
Abstract
Background:
Traumatic anterior dislocations of the sternoclavicular joint (SCJ) are rare. Although they can usually be treated by a closed reduction, the reported subsequent recurrence rate is 50%.
Purpose:
To determine whether further instability after first-time traumatic anterior dislocation would be prevented by a minimally invasive open repair of the anterior SCJ capsule, augmented with internal bracing.
Study Design:
Case series; Level of evidence, 4.
Methods:
Open repair of the anterior SCJ capsule was completed on a series of patients who had sustained a first-time traumatic anterior dislocation of the SCJ. Patients with preexisting SCJ instability and recurrent dislocations were excluded. Through a transverse incision, the anterior SCJ capsule was repaired and plicated by use of sutures. The repair was then protected by use of an internal brace, bridging between the sternum and the medial end of the clavicle.
Results:
Six patients (4 males, 2 females) with a mean age of 28.3 years were included. Four patients underwent surgery within 4 weeks of their dislocation, and 2 patients had ongoing symptoms of instability but had not had a further dislocation. The median follow-up was 28.2 months (range, 24-35 months). At the most recent follow-up, none of the patients had sustained further dislocation or episode of instability, and their SCJs appeared stable. The mean abbreviated Disabilities of the Arm, Shoulder and Hand (QuickDASH) score was 2.3 (range, 0-4.5).
Conclusion:
The medium-term results of this case series suggest that after first-time dislocation, surgical repair of the anterior SCJ capsule augmented with internal bracing can prevent recurrent instability. This may be an attractive option for individuals involved in higher risk activities, as the operative management of recurrent anterior SCJ instability usually requires a figure-of-8 tendon reconstruction, which carries a significantly higher morbidity.
First-time traumatic anterior dislocation of the sternoclavicular joint (SCJ) is usually treated by closed reduction, if required, and then rehabilitation. 12 However, the redislocation rate after anterior dislocation has been reported to be higher than 50%. 22 In addition, a number of patients who do not formally redislocate eventually develop symptomatic instability or subluxation. 6,24
The management of a patient with symptomatic, recurrent anterior instability of the SCJ usually requires surgical reconstruction. 19 Several procedures have been described; a figure-of-8 reconstruction, involving either a tendon autograft or allograft or a synthetic ligament, is the most biomechanically reliable. 4,9,15,20 This type of procedure involves obtaining adequate exposure of both the sternum and the medial end of the clavicle to make the drill holes. This can potentially put the posterior mediastinal structures at risk.
We have developed a technique to directly repair the anterior SCJ capsule, protecting the repair with an internal brace, following a first-time anterior dislocation. This procedure does not require any formal exposure of the sternum or medial end of the clavicle and does not put the posterior mediastinal structures at risk.
In this retrospective case series of prospectively collected data, we describe the technique and report our early results of direct repair of the SCJ anterior capsule, augmented with internal bracing, following a first-time, traumatic anterior dislocation.
Methods
This study was registered with our hospital audit office. Beginning January 2014, patients referred to our unit who had a persistent, acute, first-time anterior dislocation of the SCJ or had had a first-time anterior dislocation of their SCJ within the preceding month, and were younger than 30 years, were offered a surgical repair of the anterior SCJ capsule augmented with internal bracing. Additionally, patients who had had a first-time, traumatic anterior dislocation more than 4 weeks prior to presentation and had continued symptoms of instability were offered a surgical repair.
We searched the senior author’s (G.T-S.) surgical database for patients who had undergone a surgical repair of the SCJ anterior capsule augmented with internal bracing following a single, traumatic anterior dislocation, between January 2014 and December 2015. Inclusion criteria were a single, traumatic anterior dislocation with either radiographic evidence of the joint dislocation or a magnetic resonance imaging (MRI) scan demonstrating disruption of the joint capsule. Exclusion criteria included patients who had had recurrent anterior SCJ dislocations and those who had a preceding history of SCJ instability.
From the patients’ medical records, we obtained details of the mechanism of injury, history, initial management, symptoms, examination findings, and imaging. All of the patients had undergone a preoperative MRI scan in the axial and coronal planes, at our hospital, to assess the extent of the soft tissue and bony damage (Figure 1). The stability, range of motion compared with the uninjured side, and function of the SCJ were assessed at the patients’ most recent clinical follow-up by the senior author and a specialist shoulder physical therapist.
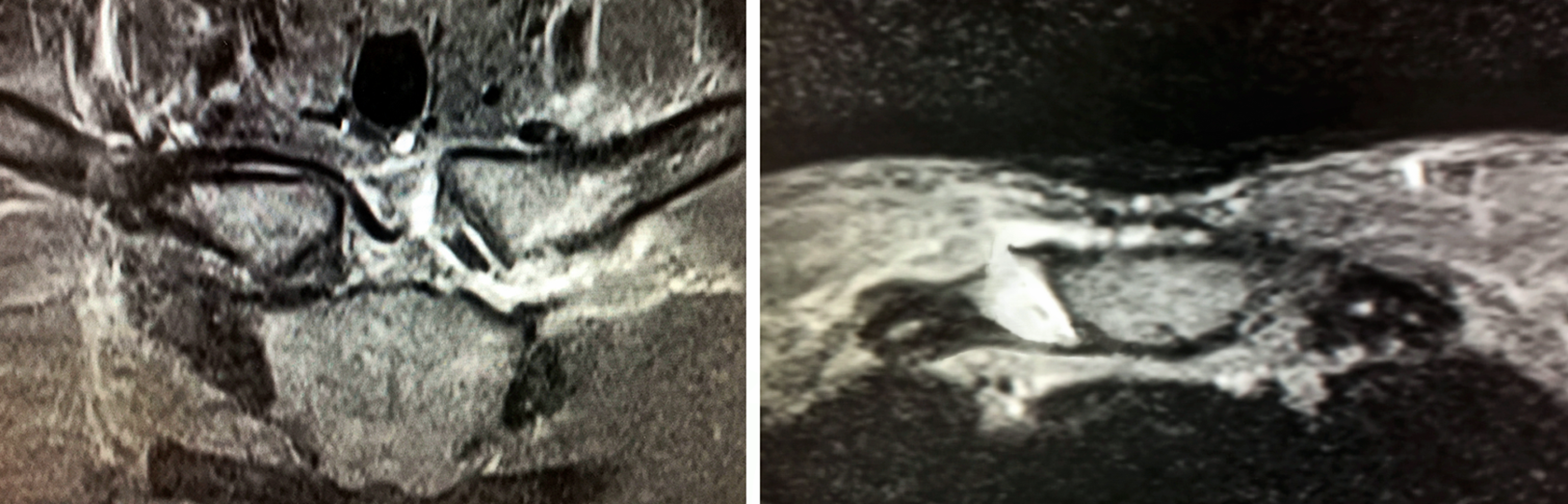
T2-weighted coronal and axial magnetic resonance imaging scans of the sternoclavicular joints 48 hours after a left traumatic anterior dislocation that has been reduced. There is a significant effusion with a tear to the left interclavicular ligament and to the anterior capsule.
The primary outcome was recurrence of instability (redislocation or subluxation). 23 Secondary outcomes were the abbreviated Disabilities of the Arm, Shoulder and Hand (QuickDASH) score 10 and range of motion. 23
All procedures were undertaken by the senior author after obtaining informed consent for all patients. This included the possibility of proceeding to a more extensive surgical dissection and a formal SCJ reconstruction using an autograft hamstring figure-of-8 technique, if achievement of a satisfactory repair of the anterior capsule was believed not possible. However, a more extensive procedure was not required for any of the patients.
Surgical Technique
At our institution, the patient is positioned supine, and the sternum and clavicles are square draped. If the medial end of the clavicle is dislocated or subluxated, an attempt at closed reduction is made. A 5-cm transverse incision is made over the medial end of the clavicle over the SCJ to the sternum. This stops short of the midline to allow for a potential curved, hockey-stick extension inferiorly, if additional exposure of the sternum is required. The platysma is divided, and the medial end of the clavicle, damaged anterior SCJ ligament, and medial edge of the sternum are exposed.
The damaged anterior SCJ ligament is then inspected. In some cases, an obvious rent in the capsule is seen, and the intra-articular disk and joint can be visualized. In other cases, the ligament has clearly been stretched out but is still in continuity. A longitudinal incision, in the line of the ligament fibers, is then made along the length of the ligament. The articular surfaces and the disk are then inspected.
A No. 5 braided nonabsorbable suture (FiberWire; Arthrex) is then passed through 1 side of the split ligament, medial to the sternal edge of the joint, and taken across diagonally and passed through the other side of the ligament, lateral to the clavicular side of the joint. This is repeated again, so that 2 passes are made of the suture diagonally. This process is repeated with another suture for the opposite edges of the ligament (Figure 2). These sutures are then tensioned and tied with their knot stacks lying on either side of the joint. This process tightens the anterior SCJ ligament in both the medial-to-lateral and superior-to-anterior directions. Further No. 5 sutures are passed and tied to repair the medial and lateral ends of the ligament (Figure 3).

Intraoperative photograph and diagram of an open repair of the anterior sternoclavicular joint capsule. The capsule has been opened longitudinally, and two No. 5 sutures (A-A, B-B) have been passed through the edges of the capsule and doubled over.

Intraoperative photograph and diagram of an open repair of the anterior sternoclavicular joint capsule. The 2 central sutures have been tied, and further sutures have been tied at either end of the capsular split.
The repair is then protected by use of an internal brace (InternalBrace; Arthrex).
Internal Bracing
Internal bracing is a ligament repair bridging concept that uses braided, ultrahigh-molecular-weight, polyester suture tape and knotless bone anchors to reinforce ligament strength as a secondary stabilizer after repair. Internal bracing is used to protect a soft tissue ligamentous or tendinous repair, eliminating the need for a postoperative external brace or immobilizer.
For an SCJ anterior capsular repair, the internal bracing system involved a 4.5-mm anchor (BioComposite SwiveLock; Arthrex), with a loaded suture tape (FiberTape; Arthrex), being inserted into the bone on the clavicular side of the joint. The 2 strands of the suture tape were passed over the repair, tensioned, and secured to the sternum on the other side of the joint with a 3.5-mm anchor (BioComposite SwiveLock). This provided a strong, static brace across the joint (Figure 4).

A diagram and a postoperative axial computed tomography scan of the left sternoclavicular joint. The 3.5-mm SwiveLock anchor has been inserted at an angle into the sternum, and the 4.5-mm SwiveLock has been inserted perpendicularly into the medial end of the clavicle with the FiberTape secured between them.
A 4.5-mm SwiveLock is 19.1 mm in length, and a 3.5-mm SwiveLock is 15.8 mm in length. We undertook preoperative measurements of the anterior-to-posterior width of the middle slice of the clavicle 1 cm from the medial end and the superior part of the sternum 1 cm medial to the sternal articular surface. The width of the medial end of the clavicle was 20 mm or more in all 6 patients. The width of the sternum was usually 15 mm.
At the time of surgery, we used a 2.5-mm pilot drill bit, which is supplied with the kit, to predrill holes in the medial end of the clavicle and the sternum, before using the presupplied taps. On the clavicular side, we measured and marked off the drill bit at 20 mm. We then carefully drilled through the midpoint of the medial end of the clavicle, 1 cm from its end, while lightly tapping the drill, so as to detect the far cortex. In all cases, the drill had penetrated to 20 mm before the far cortex was encountered. On the sternal side, we marked off the drill bit at 16 mm. Because we knew that the width of the sternum was only 15 mm, we angled the drill laterally, at about 30° to the vertical, to gain additional length to the drill trajectory and an element of a “deadman” angle fixation effect. 5 We carefully advanced the drill bit, while lightly tapping, to detect the far cortex. In all cases, again, the drill had penetrated 16 mm before the cortex was encountered (Figure 5).

Intraoperative photograph and diagram of an open repair of the anterior sternoclavicular joint capsule. The anchors for the InternalBrace have been inserted into the sternum and medial end of the clavicle with the 2 strands of FiberTape tensioned between them.
Had we felt the far cortex of either the clavicle or the sternum while we were drilling before the drill had penetrated sufficiently, we would have stopped drilling. As the anchors are made of a biocomposite material, we would have been prepared to insert them to the depth that we had obtained, accepting that they may protrude a couple of millimeters but knowing that they would resorb over time. Had we had any true concerns during the procedure that the far cortex of either bone was likely to be penetrated, we would have had a low threshold to slightly lengthen our incision and to dissect over the top of the clavicle and sternum to visualize and protect their posterior surfaces. We had obtained consent from all of the patients for the possibility of undertaking a hamstring tendon reconstruction that would have required a more extensive exposure than the intended procedure.
Having used the appropriate taps and tapped the clavicle and sternal drill holes, we inserted the 4.5-mm anchor with a loaded FiberTape into the clavicle. The 2 ends of the FiberTape were then loaded into the eyelet of the 3.5-mm anchor. The eyelet of this anchor was inserted into the bottom of the sternal drill hole, and the suture was tensioned to the point where the anchor could still be screwed down into the hole. Too much tension on the sutures would pull the eyelet out of the socket and not allow the anchor to be screwed into place.
Postoperative Regimen
Postoperatively, a computed tomography (CT) scan was undertaken to assess the reduction and the position of the anchors (Figure 6). The arm was kept in an immobilizer for 3 weeks to protect against excessive retraction. Following this, a standard rehabilitation program was begun.
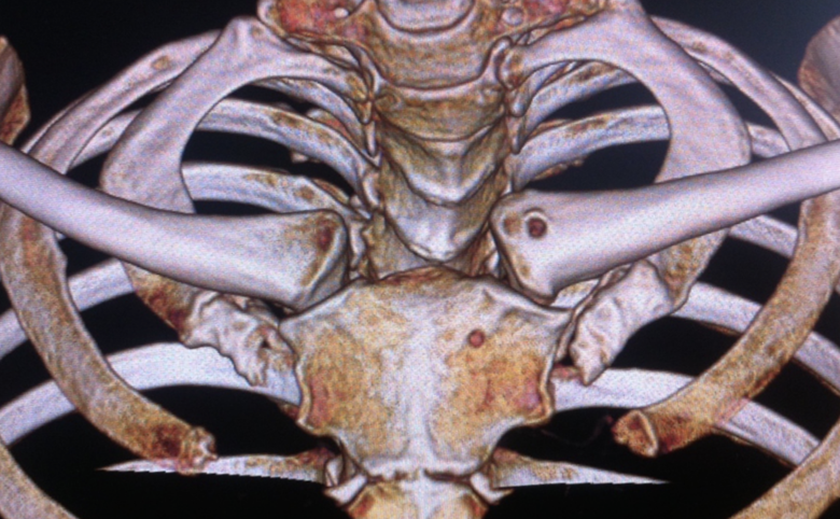
Postoperative 3D computed tomography reconstruction of the anterior chest wall demonstrating the reduced left sternoclavicular joint with the anchor entry holes visible.
Results
Six patients (4 males and 2 females) with an average age of 28.3 years met the criteria for inclusion. The median follow-up was 28.2 months (range, 24-35 months). The right side was involved in 4 patients. The first patient in the series presented acutely, with the SCJ still dislocated anteriorly. This was reduced by closed reduction at the beginning of the capsular repair procedure. Three other patients presented acutely following anterior dislocation, but these had been reduced. The remaining 2 patients had sustained an acute, anterior SCJ dislocation that had been reduced; they continued to experience symptoms of significant anterior instability but had not experienced redislocation. All of the patients played contact sports or martial arts. The mechanism of injury, ability to reduce the dislocation, and time from dislocation to surgery are summarized in Table 1.
Preoperative Demographics a

a F, female; L, left; M, male; NA, not applicable; R, right.
At the most recent follow-up, none of the patients had experienced a further dislocation of their SCJ, and they all considered their joints to be stable. They had all returned to either contact sports or martial arts within 1 year of their surgery. On clinical examination, all of the patients’ SCJs appeared stable. We noted no side-to-side difference with regard to instability or range of motion (protraction, retraction, elevation, internal and external rotation) between the operated and uninjured SCJs for any of the patients. The mean QuickDASH score was 2.3 (range, 0-4.5).
No complications occurred after any of the procedures.
Discussion
The SCJ is the only articulation joining the upper limb to the skeleton. It is the least constrained joint in the body, and its stability is heavily dependent on its ligaments and surrounding envelope of soft tissue structures. 3 Because of its central location, dislocation of the SCJ is relatively uncommon, representing less than 3% of dislocations. When it occurs, it is usually the result of high-energy indirect trauma. 19
The management of a first-time, traumatic anterior dislocation of the SCJ is generally nonoperative. In cases where the joint has spontaneously relocated, initial immobilization followed by a rehabilitation program is usually undertaken. When the joint remains dislocated, some authors have advocated an attempted closed reduction within 48 hours of the injury. If the joint is irreducible or has been dislocated for more than 48 hours, the dislocation is accepted. A combination of physical therapy, remodeling, and activity modification usually provides an acceptable result. 19
The literature provides very little information regarding open reduction and stabilization of an acute, first-time SCJ dislocation. In a study of 8 patients with a mixture of anterior and posterior SCJ dislocations, 2 patients had experienced a single, traumatic, anterior SCJ dislocation. 1 The surgeon in that study used a capsular repair technique with 2 suture anchors in the medial end of the clavicle; the sutures were passed through sternal bone tunnels and then tied back on themselves. None of the joints had redislocated at an average of 18 months after surgery; however, no mention was made of instability or subluxation. In a series of 4 pediatric patients, 2 patients had irreducible anterior dislocations that required an open reduction and were then stabilized via a figure-of-8 suture passed through clavicular and sternal bone tunnels. 7 Both patients were stable at 2 years after surgery.
The natural history after a first-time traumatic dislocation of the SCJ is not extensively documented and so not fully understood. Only a few studies are found in the literature, and they have low numbers of participants and are generally of poor methodology. However, a redislocation rate higher than 50% has been reported. 22 In another series, 78% of patients experienced either further full dislocation, a subluxation, or functional instability of the SCJ after a first-time, traumatic anterior dislocation. 6
The management of symptomatic, anterior, recurrent instability of the SCJ usually entails some form of reconstruction procedure. 13 A number of reconstruction techniques have been described. These all generally involve an open capsulotomy, resection of part of the medial end of the clavicle, and reconstruction of the capsule using either local soft tissues or a tendon graft. A biomechanical study comparing various soft tissue and graft reconstructions found that a figure-of-8 tendon graft was superior. 21 A figure-of-8 graft reconstruction is the current preferred technique used by most surgeons to reconstruct the SCJ. Numerous techniques have been described that use autograft and allograft palmaris longus and hamstring tendons and synthetic ligaments, with good results. 2,9,15,20
To our knowledge, no previous study in the literature has specifically examined a group of patients undergoing an augmented capsular repair for a first-time, traumatic anterior SCJ dislocation. The rationale for undertaking the described procedure was threefold. First, given our current knowledge of the natural history following SCJ dislocation, we considered it highly likely that the patients in this series, who wanted to return to contact sports, would go on to develop recurrent instability. Second, the senior author has observed that when undertaking an open reduction and stabilization for an acute posterior SCJ dislocation, the damaged capsular tissue is generally present. This is not the case when stabilizing a recurrent anterior or posterior SCJ dislocation where the capsular tissue is absent or of poor quality and a ligament reconstruction procedure is required. A soft tissue augmented repair to the anterior SCJ ligament requires only a relatively small incision with a limited dissection to expose the anterior surface of the medial end of the clavicle and the sternum. This stands in contrast to a ligamentous reconstruction, which requires a more extensive exposure of the sternum and mobilization of the medial end of the clavicle with potential damage to the posterior mediastinal structures. Third, internal bracing has been used successfully to augment various types of ligament repairs around the ankle, knee, and acromioclavicular joint. 8,11,14,25 Internal bracing acts as a secondary stabilizer to reinforce the repair, allowing for a quicker return to sport and potentially helping to resist injury and prevent recurrence. The additional advantage of using BioComposite anchors is that over time, they will be completely replaced by the surrounding bone.
The use of internal bracing has previously been described only as a protective augmentation after a ligament repair for a chronic soft tissue injury. 8,11,14,25 In this study, although protecting the acute, anterior SCJ ligamentous tear with internal bracing alone, and not repairing the tear, may have allowed it to heal, we did not consider this an option. The surgical exposure required to insert an internal brace involves opening up the medial and lateral ends of the capsular ligament, and we believed it would be inappropriate to not undertake a repair or plication of any associated capsular damage at the same time.
Taking the above factors into account, we believed that for the patients in this series, who had sustained a single traumatic incident and intended to return to contact sports, it would be in their interest to undergo an augmented anterior capsular repair of their SCJ.
This treatment rationale is similar to that used for younger patients who have sustained a first-time, traumatic anterior glenohumeral joint dislocation and wish to return to contact sports. The likelihood that these patients will sustain a further dislocation on returning to contact sports is so high that a primary stabilization procedure is recommended within a few weeks of their acute injury. An accelerated rehabilitation program following this procedure will enable these patients to return to sport in the same time frame as if their shoulder had been treated nonoperatively. However, the chance that their shoulder will sustain a further dislocation following surgery is less than 20%, compared with more than 90% for certain groups that are treated nonoperatively. 16 –18
A fundamental difference exists between the operative management of glenohumeral and SCJ dislocations, both first-time and recurrent. The chosen operative procedure—arthroscopic stabilization—is the same for a first-time dislocation and a recurrent glenohumeral dislocation, assuming that subsequent significant bone loss has not occurred. The technique described in this study to stabilize a first-time SCJ dislocation is a considerably simpler procedure than the figure-of-8 tendon reconstruction required to stabilize a recurrent dislocation.
Although none of the repairs in this series have failed, we believe that should a subsequent reconstruction procedure be required, the minimal repair and the complete bone replacement of the anchors would not significantly affect the procedure technically or influence its likely success.
This study has a number of limitations. It is a small, retrospective case series of prospectively acquired data with a relatively short follow-up. No comparative control groups were involved, such as nonoperative, surgical repair without internal bracing and internal bracing without surgical repair. No follow-up MRI was conducted to assess healing of the soft tissue repair or any accelerated degenerative changes.
Conclusion
A first-time, traumatic anterior dislocation of the SCJ is an unusual injury, and it can result in ongoing instability. The short-term results of this case series suggest that following a first-time dislocation, surgical repair of the anterior SCJ capsule augmented with internal bracing prevented the incidence of recurrent instability.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study. Rather, this study was registered with the Quality and Safety Information System of Cambridge University Hospitals Trust.