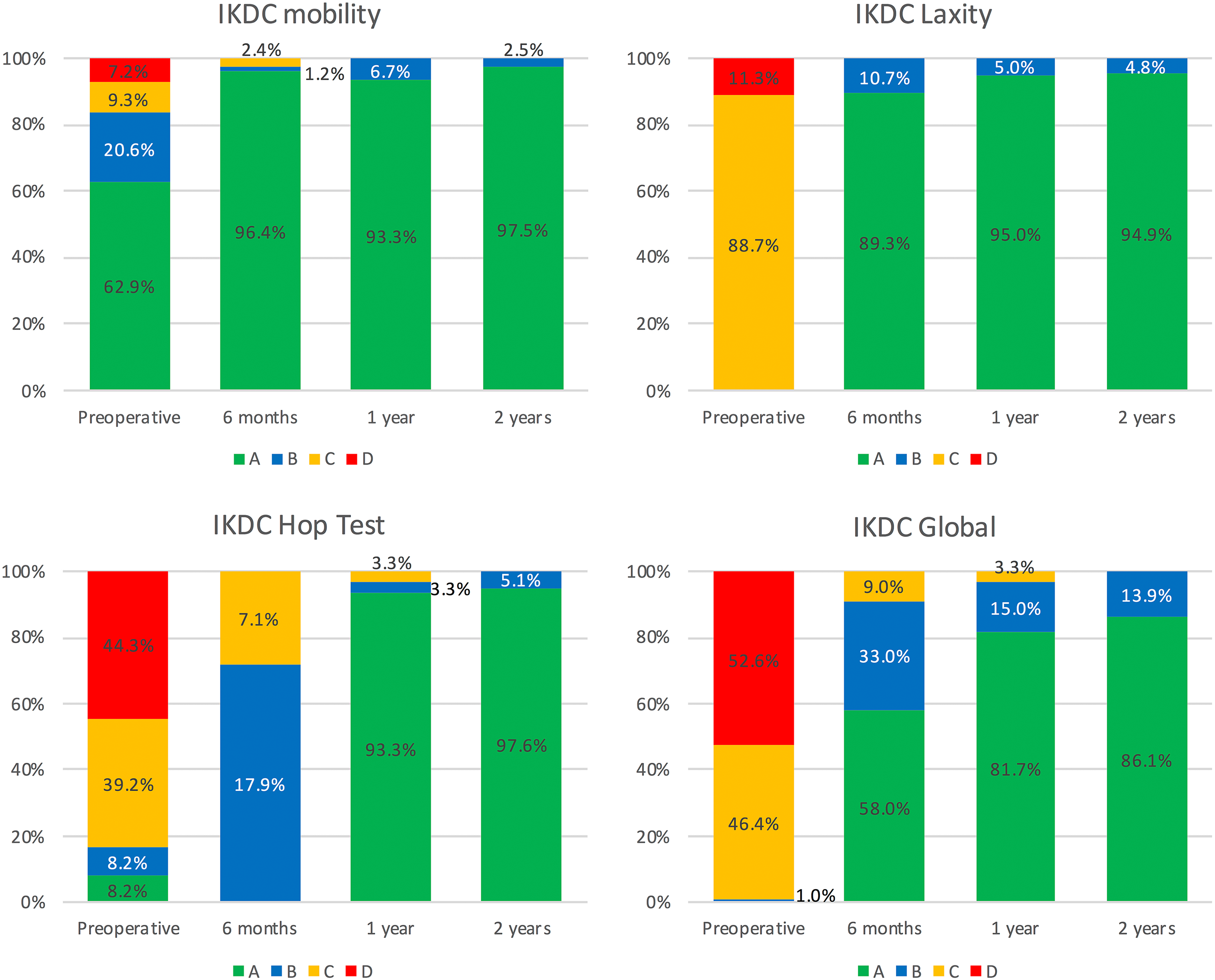
Bar charts indicating improvements in various subcomponents of the International Knee Documentation Committee (IKDC) score at different follow-up visits: A, normal (green); B, nearly normal (blue); C, abnormal (yellow); and D, severely abnormal (red).

Box plots comparing 2-year knee laxity and clinical scores for patients with partial or complete anterior cruciate ligament ruptures. P values indicate the significance of differences between the 2 groups (Mann-Whitney test). Dots indicate outliers. IKDC, International Knee Documentation Committee; SSD, side-to-side difference.
Multivariable regression revealed that postoperative 2-year anterior laxity was independent of all demographic and perioperative variables tested (Table 3). In contrast, the IKDC score decreased with increasing preoperative laxity (regression coefficient [β] = –1.35 [95% CI, –2.48 to –0.23]; P = .019) (Table 4), and the Lysholm score tended to increase with the presence of medial meniscal lesions before surgery (β = 4.60 [95% CI, 0.08 to 9.13]; P = .046) (Table 5).
Linear Regression to Identify Factors Associated With SSD in Anterior Laxity at 2 Years a

a ACL, anterior cruciate ligament; SSD, side-to-side difference.
b Expected difference.
c Excluded from the multivariable model because of excessive collinearity with preoperative laxity.
Linear Regression to Identify Factors Associated With IKDC Subjective Score at 2 Years a
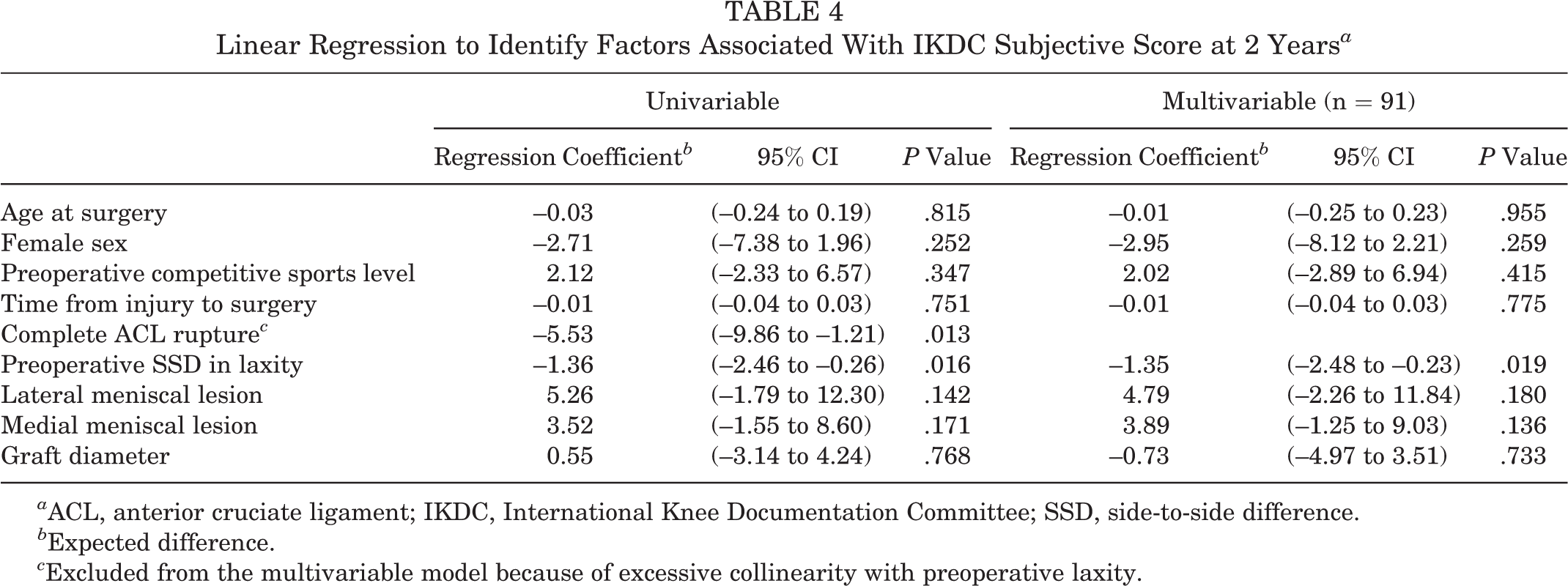
a ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; SSD, side-to-side difference.
b Expected difference.
c Excluded from the multivariable model because of excessive collinearity with preoperative laxity.
Linear Regression to Identify Factors Associated With Lysholm Score at 2 Years a
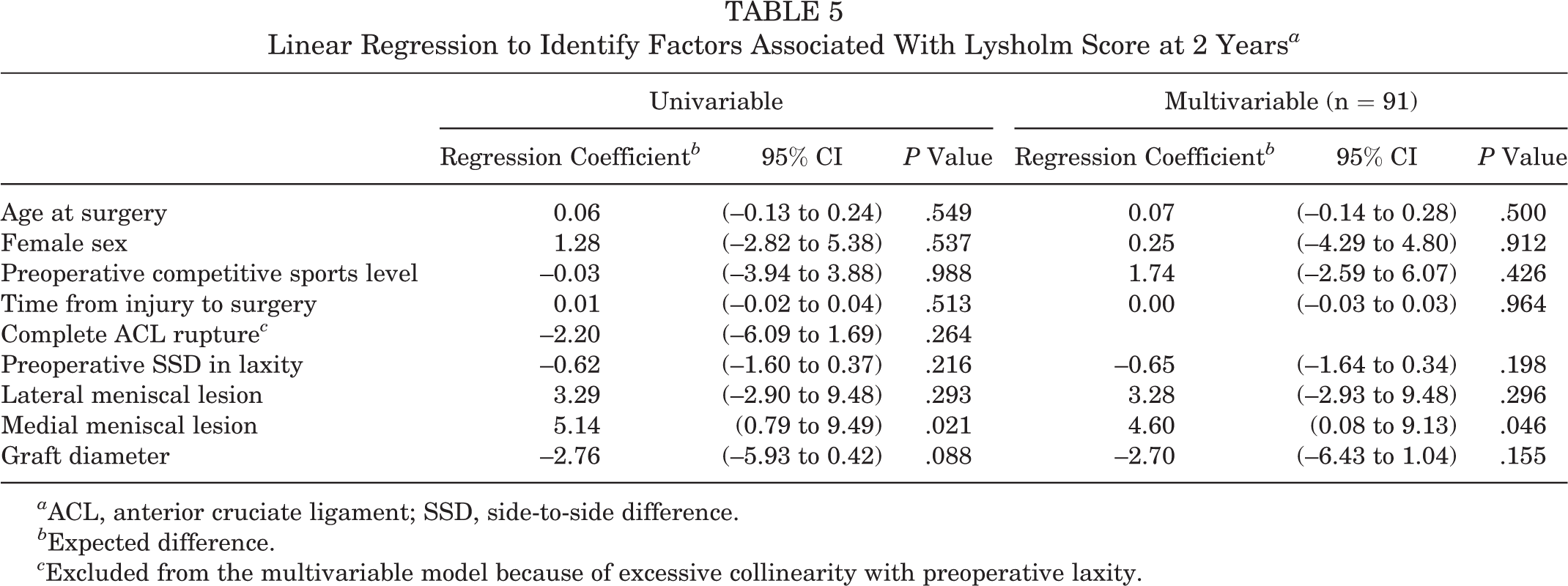
a ACL, anterior cruciate ligament; SSD, side-to-side difference.
b Expected difference.
c Excluded from the multivariable model because of excessive collinearity with preoperative laxity.
Discussion
Graft fixation devices are important for the success of ACL reconstruction with hamstring tendon autografts. 19,21,42,50,55,61,66 Fixed-length CSF devices are frequently used but are associated with tunnel widening, induced by micromotion at the bone-graft interface. 14,36,41 Adjustable CSF devices aim to solve these problems but have rendered mixed short-term outcomes and have been suspected to lengthen after surgery, 47,51 thus increasing the risks of residual laxity and graft failure. The purpose of this study was therefore to report anterior laxity, clinical scores, and failure rates after ACL reconstruction with 4ST autografts, which were attached at both the femur and tibia using a novel adjustable CSF device. At 2 years, our series had a mean anterior laxity of 0.8 mm and satisfactory clinical scores, with a failure rate of 2.1%.
Our results confirm the hypothesis that the outcomes of the novel adjustable CSF device compare favorably with those reported in the literature for fixed-length CSF devices § and with those of other adjustable CSF devices 8,10,11,15,23,57,68 (Table 6). While most published studies reported anteroposterior laxity measured using different techniques and forces, our series was measured using one of the most reproducible systems (GNRB), 9,31,53 which applied a constant calibrated force of 150 N. Our postoperative anterior laxity was considerably lower than most values reported in the literature, including series that measured laxity at lower forces. Our subjective IKDC and Lysholm scores were also consistent with those of other CSF devices. Our failure rate of 2.1% is the lowest among studies that reported failure rates at ≥2 years for cohorts larger than 40 patients. While the precise cause of our 2 graft ruptures cannot be confirmed, the patients had typical risk factors: young age, male sex, competitive sports practiced, and relatively high preoperative laxity. It is possible that these graft failures could have been avoided by a more gradual and monitored return to sport.
Outcomes of Anterior Cruciate Ligament Reconstruction Using Adjustable and Nonadjustable CSF Devices Reported in Recent Literature a

a CSF, cortical suspensory fixation; IKDC, International Knee Documentation Committee; SSD, side-to-side difference.
b With 150-N force.
c With maximum manual force.
d With 134-N force.
e With 89-N force.
f With 200-N force.
In 2017, a meta-analysis 12 found that, compared with aperture fixation, suspensory fixation is more reliable for laxity correction, offering comparable clinical scores and lower failure rates. In 2018, a study using the Scandinavian knee ligament registries 49 reported 2-year revision rates for CSF devices of around 2.7% for the femur and 2.8% for the tibia. In 2018, Eysturoy et al 22 reported the failure rates of ACL reconstruction with hamstring tendon grafts in the Danish registry for using all major fixation devices. They found that adjustable CSF devices lower the relative failure risk (hazard ratio [HR], 0.96) at 2 years compared with nonadjustable CSF devices (HR, 1.24) and interference screw fixation (HR, 1.28). Therefore, our comparisons with the literature are consistent with the conclusions of recent reviews and registry studies. 12,22,49
The use of adjustable CSF devices at both the femur and tibia enables ACL reconstruction with short grafts, which have the potential benefits of preserving the gracilis, thereby reducing morbidity of the flexor muscles and adapting the graft diameter to patients’ needs and morphology, thus resulting in more conservative use of harvested collagen and sparing bone that would be sacrificed with interference screws. Conversely, adjustable CSF devices have been criticized in biomechanical studies, which have suggested that adjustable loops could loosen after surgery and thus increase postoperative laxity or early failure rates. 47,51 In our series, postoperative laxity and failure rates were relatively low compared with other suspension devices. Further, we found that postoperative laxity remained stable after the first 6 months after surgery, while clinical scores continued to improve. This suggests that the novel device used in this study offers stable graft fixation and prevents lengthening, or that any potential lengthening is not clinically detectable or relevant.
Regression analyses revealed that postoperative laxity was independent of demographic and preoperative factors considered. Moreover, compared with knees with partial ACL ruptures, those with complete ACL ruptures had equivalent postoperative laxity, although they had lower IKDC scores. The IKDC score was, in fact, associated with preoperative laxity, with a regression coefficient of –1.35. Considering that the maximum preoperative laxity was 9.8 mm, the maximum associated decrease in the IKDC score would be 13 points, which is within the range of the minimal clinically important difference reported for this score (11.5 to 20.5 points depending on surgical procedure). 16 Unlike often reported in the literature, 2,3,37,67 we did not find meniscal lesions to affect the outcomes of ACL reconstruction in our series. The Lysholm score was even significantly better for knees with medial meniscal lesions. While we cannot explain this unexpected trend, it is not clinically relevant and could be related to a confounder that we did not adjust for.
The main limitation of this study is the lack of a control group, rendering a direct comparison with other suspension devices difficult. Nevertheless, the literature presents a large number of heterogeneous studies reporting a range of 2-year outcomes, in light of which our results remain favorable. Second, the follow-up period was relatively short at 2 years. However, the literature reports that a large proportion of graft failures occur within the first 2 years after surgery, and this time point is widely used to compare fixation devices. 33,43,64 Finally, there was no radiographic analysis of tunnel widening at follow-up, and it is unknown whether the novel suspension device improves upon classic devices in this regard. Despite these limitations, the present study is the first to report the outcomes of ACL reconstruction using a novel adjustable CSF device, which exhibited encouraging short-term results. In addition, the relatively large cohort compares well with other recent studies and reduces the risk that our study was underpowered.
Conclusion
At 2 years, ACL reconstruction using the novel adjustable CSF device granted a mean SSD in anterior laxity of 0.8 mm and satisfactory clinical scores, with a failure rate of 2.1%. The novel device appeared to prevent postoperative lengthening, and its outcomes compare favorably with those reported for nonadjustable CSF devices.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: P.C. receives royalties from SBM France. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Patient Protection Committee, South Mediterranean Region (IV), France (ID-RCB 2017-A00610-53).