
Abstract
Background:
Racquet sports have increased in popularity over the past decade. Although research is available regarding the epidemiological characteristics of tennis injuries, little is known about the frequency and characteristics of injuries in other racquet sports.
Hypothesis:
Given the increase in all racquet sport participation in the United States (US), it is hypothesized that injuries have accordingly become more frequent.
Study Design:
Descriptive epidemiology study.
Methods:
Using the National Electronic Injury Surveillance System database, we reviewed the numbers of badminton and squash/racquetball injuries presenting to a representative sample of US emergency departments (EDs). We used weighted estimates to extrapolate the data to the US population. Incidence estimates were compared with national participation data and stratified.
Results:
A total of 4330 injuries were reported, representing an estimated 173,000 injuries presenting to US EDs from 1997 through 2016. Despite the increase in the number of players from 2006 through 2016, the annual injury rate for squash/racquetball declined significantly, including the rates for each body region assessed. No similar trend was found for badminton injuries. Within our extrapolated ED cohort, the lower extremities were the most common body region injured (37%). Strains/sprains were the most common injury type in the trunk (73%), lower extremities (65%), and upper extremities (32%), whereas lacerations were most common in the head/neck (49%). In badminton, the youngest players (age range, 5-18 years) sustained twice as many fractures (relative risk [RR], 1.96; 95% CI, 1.14-3.38) and almost 3 times as many lacerations as patients in any other age group. Similarly, the youngest squash/racquetball players were at highest risk for lacerations (RR, 1.45; 95% CI, 1.22-1.73) and head and neck injuries (RR, 1.52; 95% CI, 1.26-1.83).
Conclusion:
Although declines in rates of squash/racquetball injuries were observed, the increasing popularity of badminton, squash, and racquetball necessitates further preventive measures to improve player safety, with an emphasis on the youngest players.
Racquet sports, comprising tennis, badminton, racquetball, and squash, have seen a significant surge in popularity during recent years, with an annual percentage growth that has outpaced more visible sports such as football, basketball, and ice hockey. 5 This trend has been attributed in part to the relative convenience and feasibility of these sports for individuals of all ages, combined with minimal financial barriers to entry. Modern adaptations of the traditional rules, such as reduction in badminton court sizes to accommodate younger players, have also given the general public increased accessibility to racquet sports. 5,25,29
The physical exertions called for in racquet sports involve a combination of repetitive maneuvers that can place major stresses on the upper and lower extremities. These forces increase the risk for acute and chronic injuries of varying severity. The sudden and frequent acceleration and deceleration maneuvers involved in racquet sports place a substantial eccentric load on the lower extremities, risking strains, sprains, and ligament injuries. 2 Meanwhile, the recurring motion of overhead serves and returns places repetitive rotational stress on the upper extremity, especially the shoulder.
Among racquet sports, tennis has the largest number of players and is responsible for most of the growth in racquet-sport participation and racquet-sport injuries. However, nontraditional racquet sports have also seen meaningful increases in recreational participation. Squash, in particular, is one of the 3 fastest growing activities in the United States (US), with participation increasing by approximately 66% from 2010 to 2015. 23,29 Participation in badminton also increased in the United States from 2006 to 2016, by about 1.4 million players aged 6 years and older, 24 and it has increased worldwide over the past few years, although the increases in badminton participation have not occurred to the same degree as the other racquet sports. 24
Despite these developments, biomedical research on racquet sports has focused almost exclusively on tennis, and comprehensive data regarding nontennis (“alternative”) racquet sports are almost nonexistent. 9,16 Many such studies were single-institution reviews or were based on small, nongeneralizable samples. Still, these studies have shown that badminton and squash players sustain a higher frequency of traumatic injuries and a lower frequency of overuse injuries compared with tennis players. Additionally, facial and ocular injuries have been observed at higher rates in racquetball than in other racquet sports, despite the use of protective eyewear. 17,18 The distribution of injuries in these alternative racquet sports thus warrants further inquiry.
To our knowledge, no study has assessed injuries in alternative racquet sports. Our aim was to investigate these injuries during a 20-year period using a nationally representative data set. Understanding the different injury patterns that exist between badminton and squash/racquetball, particularly as they compare with tennis, is an important step toward elucidating long-term trends and providing better, more targeted injury prevention.
Methods
This study was deemed exempt by our institutional review board. We reviewed the prospectively collected data from the National Electronic Injury Surveillance System (NEISS) database from 1997 through 2016. These data, maintained by the US Consumer Product Safety Commission, are collected from approximately 100 representative US hospitals. 26 Each emergency department (ED) visit is reviewed by a NEISS coder who records patient age, race, sex, injury type, affected body part, consumer products involved, disposition from the ED, setting where the injury occurred, and a brief description of the injury mechanism. Sampling is performed to create a probability sample that allows generalizability of NEISS data to the approximately 5400 US hospitals that have at least 6 beds. 27
All cases of alternative racquet-sport injuries were downloaded from the NEISS website. 28 Stable badminton data were available from only 2001 onward. These data included injuries associated with activity, equipment, or apparel. Cases were excluded if the injury did not occur secondary to the act of playing the sport or if they involved a spectator. Data on patients younger than 5 years were excluded because of the physical abilities required for appropriate play. Ultimately, there were 843 cases of badminton and 3487 cases of squash/racquetball that met inclusion criteria.
NEISS variables for age, injury, body part, disposition from the ED, and injury setting were categorized for analysis. For squash/racquetball, we created age categories on the basis of current age divisions used by the US Squash Organization: 5-18 years, 19-34 years, 35-49 years, and ≥50 years. 29 In the absence of established age brackets for badminton, the US Squash Organization’s age brackets were used for badminton as well.
We categorized diagnoses as either skin-level injuries (including lacerations and avulsions) or soft tissue injuries (including hematomas and contusions/abrasions). Concussions, dislocations, fractures, and strains/sprains were treated as separate categories. All remaining NEISS codes for injury type were grouped as “other.”
For body parts, NEISS categories were subdivided into head/neck (ear, face, head, mouth, or neck), lower extremity (upper legs to toes), trunk, and upper extremity (shoulders to fingers). Dispositions were classified as released from the ED, hospitalized (admitted, transferred, or held for observation), or left hospital against medical advice. Injury settings were regrouped as schools/public properties, sports/recreational centers, or other (including homes, farms, apartments/condominiums, or street/highway).
A sampling weight was assigned to each case on the basis of the inverse probability of each selection to provide a national estimate. Values with weighted historical estimates less than 1200, with fewer than 20 records, or with a coefficient of variation greater than 33% were considered unstable and excluded from our model. Data were rounded to 2 significant digits for ease of comprehension. However, all calculations were made using the raw values obtained from the statistical models. Data were analyzed by use of SPSS Complex Samples software, version 3.0 (IBM Corp); 95% CIs were calculated by using a direct variance estimation procedure that accounted for sampling weights. A linear regression model was used to evaluate trends in injuries per year and stratified by age group, body region, and injury type. The Outdoor Industry Association estimates of badminton, squash, and racquetball participation from 2006 through 2016 for individuals aged 6 years or older were used to calculate annual injury rates. 23,24 Statistical significance for all tests was defined as P < .05.
Results
Combined Alternative Racquet-Sport Injuries
During the 20 years studied (1997-2016), an estimated 173,000 individuals (95% CI, 110,000-220,000 individuals) with alternative racquet-sport injuries were treated at EDs in the United States. The mean age of injured patients was 33 years (SD, 17 years). Age distribution was bimodal, with peaks at 18 and 42 years. Male players comprised 74% of all alternative racquet-sport injuries, and 33% of all patients were aged 19 to 34 years. Only 2.3% of patients were admitted to the hospital for their injuries. Most injuries occurred at sports/recreational centers (76%), with the second most common injury setting being school/public property (17%).
Within our extrapolated cohort, the most common injury types across the sports were strains/sprains (36%), soft tissue injuries (16%), and skin-level wounds (16%). In the extremities and trunk, the most frequent injuries were strains/sprains (73% trunk, 65% lower extremity, and 32% upper extremity). For the head and neck, lacerations were the most common injury (49%).
Injury Trends
Although the total number of squash/racquetball players has increased during the past 2 decades, the annual number of injuries treated at US EDs decreased during the years examined, from an estimated 10,000 injuries in 1997 to 3100 injuries in 2016 (r 2 = 0.95) (Figure 1). This was a significant reduction of 70% (m = −346, P < .0001). According to US participation data from 2006 through 2016, the annual injury rate per 100,000 players also decreased (m = −7.58, P < .0001). When stratified by age group, the injury reductions were significant only for those in the 19- to 34-year (m = −36.3) and 35- to 49-year (m = −21.2) age groups (both P < .0001). Similar trends were seen in the rates of injuries for patients treated in the ED when stratified by body part across all regions (ie, head/neck, lower extremity, upper extremity, and trunk) for squash/racquetball. We found no significant trends in injury type. No significant trends were observed (m = 13.9, P = .43), whether overall or stratified, for badminton despite estimates of a 22% increase in participants from 2006 through 2016 (Figure 2).

Estimated number of squash/racquetball injuries in the US population (for players aged ≥5 years), 1997 through 2016.
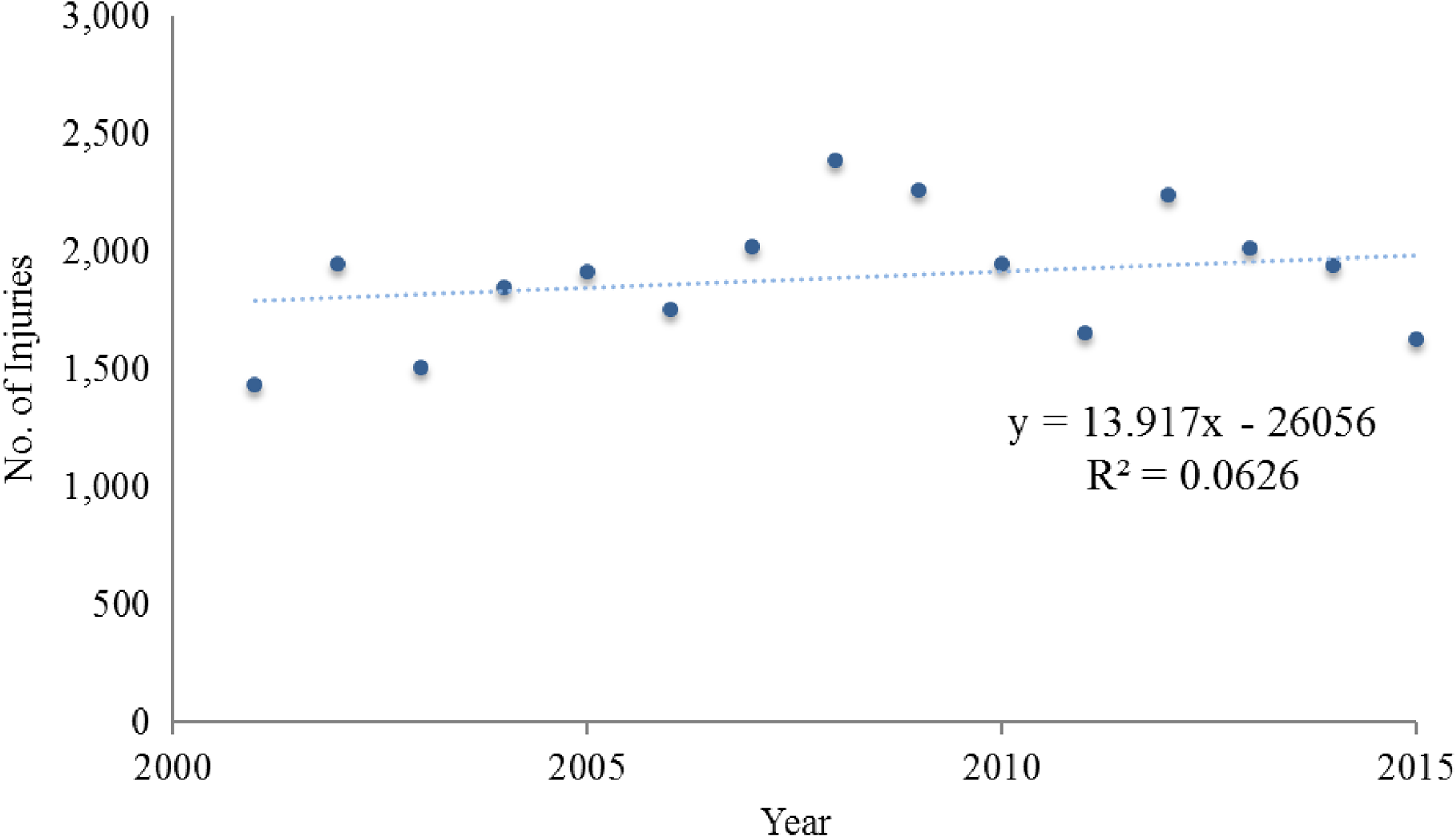
Estimated number of badminton injuries in the US population (for players aged ≥5 years), 2001 through 2016.
Badminton
Demographic Characteristics
In total, 33,000 patients (95% CI, 25,000-41,000) were treated in US EDs for badminton-related injuries as documented in the NEISS database from 2001 through 2016 (Table 1). Approximately 50% of patients were female. Players 5 to 18 years of age comprised the largest age group (58%). In contrast to squash/racquetball, most injuries (40%) occurred in schools/public properties.
Characteristics of Badminton Injuries Treated in US Emergency Departments Based on NEISS Sample, 2001-2016 a

a ED, emergency department, NEISS, National Electronic Injury Surveillance System.
b Estimates have been rounded to 2 significant digits. Percentages were calculated on the basis of the fraction of recorded injuries, using national estimates, in each subcategory out of the group total. Percentages may not sum to 100% because of rounding error.
Injury Type and Body Part Injured
Within our extrapolated cohort of badminton players evaluated in emergency care settings, strains/sprains were the most common type of injury sustained (45%), with soft tissue injuries (17%) and skin-level injuries and fractures (9% for each) accounting for the second and third most frequent types (Figure 3). Dislocations were the most common type of injury in the upper extremity (12%). For the head/neck, lacerations (37%) accounted for the largest proportion of the injuries. Strains/sprains were the most common injuries in the trunk (56%) and lower extremity (69%). Badminton players aged 5 to 18 years had a higher risk of fractures (relative risk [RR], 1.96; 95% CI, 1.14-3.38; P = .015) and lacerations (RR, 2.82; 95% CI, 1.70-4.68; P = .0001) than any other age group.

(A) Distribution of injuries sustained during badminton by body region. (B) Type of injuries sustained during badminton.
The lower extremities were the most commonly injured region (44%), of which the ankle was the most affected body part (42%). Upper extremity and facial injuries were nearly equal in frequency (24% and 21%, respectively). Female players had nearly twice the risk of upper extremity injuries as did male players (RR, 1.74; 95% CI, 1.33-2.26; P = .001).
Squash/Racquetball
Demographic Characteristics
From 1997 through 2016, an estimated 140,000 (95% CI, 95,000-180,000) patients were treated in US EDs for squash- or racquetball-related injuries (Table 2). In contrast to badminton, 80% of injured players were male. Players aged 19 to 34 years represented 37% of the patients. Ninety-seven percent of patients were treated and released from the ED; only 2.4% were admitted to the hospital. Most recorded injuries occurred at sports/recreational centers (85%), compared with 11% at schools/public properties.
Characteristics of Squash and Racquetball Injuries Treated in US Emergency Departments Based on NEISS Sample, 1997-2016 a

a ED, emergency department, NEISS, National Electronic Injury Surveillance System.
b Estimates have been rounded to 2 significant digits. Percentages were calculated on the basis of the fraction of recorded injuries, using national estimates, in each subcategory out of the group total. Percentages may not sum to 100% because of rounding error.
Injury Type and Body Part Injured
The most commonly injured body regions for squash/racquetball players treated in emergency care settings in the United States were the lower extremity (35%) and trunk (11%) (Figure 4). As in badminton, the ankles were the most frequently injured location in the lower extremity (39%), whereas the face (consisting of the eyelid, ocular region, and nose) accounted for 47% of injuries to the head/neck. Notably, the ocular region represented 26% of all head/neck injuries. Female players had a higher risk of upper extremity (RR, 1.22; 95% CI, 1.05-1.43; P = .01) and lower extremity (RR, 1.12; 95% CI, 1.00-1.24; P = .046) injuries than did male players, whereas male players had a higher risk of head/neck injuries (RR, 1.20; 95% CI, 1.06-1.37; P = .004), particularly to the face (RR, 1.51; 95% CI, 1.03-1.90; P = .004). The body parts at greatest risk in female players of squash/racquetball were the wrist (RR, 2.47; 95% CI, 1.73-3.52; P = .0001), arm (RR, 2.06; 95% CI, 1.20-3.56; P = .0091), and knee (RR, 1.50; 95% CI, 1.20-1.99; P = .0008). Players aged 5 to 18 years had nearly 1.6 times higher risk of head/neck injuries than all others, largely because of a significantly greater risk of facial injuries (ie, to the eyelid, ocular region, and nose) (RR, 1.52; 95% CI, 1.26-1.83; P < .0001).

(A) Distribution of injuries sustained during squash/racquetball by body region. (B) Type of injuries sustained during squash/racquetball.
Strains/sprains were the most common injury type for squash/racquetball players who presented to US EDs, accounting for 34% of injuries, followed by skin-level wounds at 17%. Strains/sprains were the most common injuries in the lower extremity (59%), upper extremity (32%), and trunk (14%). In squash/racquetball, similar to badminton, lacerations were the most common injury of the head/neck region (49%). Players aged 5 to 18 years had nearly 1.5 times higher risk of lacerations than players in other age groups (RR, 1.45; 95% CI, 1.22-1.73; P = .0001). No differences in risk were observed between male and female squash/racquetball players by injury type.
Discussion
The number of injuries associated with squash/racquetball treated in US emergency care facilities declined significantly in rate and in number from 1997 to 2016, despite much greater expansion of its US player base compared with badminton in the past decade. 29 We found that the greatest proportion of injuries occurred in the lower extremities and primarily consisted of strains and sprains. The vast majority of these injuries, irrespective of sport, occurred at sports/recreational centers, rather than at home, work, or other settings.
Several factors may explain the annual decline in injuries for squash/racquetball treated at US EDs. The increasing number of dedicated squash and racquetball clubs that cater to players of all skill levels is one likely explanation, because these facilities can advocate for safe play and encourage use of protective equipment. Additionally, the growth of the sports among younger players (whose reaction times are faster, on average, than those of older players 3,20 and who may therefore better tolerate the rapid nature of these games) may contribute to the reduced incidence of injuries. It is also plausible that newer players engage in a less dangerous, more leisurely level of play and thereby reduce risk of injury. However, this factor is difficult to quantify, and it would not explain fully the observed decline in injuries. Other explanations for the decreased incidence of injury could be reflective of limitations in this data set. The overall number of alternative racquet-sport injuries, especially minor types, is likely underestimated because only those evaluated in an ED setting were captured. Thus, this number would not include the minor overuse injuries treated at the increasingly available urgent care, primary care physician, or outpatient sports medicine office. In addition, this data set does not include players who sustained an injury from play but did not seek further treatment.
We did not observe a similar reduction in injury rates for badminton compared with squash/racquetball. One explanation is that the basic equipment for badminton has remained largely stagnant compared with squash/racquetball, where eye protection has become increasingly emphasized, including within statements from the US Squash Organization, 29 and thus posted at many dedicated playing facilities. Given the relatively stable number of participants in badminton over the past 10 years, compared with the rapid player increase observed in squash/racquetball, badminton clubs and organizations may not have the same level of awareness and urgency regarding injury protection.
Despite this reduction in incidence, certain player subgroups (by age and sex) stood out among our extrapolated ED cohort as being at higher risk for particular injuries. Squash/racquetball players aged 5 to 18 years were at higher risk for acute traumatic injuries, particularly lacerations and fractures, compared with all other age groups. This finding corroborates previous studies that have shown significantly greater proportions of acute traumatic injuries among squash players compared with players of other racquet sports. 2,22 This disparity may be explained in part by the smaller court used in squash, which, when combined with less experienced, younger players who may have less sound technique and a more reckless style of play, poses obvious increased risks. 11 However, given the overwhelming similarities between squash and racquetball, further inquiry is needed to elucidate the differences in style of play and injury risk between these 2 sports.
For those players treated in the ED setting, the youngest subgroup of players (ages 5-18 years) were at more than 1.5 times higher risk of head/neck injuries in badminton and squash/racquetball, primarily because of higher incidence of facial trauma. These sports pose risk of injury to the face and eyes because of the close proximity of players and the projectile nature of the ball or shuttlecock. Previous studies have evaluated the effectiveness of eye protection rules at reducing injury, citing increased exposure to instruction and knowledge of injury risk as proportional to the likelihood of players adopting such rules. 4,6,8 It thus follows that young players may be less likely to wear eye protection and to observe equipment rules. Regardless, ocular involvement was observed in more than 25% of patients with head and neck injuries. Although equipment compliance data were unavailable, research shows that less than 50% of squash players use adequate eye protection, a finding which suggests that further enforcement and disbursement of proper equipment are warranted, particularly for less experienced players. 20
We found that female players were 1.1 to 1.7 times more likely to sustain upper and lower extremity injuries compared with male players. Injury risk by player sex has been well studied in the tennis research. Bylak and Hutchinson 1 reported that female players more frequently experienced patellofemoral injuries, had lower upper extremity strength, and began competitive play with less conditioning than their male counterparts. In addition, Safran and Hutchinson (unpublished data, 1997), studying participants at the US Tennis Association National Hard Court Championships, showed in a 1-year sample that girls younger than 18 years had greater injury risk and higher prevalence of injuries (specifically of the lower extremity, wrist, or hand) than male players of the same age. Because the biomechanics of tennis are similar to those of other racquet sports, the explanation by Bylak and Hutchison 1 regarding the greater risk of shoulder, elbow, and knee injuries in female tennis players may apply to female badminton and squash/racquetball players as well.
Our finding that fractures were the fourth most common injury type evaluated and treated in US EDs, occurring at a rate of 9.7%, represents a potential weakness of our study. This figure is nearly twice the values cited in the research, which range from 1.5% to 4.9% for badminton, squash, and racquetball collectively. 14 Our larger estimate is likely attributable to the selection bias toward more severe injury types and mechanisms that is inherent in using an ED sample. Similarly, this data set may underestimate the incidence of nonemergent, chronic overuse, and stress-type injuries. The fact that so many players sought emergency medical care nonetheless underscores the need for protective equipment and safe play.
As expected, most injuries occurred at sports/recreational centers and schools/public properties. Approximately 37% of injuries, irrespective of sport, occurred in the lower extremity, which is consistent with other reported values ranging from 26% to 92%. 7,12,13,15 The overwhelming majority of lower extremity injuries we analyzed were strains or sprains, similar to other reports. 10,22 These findings represent an opportunity for targeted intervention, given the predictable settings in which these injuries occur. Sciascia and Cromwell 21 showed that preparticipation stretching does not reduce the risk of overuse injuries but does reduce the risk of muscle strain injuries. Therefore, we recommend training in muscular strength, endurance, and coordination because these sports require many jumps, lunges, and quick changes in direction with rapid arm movements from a variety of postural positions. 7 In particular, for the upper extremity, studies have shown benefits of a structured 3-phase rehabilitation program focused on core stabilization, kinetic chain integration, and functional strengthening. 14,19,21 Stretching of the major muscle groups (ie, the gluteals, hamstrings, hip flexors, and quadriceps) is important to improve the range of motion in the hips, knees, and ankles.
This data set is the only representative, stratified probability sample of injuries sustained by players of badminton, squash, and racquetball in the United States. The stability of these data is a strength of our study because it allows assessment of trends and can provide important information on sports-related injuries, as has been done previously in a variety of other sports. Limitations of our study are those inherent to a retrospective design and to the NEISS data set. Injuries treated at EDs are frequently the most severe, and only the most serious injury per individual is recorded in the NEISS data. Thus, our total incidence data are underestimated because NEISS does not capture non-ED settings, such as urgent care and primary care, or minor injuries that do not cause patients to seek care. Although most of patient encounters in this study likely represent unique individuals, it is possible that some patients may have presented multiple times for treatment of the same injury.
Conclusion
Although the overall number of injuries related to badminton and squash/racquetball that are treated at EDs in the United States has declined, the significant growth in participation in these sports warrants development and enforcement of protective rules, most importantly for the youngest players, who are at the highest risk of injury.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.L. has received educational support from Sofamor Danek and Arthrex and has received research support from Arthrex.
Ethical approval for this study was waived by the Johns Hopkins University.