
Abstract
Background:
Currently, clinical physical examination maneuvers alone provide variable reliability in diagnosing full-thickness rotator cuff tears (RCTs).
Purpose:
To assess the diagnostic accuracy of the scapular retraction test (SRT) to predict full-thickness RCTs.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
A total of 331 patients were prospectively evaluated in this cohort study. SRT was performed to assess the status of the rotator cuff. A positive SRT indicates an intact rotator cuff, and a negative SRT indicates a full-thickness RCT. Magnetic resonance imaging (MRI) was used as the gold standard. The examiner was blinded to the results until completing the physical examination. Statistical analysis was performed to assess the sensitivity, specificity, accuracy, positive and negative predictive values, and positive and negative likelihood ratios of the SRT.
Results:
The prevalence of full-thickness RCTs diagnosed on MRI was 54.4% (180 of 331). Among the 180 patients with an MRI-confirmed full-thickness RCT, the SRT was negative for 147. Of 150 patients with an intact rotator cuff by MRI, 122 had a positive SRT. In diagnosing full-thickness RCTs, the SRT had a sensitivity of 81.7% (95% CI, 77.2%-85.4%), specificity of 80.8% (95% CI, 75.5%-85.3%), and accuracy 81.3%. The positive predictive value was 83.5% (95% CI, 78.9%-87.4%); the negative predictive value, 78.7% (95% CI, 73.5%-83.1%); the positive likelihood ratio, 4.3 (95% CI, 3.1-5.8); the negative likelihood ratio, 0.23 (95% CI, 0.17-0.30); and the diagnostic odds ratio, 18.7 (95% CI, 10.4-34.0).
Conclusion:
The results of this diagnostic study indicate that the SRT can accurately be used to clinically assess the status of the rotator cuff. This physical examination maneuver was found to be accurate, sensitive, and specific in diagnosing full-thickness RCTs. Additionally, our results indicate that it is equally as accurate to predict an intact rotator cuff tendon. Providing an accurate, reliable, and reproducible physical examination test will allow clinicians to diagnosis the integrity of the rotator cuff and will help guide treatment recommendations.
Keywords
Shoulder pain generated from underlying rotator cuff pathology is commonly seen clinically. This pain can stem from myriad issues, including rotator cuff tendinopathy, partial- or full-thickness rotator cuff tears (RCTs), or long head of biceps pathology, among others. At times, classic clinical findings are seen—for example, a patient with a traumatic full-thickness RCT who presents after a fall and has lag signs and pseudoparalysis upon examination. More frequently, however, physical examination maneuvers alone may still limit the ability to make a definitive diagnosis of the integrity of the rotator cuff. This leads physicians to rely on advanced imaging, such as magnetic resonance imaging (MRI) or ultrasound, to determine the status of the rotator cuff tendons.
Many physical examination maneuvers have been utilized to determine the status of the rotator cuff to aid in diagnostic and therapeutic decisions. 1,3,5,12,14,15,18,20 Litaker et al 11 demonstrated that weakness with external rotation (odds ratio, 6.96), age >65 years (odds ratio, 4.05), and symptoms of night pain (odds ratio, 2.61) together best clinically predicted the presence of a full-thickness RCT. Other commonly used physical examination maneuvers that contribute to the diagnosis of a full-thickness RCT include the empty can test, 5 full can test, 5 drop arm sign, external rotation lag sign, 2 Hawkins sign, 3,4,6 and painful arc test. 1,3,4,6 Amid current literature, these maneuvers have demonstrated variable and inconsistent results with regard to sensitivity, specificity, and positive and negative predictive values, as well as accuracy in diagnosing full-thickness RCTs. 1 –6,14,18
Kibler et al 8 described the scapular retraction test (SRT) in an attempt to demonstrate that patients with concomitant rotator cuff dysfunction and scapular dyskinesis could have improvement of supraspinatus strength deficits through stabilization of the scapula in a retracted position. A protracted scapular position was shown to decrease rotational strength of the shoulder, which corroborates these findings. 16 The test is performed through stabilization of the scapula in a retracted position, in conjunction with standard manual supraspinatus muscle strength testing with the empty can test, with the arm in the plane of the scapula. A positive test correlates with scapular dyskinesis, demonstrating an improvement in supraspinatus strength as compared with the empty can test without scapular stabilization. 7,9
The purpose of this study was to examine the use of the SRT as a clinical examination diagnostic tool to accurately identify the presence of full-thickness RCTs. We hypothesize that the SRT will be highly sensitive, specific, and accurate in diagnosing full-thickness RCTs.
Methods
With institutional review board approval, we performed a prospective diagnostic accuracy cohort study based on data from patients who presented with shoulder pain at an academic institution from September 2013 through February 2016 (N = 331). Patients with a diagnosis of calcific tendinitis, adhesive capsulitis, or glenohumeral osteoarthritis or a history of shoulder surgery were excluded from the study.
As part of the physical examination, the SRT as described by Kibler et al 8 was performed to assess the status of the rotator cuff. Our preferred method for performing the SRT involves first performing the traditional empty can test with the patient’s shoulder internally rotated, flexed to 90°, and abducted collinear with the scapular axis, at which point the patient is instructed to resist downward pressure by the examiner. The test is then repeated, this time with additional manual stabilization of the patient’s medial scapular border with the volar aspect of the examiner’s forearm and fingers cupped firmly over the anterior shoulder at the clavicle (Figure 1).

Clinical photograph demonstrating the scapular retraction test. The examiner retracts the scapula, placing the forearm against it for support. To perform manual muscle strength testing, the patient’s arm is forward elevated in the plane of the scapula, with downward force applied by the examiner.
A positive SRT was defined as restoration of strength with the scapula held retracted and the arm in the abducted forward-flexed position in the plane of the scapula. Restoration of strength was defined as the patient being able to resist the examiner’s downward force in the empty can position (ie, no strength deficit or improvement to full rotator cuff strength in this position). A negative SRT was defined as continued weakness or the arm dropping. Based on these findings, a positive SRT indicates an intact rotator cuff, and a negative SRT indicates a full-thickness RCT.
MRI was used as the gold standard to confirm the status of the rotator cuff (intact or torn). All examinations were performed by a single fellowship-trained shoulder surgeon (M.K.) who had been using the SRT as part of the clinical shoulder examination for 10 years. The examiner was blinded to the MRI findings until the physical examination was completed. A 2 × 2 table was created to calculate sensitivity, specificity, diagnostic accuracy, positive and negative predictive values, as well as positive and negative likelihood ratios, with their respective CIs. The statistical analysis was performed with GraphPad Prism statistics software (v 7; GraphPad Software).
Results
The 331 shoulders evaluated were divided into 2 groups based on their MRI findings, with either the presence or absence of a full-thickness RCT (Table 1).
Demographic Composition of the Case-Control Groups a

a MRI, magnetic resonance imaging; SRT, scapular retraction test.
The prevalence of full-thickness RCTs diagnosed on MRI in the study population was 54.4% (180 of 331). Of these 180 patients, 80 were men and 100 were women, with a mean age of 54.3 years. The SRT was positive for 33 (18.3%) MRI-confirmed full-thickness RCTs and negative for 147 (81.7%).
The control group consisted of the remaining 151 patients, diagnosed with an intact rotator cuff. Given the difficulty and poor agreement in classifying partial-thickness RCTs, we categorized any MRI finding that did not indicate a full-thickness tear as an “intact tendon.” The mean age of this group was 54.6 years, with 74 men and 77 women; of these patients, 122 (80.8%) demonstrated a positive SRT and 29 (19.2%) had a negative SRT (Table 2).
SRT and MRI Findings a
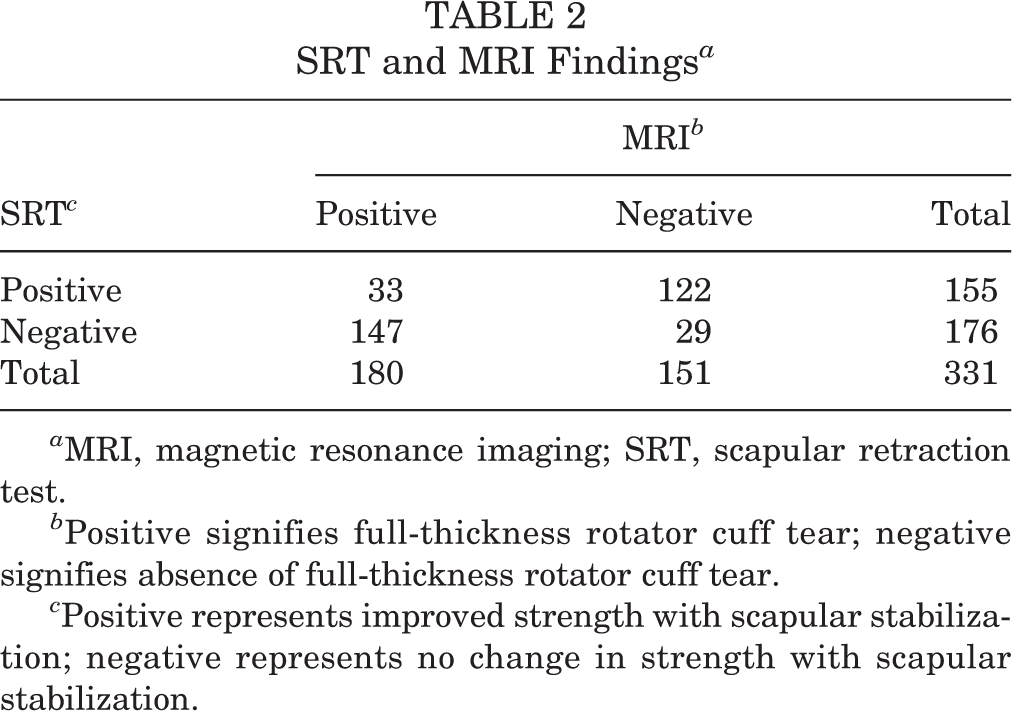
a MRI, magnetic resonance imaging; SRT, scapular retraction test.
b Positive signifies full-thickness rotator cuff tear; negative signifies absence of full-thickness rotator cuff tear.
c Positive represents improved strength with scapular stabilization; negative represents no change in strength with scapular stabilization.
Statistical analysis demonstrated a sensitivity of 81.7% (95% CI, 77.2%-85.4%), a specificity of 80.8% (95% CI, 75.5%-85.3%), and an accuracy of 81.3% for the SRT in diagnosing full-thickness RCTs. The positive predictive value was 83.5% (95% CI, 78.9%-87.4%); the negative predictive value, 78.7% (95% CI, 73.5%-83.1%); the positive likelihood ratio, 4.3 (95% CI, 3.1-5.8); the negative likelihood ratio, 0.23 (95% CI, 0.17-0.30); and the diagnostic odds ratio, 18.7 (95% CI, 10.4-34.0) (Table 3).
Statistical Validity of the SRT to Diagnose Full-Thickness Rotator Cuff Tears a

a SRT, scapular retraction test.
Discussion
Scapular dyskinesis describes the complex alteration of scapular motion and positional control attributable to a number of factors. 19 The SRT was developed to help differentiate shoulder weakness attributable to scapular dyskinesia. Improvement in demonstrated supraspinatus strength upon scapular stabilization versus the empty can test without such stabilization denotes a positive test and suggests scapular dyskinesis. A negative test therefore represents no improvement in supraspinatus strength in the aforementioned clinical scenario and is found for patients with a full-thickness RCT. The purpose of this study was to determine if this clinical examination maneuver, reflected by a negative SRT result, could accurately diagnose full-thickness RCTs.
While not perfect, a sensitivity of 81.7% and a specificity of 80.8% and the corresponding positive and negative likelihood ratios of 4.25 and 0.23, respectively, are not clinically insignificant. These results are comparable with statistical findings in the literature for other RCT diagnostic physical examination tests. 5,6,15 These results indicate that the SRT can both identify and rule out full-thickness RCTs with good reliability. Similarly, respective positive and negative predictive values of 83.5% and 78.7% contribute to an overall test accuracy of 81.3%. A negative predictive value of 78.7% represents a respectable proportion of positive SRTs (improvement in rotator cuff strength testing) correlating with an absence of full-thickness tear on MRI. Interestingly, while not an intended initial finding of the study, the high negative predictive value indicates that the SRT is equally as accurate in predicting an intact rotator cuff tendon as it is in predicting a full-thickness RCT. For the purpose of this study, an MRI finding of a partial-thickness RCT was considered equivalent to an intact rotator cuff and was categorized accordingly. Given the poor reliability and difficulty in classifying the severity of partial-thickness RCTs on imaging, we thought that by dichotomizing the integrity of the rotator cuff tendon (either full-thickness tear or intact tendon), the study design would control for this variability. Additional analysis could be performed to evaluate the accuracy and validity of the SRT in the setting of a partial-thickness RCT, but this is beyond the scope of the present research question. Several studies have demonstrated the limitations in reliably predicting and diagnosing the degree and severity of partial-thickness RCTs with MRI or arthroscopy. 10,17
To our knowledge, no prior study has evaluated the accuracy of the SRT as an adjunct in clinically diagnosing full-thickness RCTs. Rather, the literature definitively demonstrated an association with altered scapular kinematics among patients with rotator cuff pathology. 8,13 The results of this diagnostic study suggest that the SRT can accurately be used to assess the status of the rotator cuff, providing a simple and useful addition to shoulder examination maneuvers available to the clinician. A meta-analysis by Hegedus et al 3 in 2012 concluded that no single shoulder examination maneuver could be unequivocally recommended as being pathognomonic for diagnosing RCTs. While we agree that no test in isolation can definitively diagnose full-thickness RCTs, the accuracy and predictive nature of the SRT amplify a physician’s clinical suspicion with the addition of a simple examination maneuver conducted in the outpatient setting.
Future studies need to be performed that will the sensitivity, specificity, predictive values, likelihood ratios, and odds ratio of the SRT coupled with a group of other common physical examination tests used to clinically diagnose full-thickness RCTs.
A limitation of this study is that all physical examinations were performed by a single fellowship-trained shoulder surgeon, and while this provides examination maneuver consistency, the reproducibility is unknown. Further analysis of interrater reliability and incorporation of multiple surgeons and/or centers would be useful in validating the reliability and accuracy of the SRT to assess the integrity of the rotator cuff. We did not perform an a priori power analysis for this investigation, but given the sample size in each group, we do not think that our results would suffer from being underpowered. Additionally, we did not assess the impact of the status of the long head biceps, superior labrum, adhesive capsulitis, or osteoarthritis on the outcome of the SRT, so it is unknown if pathology to these structures may influence the outcome because of the pain response. Future investigation with a prospective study design will be useful to examine the influence of these variables on this examination maneuver.
Conclusion
The findings of this diagnostic study support the hypothesis that the SRT may accurately be used to assess the status of the rotator cuff. This quick, simple physical examination maneuver was found to be accurate, sensitive, and specific for diagnosing full-thickness RCTs. Additionally, these results indicate that the SRT is equally as accurate in predicting an intact rotator cuff tendon.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K. is a consultant for Tornier/Wright Medical, has received research support from Wright Medical, and is a paid speaker/presenter for Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Texas Southwestern Institutional Review Board (STU 092013-085).