
Abstract
Background:
Anterior glenohumeral instability is a common abnormality in the young, athletic population, especially in those participating in contact or collision sports.
Purpose:
To examine the effect of anterior labral tears, their associated injuries, and their management on future National Football League (NFL) performance.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of all NFL Combine participants from 2009 to 2015 was performed using medical and imaging reports compiled at the NFL Combine. These notes and images were reviewed and analyzed for involved structures, associated injuries, and evidence of previous surgical interventions. The respective NFL draft position, number of NFL games played, number of NFL games started, and NFL snap percentage for each player’s first 2 seasons were collected and compared with a control group and within subgroups.
Results:
Of the 2285 players at the NFL Combine between 2009 and 2015, there were 206 (9%) anterior labral tears confirmed by magnetic resonance imaging, 20 of which were bilateral, for a total of 226 affected shoulders. There were 908 players who fit the criteria for inclusion in the control group. Overall, there were no significant differences between players with anterior labral tears and the control players in terms of draft position (P = .259), games played in their first 2 NFL seasons (P = .391), games started in their first 2 NFL seasons (P = .486), or snap percentage in their first (P = .268) and second (P = .757) NFL seasons. In general, sustaining a concomitant injury with an anterior labral tear (superior labrum from anterior to posterior [SLAP] tear, glenoid bone loss, Hill-Sachs lesion, rotator cuff tear, humeral avulsion of the glenohumeral ligament, and anterior tear combined with posterior tear) negatively affected a player’s NFL draft position when compared with those with an isolated anterior labral tear (P = .003). There was no significant difference between operative and nonoperative management for anterior labral tears in terms of any performance metric.
Conclusion:
A history of anterior labral tears was not significantly associated with future NFL performance. While players with isolated injuries were drafted significantly earlier than those with concomitant injuries, combined injuries did not affect players’ games played, games started, or snap percentage in their first 2 NFL seasons. Glenoid bone loss did significantly decrease draft position; however, the severity of bone loss did not affect draft position, and there were no significant associations between glenoid bone loss and games played, games started, or snap percentage.
Anterior glenohumeral instability is a common abnormality in the young, athletic population, especially in those participating in contact or collision sports. 13,15 Typically caused by an initial traumatic event, shoulder instability is described as disruption of the inert (glenohumeral ligaments, glenoid labrum, etc) and dynamic (rotator cuff muscles, rotator cuff interval, etc) stabilizers of the glenohumeral joint, which leads to dislocations, subluxations, or apprehension. 13 Anterior disruption of the labrum, also known as a Bankart lesion, has been reported in up to 96% of patients with anterior instability, making it the most common pathoanatomic feature of this condition. 3 Variant lesions of the glenoid labrum include anterior labroligamentous periosteal sleeve avulsions, humeral avulsions of the glenohumeral ligament (HAGLs), and superior labrum from anterior to posterior (SLAP) tears. 13,26 These lesions, along with other associated injuries such as rotator cuff tears and bony defects, can contribute to the severity and outcomes of anterior shoulder instability. ∥
Recurrent instability is a common sequela of anterior instability, especially in high-risk patients. It has been shown that 38% of all patients who experience a primary dislocation will suffer a recurrence. 32 Factors that increase a patient’s risk for redislocations include young age at the initial episode, male sex, contact sport participation, and associated bony defects. 13,31 Treatment decisions of these injuries also affect the risk of redislocations, as surgical and nonsurgical management have produced differing results in patients with a first-time dislocation. Nonoperative management has produced recurrent instability rates ranging from 21% to 67%, with even higher rates seen in young patients, male patients, and athletes. 20,21,31,34,35,41 In contrast, surgical management of anterior instability has produced recurrence rates from 3% to 31%, even in young athletes participating in collision sports. ¶
These injuries are common occurrences in collegiate and professional football. The shoulder was reported to be the second most common injury site in a study of over 60,000 National Collegiate Athletic Association (NCAA) football players, 4 and another study reported that NCAA football players had the highest rate of shoulder instability episodes among collegiate athletes. 28 Previous studies have shown a detrimental effect from anterior shoulder instability on a player’s National Football League (NFL) career, 6 –8 especially in offensive and defensive linemen. 4,8 However, no study has specifically analyzed the effect of magnetic resonance imaging (MRI)–confirmed labral and associated injuries.
The purpose of this study was to examine the effect that anterior labral tears, their associated injuries, and their management had on future NFL performance, with a secondary goal of stratifying this analysis by position group. Our hypothesis was that these injuries would affect NFL performance and that linemen would be more significantly affected than non-linemen.
Methods
Study Design
A retrospective review of all NFL Combine participants from 2009 to 2015 was performed after approval from an institutional review board. Medical records and MRI scans were reviewed to identify all players with anterior tears of the glenohumeral labrum. MRI scans in the coronal, sagittal, and axial planes performed at the NFL Combine were then independently reviewed by 2 sports fellowship–trained orthopaedic surgeons (S.J.F., S.M.). An MRI was performed in players with prior labral surgery, a history of shoulder instability in the NCAA database, or physical examination findings suggesting anterior or posterior instability. It is presumed that these players were symptomatic or had been symptomatic in their collegiate playing career.
All injury data were collected through a review of the injury registry available to the medical and athletic training staff of all NFL teams after completion of the NFL Combine. The medical records and MRI scans were compiled at the NFL Combine, where the medical staff of each of the 32 NFL teams performed a musculoskeletal evaluation and recorded a comprehensive orthopaedic note for each player attending the combine. These notes and images were reviewed and analyzed for involved structures, associated injuries, and evidence of previous surgical interventions.
Labrum Evaluation
In this study, a glenoid labral tear was diagnosed by discontinuity of the normal labral tissue, separation from the glenoid rim, or intrasubstance splits in the labral tissue. A diagnosis was made and supported high-quality 3-T MRI scans, which have been proven to provide good utility in diagnosing these injuries. 1 For each affected shoulder, the size and location of the tear were documented. Labral tears were classified in terms of the location as anterior, posterior, or combined anterior and posterior. Any associated injuries were also documented, including SLAP tears, glenoid bone loss, Hill-Sachs lesions, rotator cuff tears, HAGLs, and those tears that were combined with posterior tears. Glenoid bone loss was separated into minor (<15%) or severe (≥15%) bone loss. Additionally, any evidence of previous surgical interventions seen on shoulder MRI was noted.
Performance Evaluation
Player position and number of missed collegiate football games were obtained from the medical database organized during the NFL Combine. Each player’s respective NFL draft position, number of NFL games played, number of NFL games started, and NFL snap percentage for the first 2 seasons in the NFL were collected through the use of NFL.com and Pro Football Focus, which are web-based, publicly accessible comprehensive sports statistics databases. Snap percentage was defined as the total number of plays in which an athlete participated divided by the total number of eligible plays over the course of a season.
A control group was formed to evaluate whether players without anterior labral injuries were drafted in earlier draft rounds and had superior performance during the first 2 years of play compared with players with labral injuries. The control group was composed of players who participated in the NFL Combine from 2009 to 2015 based on the following set of criteria: (1) no significant missed time before the NFL (≤2 total missed games in college) and (2) no history of any surgery before the NFL Combine.
Statistical Analysis
The performance metrics detailed above were compared between groups. Data were tested for normal distribution using the Shapiro-Wilk test. For comparisons of normally distributed continuous variables between groups, an independent t test was utilized. For comparisons of nonnormally distributed continuous variables between groups, the Mann-Whitney rank-sum U test was utilized. Comparisons of 2 categorical data were performed by use of the chi-square and Fisher exact tests. All P values were 2-tailed, and P values of <.05 were considered statistically significant. All statistical analyses were performed by the use of R (The R Project for Statistical Computing).
Results
Demographics
Of the 2285 players at the NFL Combine between 2009 and 2015, 581 underwent MRI of their shoulder. There were 206 (9%) anterior labral tears confirmed by MRI, 20 of which were bilateral, for a total of 226 affected shoulders. There were 908 players who fit the criteria for inclusion in the control group. Of the 206 affected players, 148 (72%) showed imaging evidence of a surgical intervention, while 58 (38%) were managed nonoperatively. There were 192 (93%) players with an associated injury, with the most common being a Hill-Sachs lesion (n = 138, 67%) and a combined posterior labral tear (n = 103, 50%). Demographic data are detailed in Table 1.
Demographics of Players a

a Values are reported as n.
Performance Evaluation
Overall, players with anterior labral tears did not perform significantly worse in the NFL than the control group in terms of draft position (P = .259), games played in their first 2 NFL seasons (P = .391), games started in their first 2 NFL seasons (P = .486), or snap percentage in their first (P = .268) and second (P = .757) NFL seasons. Positional analyses did not show significant associations in any performance measure, although offensive linemen typically demonstrated the lowest P values of any position. Injured linemen, both offensive and defensive, were not significantly affected in any performance measure when compared with the control group. Overall performance evaluation findings are outlined in Table 2.
Overall Performance Evaluation Results a

a Values are reported as injured mean/control mean (P value). N/A, not applicable.
Associated Injuries
In general, sustaining a concomitant injury with an anterior labral tear negatively affected a player’s NFL draft position when compared with those with an isolated anterior labral tear. For all players in this study who sustained associated injuries that were recorded, they were drafted later than those players with isolated anterior labral injuries (95.8 vs 170.1, respectively; P = .003). This significant difference held true for each specific concomitant injury, with the exception of HAGLs (P = .229). There were no significant differences between combined and isolated injuries in terms of games played, games started, or snap percentage in the first 2 NFL seasons. The effects of associated injuries are delineated in Table 3.
Effects of Associated Injuries a
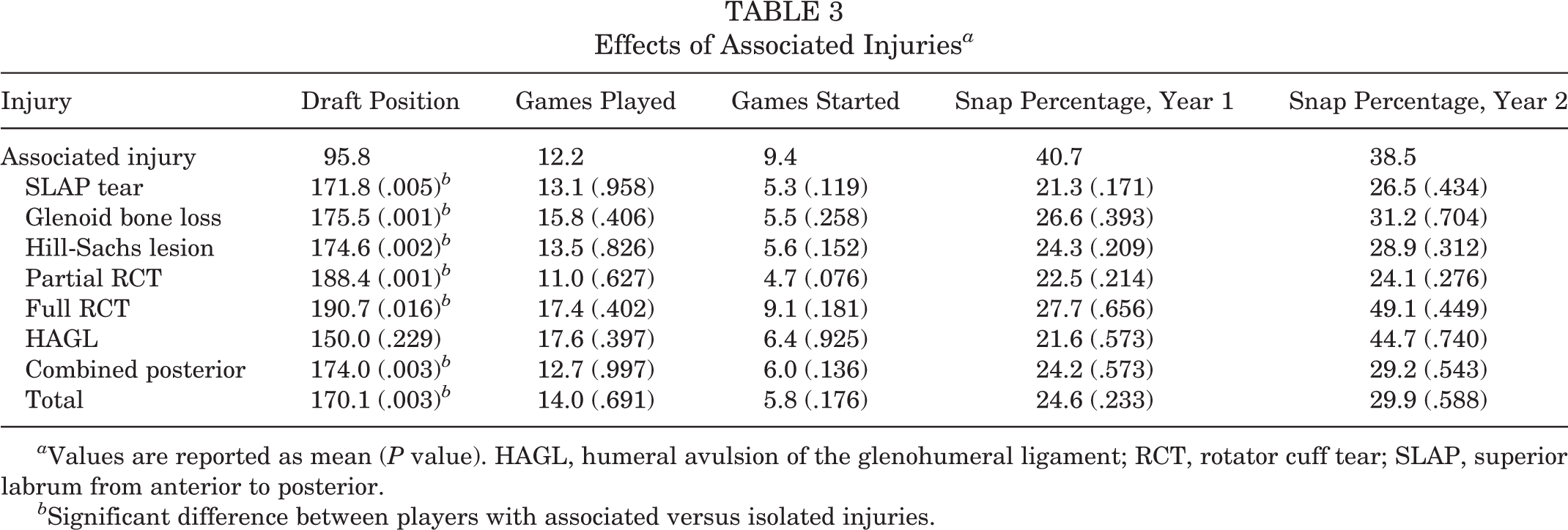
a Values are reported as mean (P value). HAGL, humeral avulsion of the glenohumeral ligament; RCT, rotator cuff tear; SLAP, superior labrum from anterior to posterior.
b Significant difference between players with associated versus isolated injuries.
Glenoid bone loss affected a player’s draft position when combined with anterior labral tears compared with isolated labral tears (95.8 vs 175.5, respectively; P = .001). This was true for both severity levels of bone loss: minor bone loss (<15%) and severe bone loss (≥15%). Associated glenoid bone loss did not demonstrate significant differences from isolated anterior labral tears in terms of games played, games started, or snap percentage in the first 2 NFL seasons. The severity of bone loss showed significant differences only in games played and games started; these data are detailed in Table 4.
NFL Performance Based on Severity of Anterior Glenoid Bone Loss a

a Values are reported as mean (P value vs no glenoid bone loss). NFL, National Football League.
Operative Versus Nonoperative Management
There were no significant differences between operative and nonoperative management for players with anterior labral tears in terms of any performance metric. No position demonstrated any significant difference based on the treatment. A comparison of operative versus nonoperative treatment is displayed in Table 5.
Operative Versus Nonoperative Management a

a Values are reported as mean unless otherwise stated.
Discussion
The most important finding of this study was that although anterior labral tears do not appear to independently affect NFL performance, they do have a significant detrimental effect on NFL draft position when associated with several different concomitant shoulder injuries. This negative effect was seen when combined with SLAP tears, glenoid bone loss, Hill-Sachs lesions, rotator cuff tears, and combined anterior and posterior labral tears. HAGLs did not demonstrate a significant association with draft position. These same detrimental effects were not seen in games played, games started, or snap percentage, perhaps suggesting that these players are overpenalized by teams in the draft.
Secondarily, this study found that although glenoid bone loss demonstrated a significantly detrimental effect on draft position, it did not affect any other NFL performance metrics, and the severity of bone loss did not show an overwhelmingly significant effect on any performance metric. This is an important finding because bony defects are often associated with anterior instability, and the progression of bone loss typically leads to worsening of the condition. 10,18
Brophy and colleagues 6,7 found that a history of anterior shoulder instability significantly decreased the likelihood of playing in the NFL for linemen. Our study did not find that MRI-confirmed anterior labral tears necessarily decreased the number of games played or started in a player’s first 2 NFL seasons after the combine for any specific position or for linemen as a group. In another study, Brophy and Marx 9 also reported an increased recurrence rate and decreased time to recurrence in players with anterior shoulder instability treated nonoperatively. However, their cohort did not demonstrate any significant differences between surgical and conservative management in terms of the performance metrics analyzed (draft position, games played, games started, and snap percentage).
There were some limitations to this study, beginning with the retrospective nature of the compiled patient data. Because not every player underwent shoulder MRI at the NFL Combine, there is a potential that players with anterior labral tears were not included in our study, especially those without significantly debilitating symptoms. Further, we were unable to perform magnetic resonance angiography or 3-dimensional computed tomography consistently in this study; these measures have been reported to provide greater sensitivity in detecting certain labral abnormalities and glenoid bone loss, respectively. This study did not correlate physical examination findings to imaging findings, limiting the clinical applications. There are several potential confounding variables that could have affected draft position and NFL performance, including collegiate performance, combine performance, interview results, off-field issues, and NFL team needs. There is a potential bias for better performance in these injured players, given the additional motivation from salary and future socioeconomic status. In certain instances, our analyses by position were limited by the sample size. Some studies on NFL performance outcomes have employed a longer follow-up duration 6,7,14 ; however, certain players in our cohort only had 2-year data available, which may limit the conclusions that can be drawn from our results. Despite its limitations, there are significant findings from this study that may help guide diagnosis and treatment decisions in elite collegiate football players with shoulder injuries.
Conclusion
A history of anterior labral tears was not significantly associated with future NFL performance. While players with isolated injuries were drafted significantly earlier than those with concomitant injuries, combined injuries did not affect players’ games played, games started, or snap percentage in their first 2 NFL seasons. Glenoid bone loss did significantly decrease draft position; however, the severity of bone loss did not affect draft position, and there were no significant associations between glenoid bone loss and games played, games started, or snap percentage.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.F. receives research support from DJO. S.M. receives research support from DJO and Smith & Nephew. M.D.P. is a consultant for Arthrex, DePuy, and Arthrosurface. R.F.L. receives royalties from Arthrex, Ossur, and Smith & Nephew; is a consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew. M.T.P. receives royalties from Arthrex and SLACK and is a consultant for Arthrex and the Joint Restoration Foundation (AlloSource).
Ethical approval for this study was obtained from Partners HealthCare.